
|
|
|
|
|
|
|
|
From IS Implant to Tatum Cylindrical One
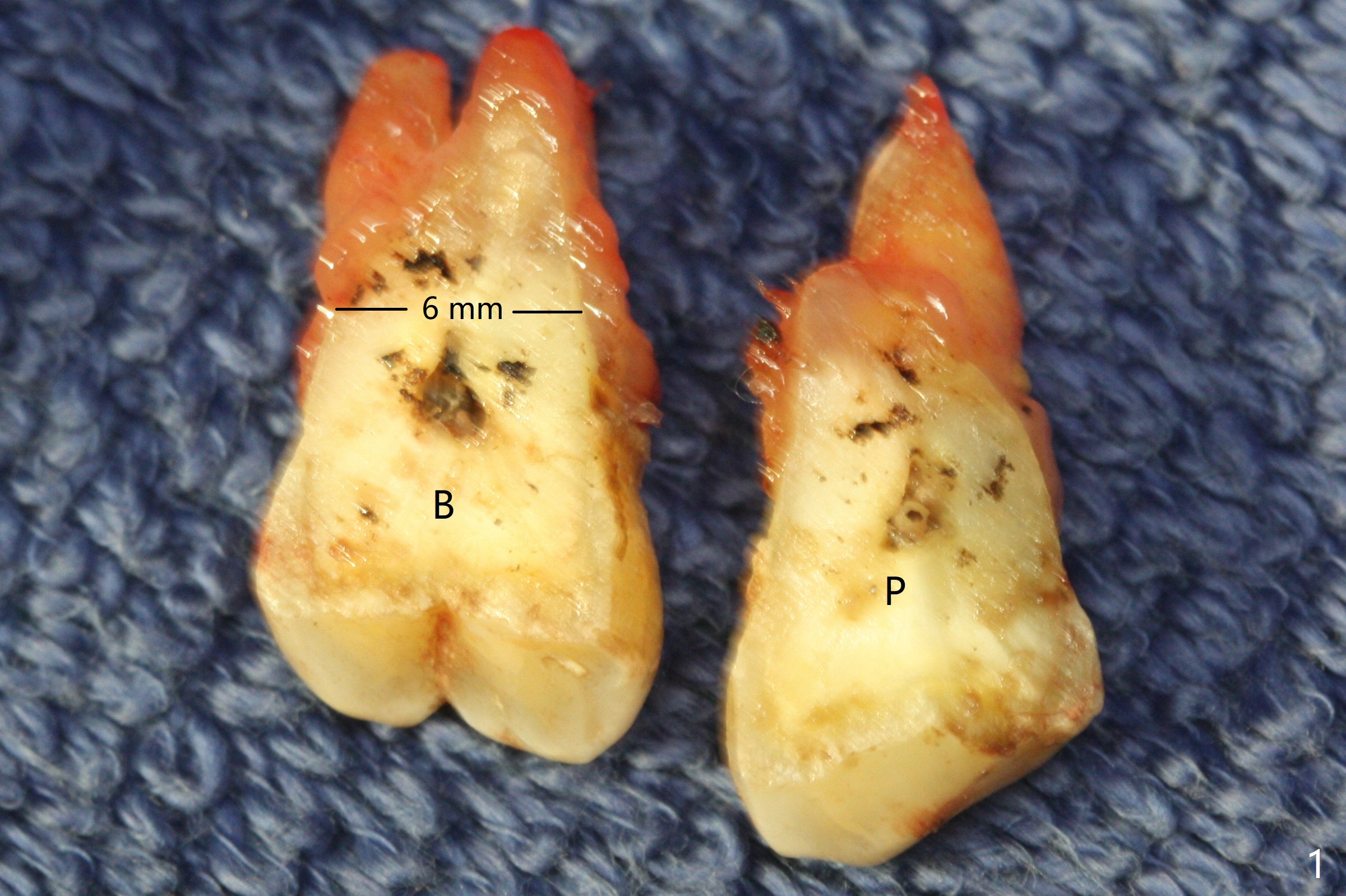
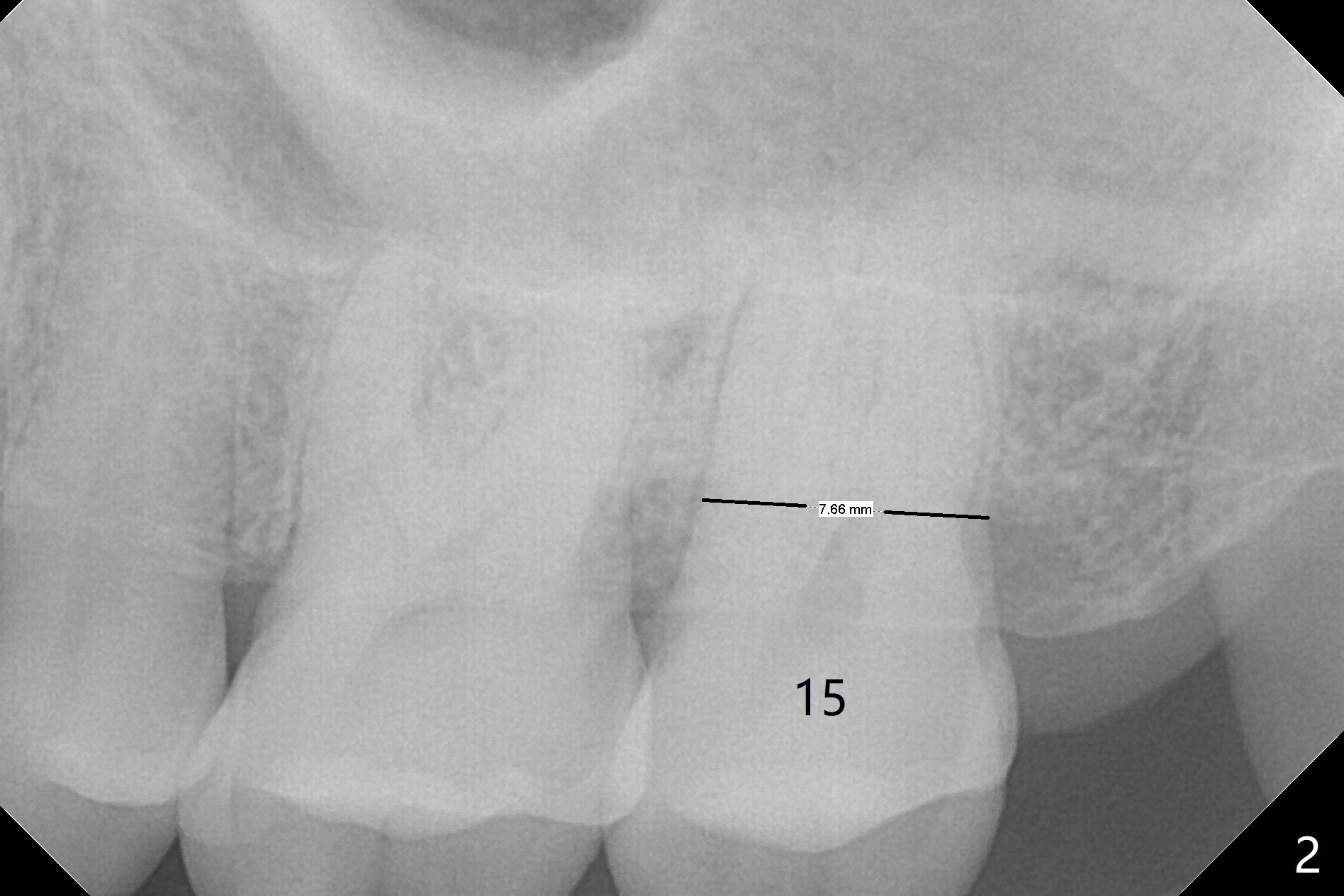
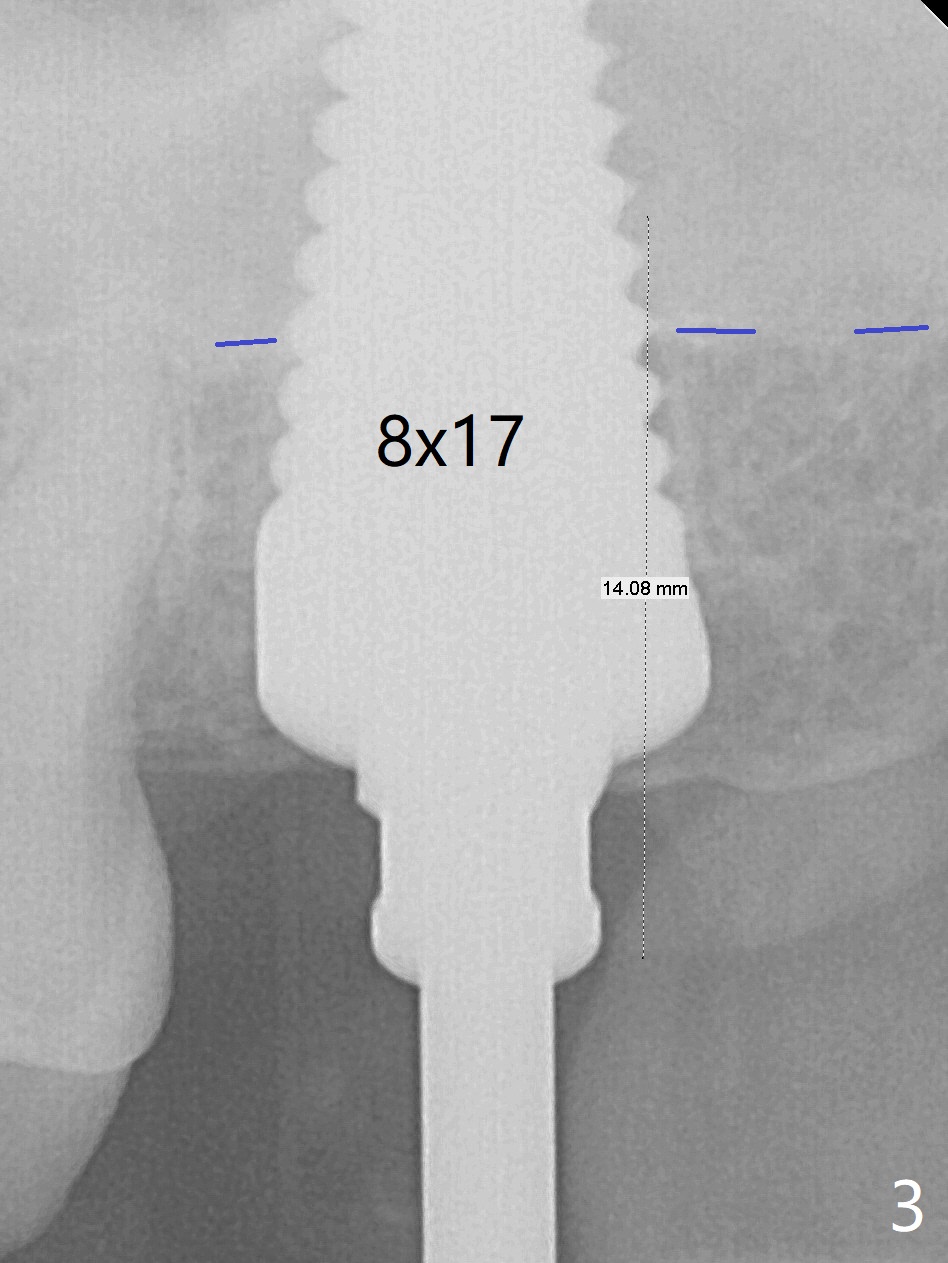
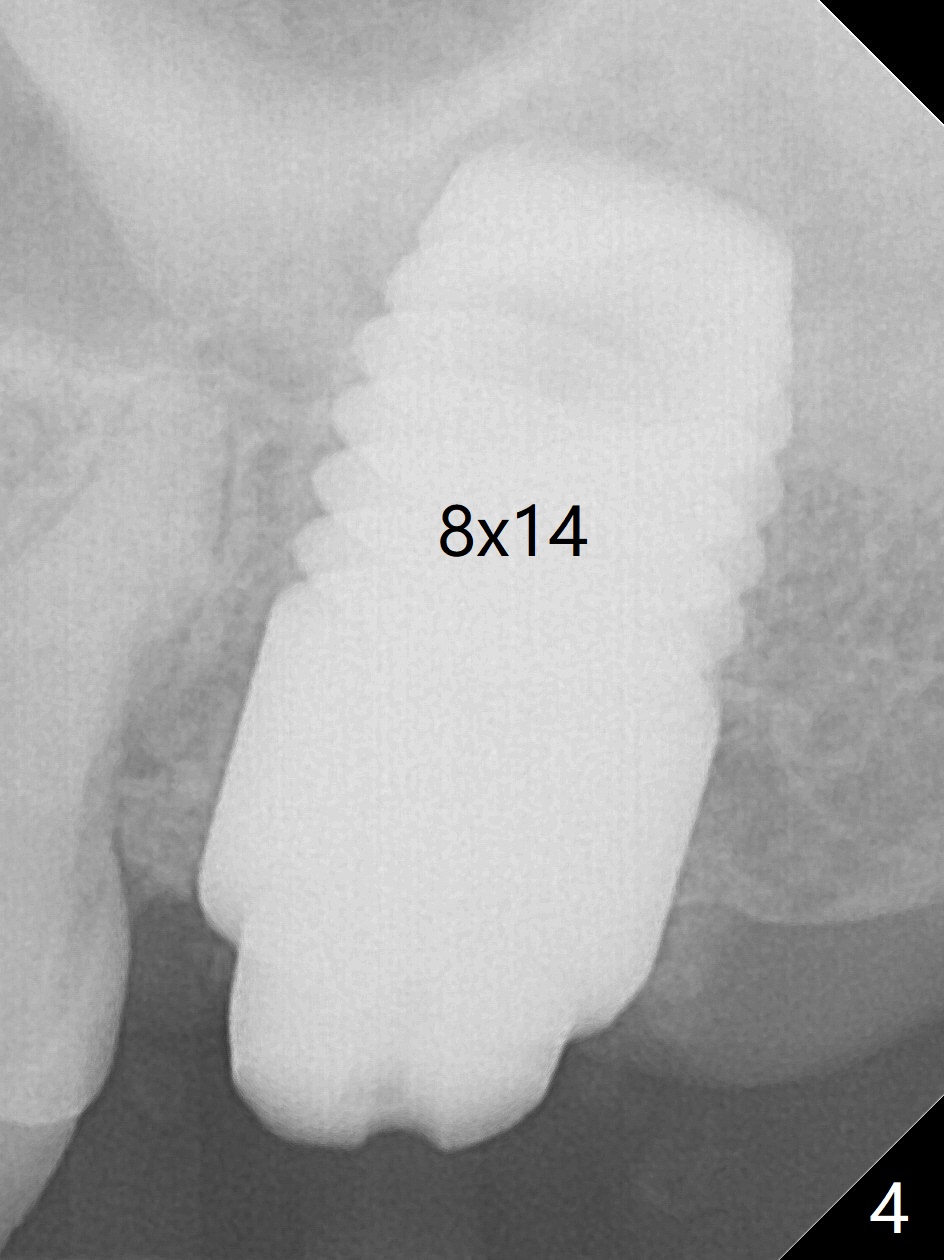
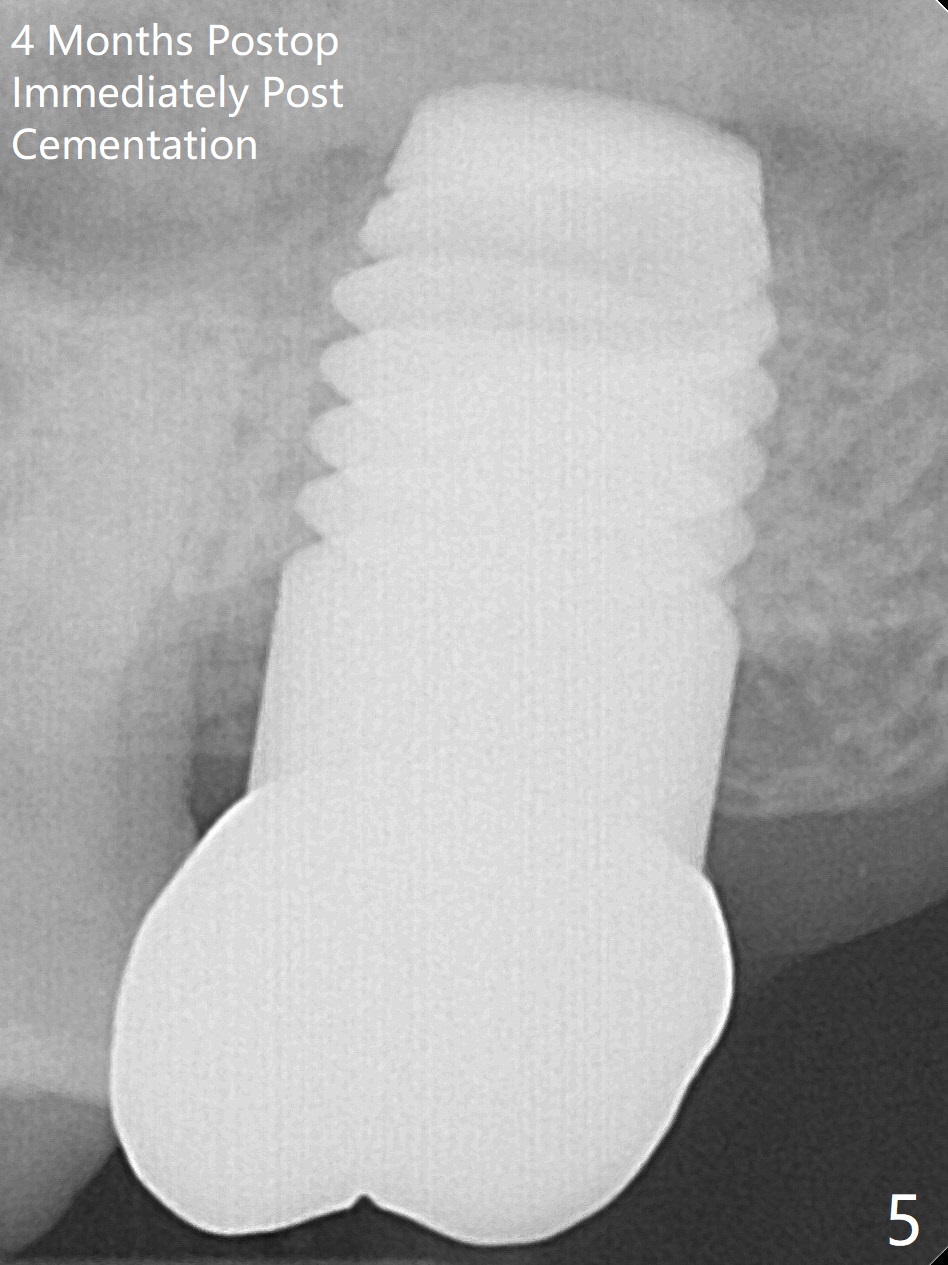
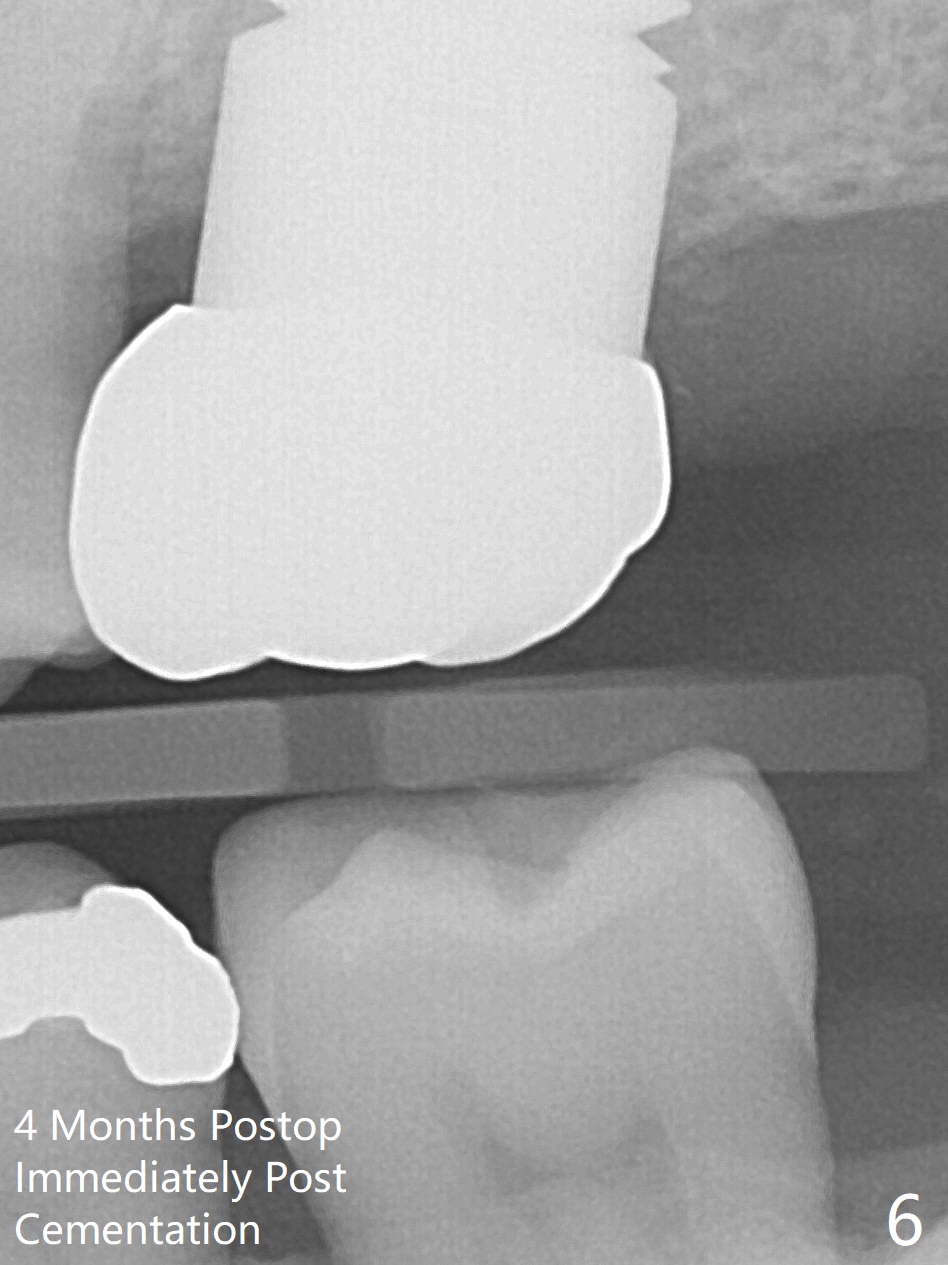
Initially the patient is reluctant to have the crack tooth extracted (Fig.1). Blood drawing for PRF fails. After extraction, the septum is confirmed to be short and thin. The bone density is moderate. When a 3.5 mm drill is being used, the osteotomy perforates into the mesiobuccal socket. A 5x10 mm IS implant achieves minimal stability. As 5.5, 6.0 and 7.0 mm cortical taps are inserted, primary stability is not obtained, as more bone is being removed at the level of the septum. When a 7x17 mm Tatum tapered tap is placed, it looks too small for the socket, as confirmed by measurement of a preop PA (Fig.2). Chronic infection associated with crack syndrome for 2 years may cause bone loss of the socket walls. Since the primary stability of a 8x17 mm tapered tap is not high (Fig.3), a 8x14 mm cylindrical implant is placed (after try in of its dummy one) with > 50 Ncm (Fig.4). The implant engages into the mesial and distal socket walls for stability. A 6x3 mm abutment is placed for an immediate provisional. In spite of difficult manipulation, the sinus membrane remains intact. Vanilla graft is placed for sinus lift and buccal and palatal gaps. Since IS implants are more or less cylindrical and if a 5 mm one does not achieve primary stability, a larger Tatum tapered tap should be tried immediately without using IS cylindrical taps. The patient returns 3 months postop, requesting early restoration before a trip to home country. The provisional has occlusal perforation. Final restoration is cemented nearly 4 months postop (Fig.5,6). The large implant makes the early restoration possible. However there is bleeding on probing palatal 1.5 years post cementation (Fig.7), suggesting palatal thread exposure. Return to Upper Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments 6 Xin Wei, DDS, PhD, MS 1st edition 05/07/2018, last revision 05/08/2021