|
|
|
|
|
|
|
|
Enough Bone for Lift? M
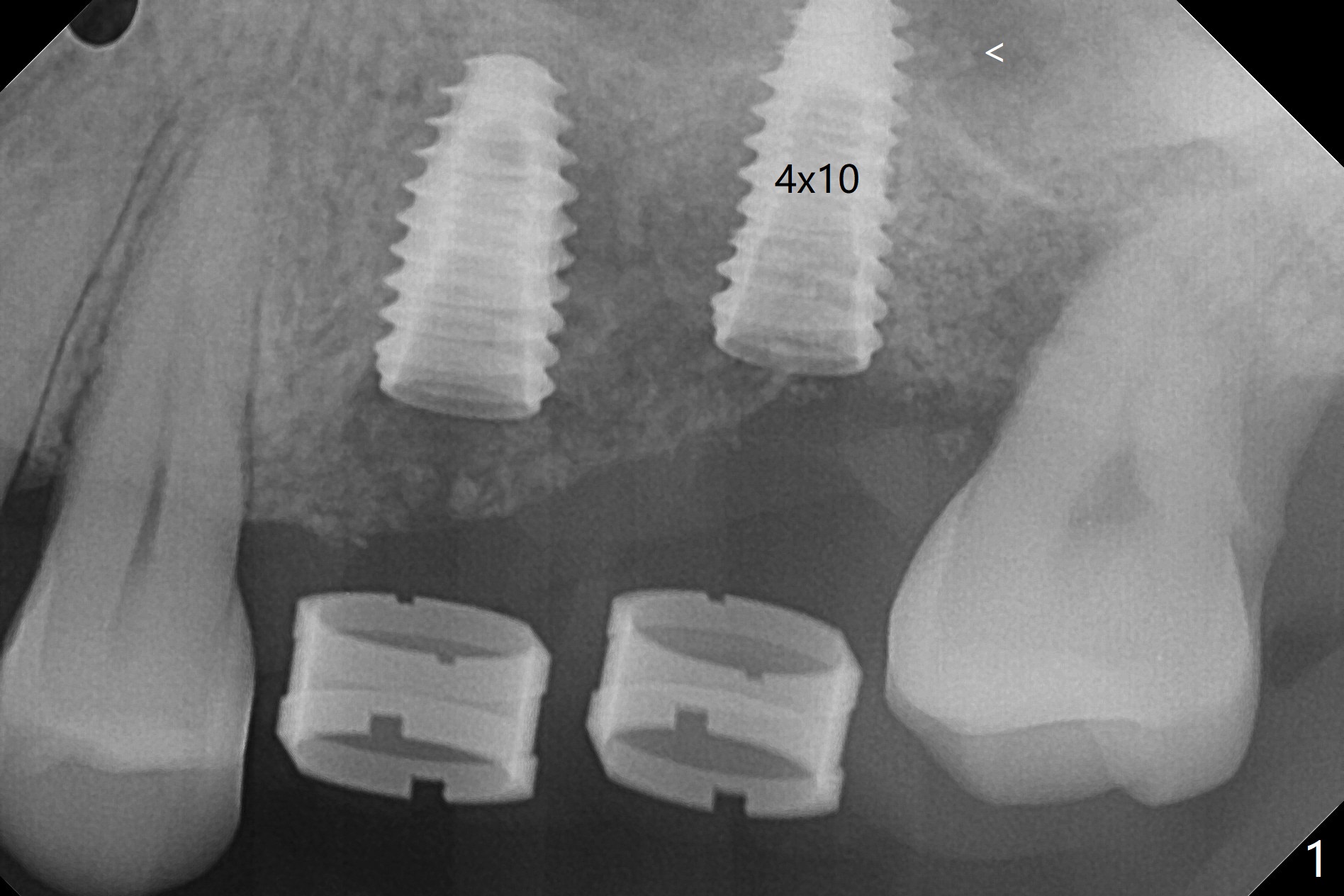
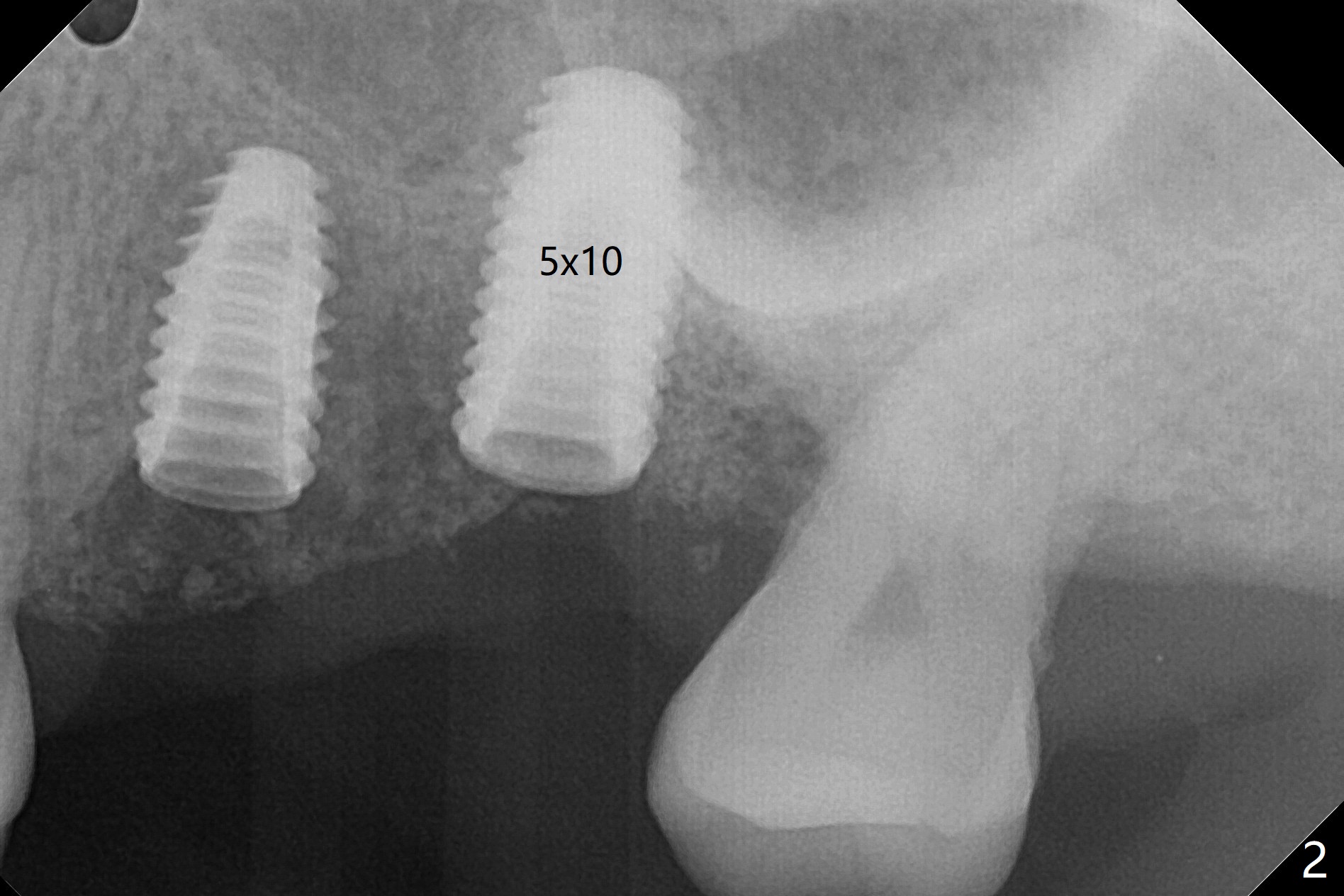
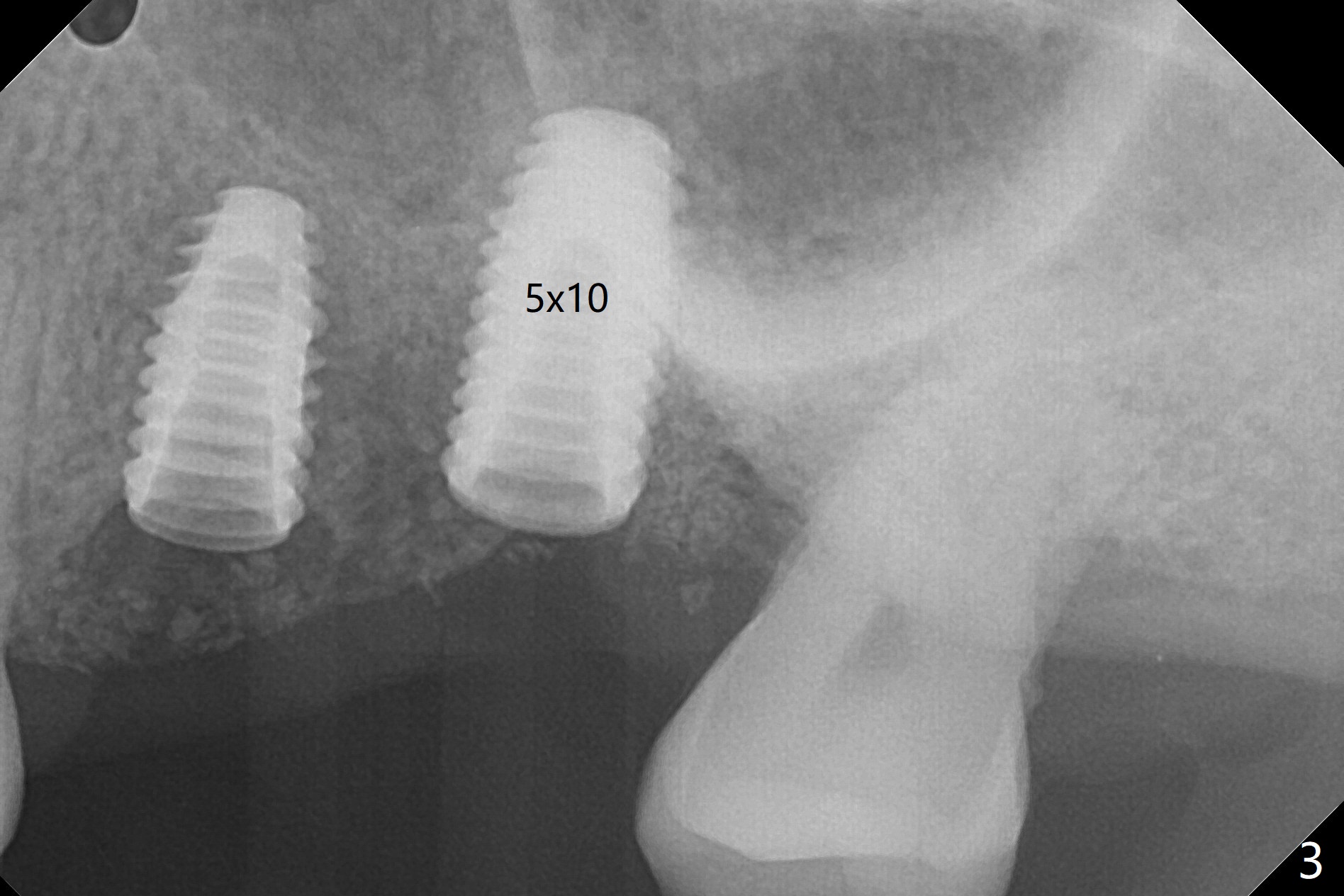
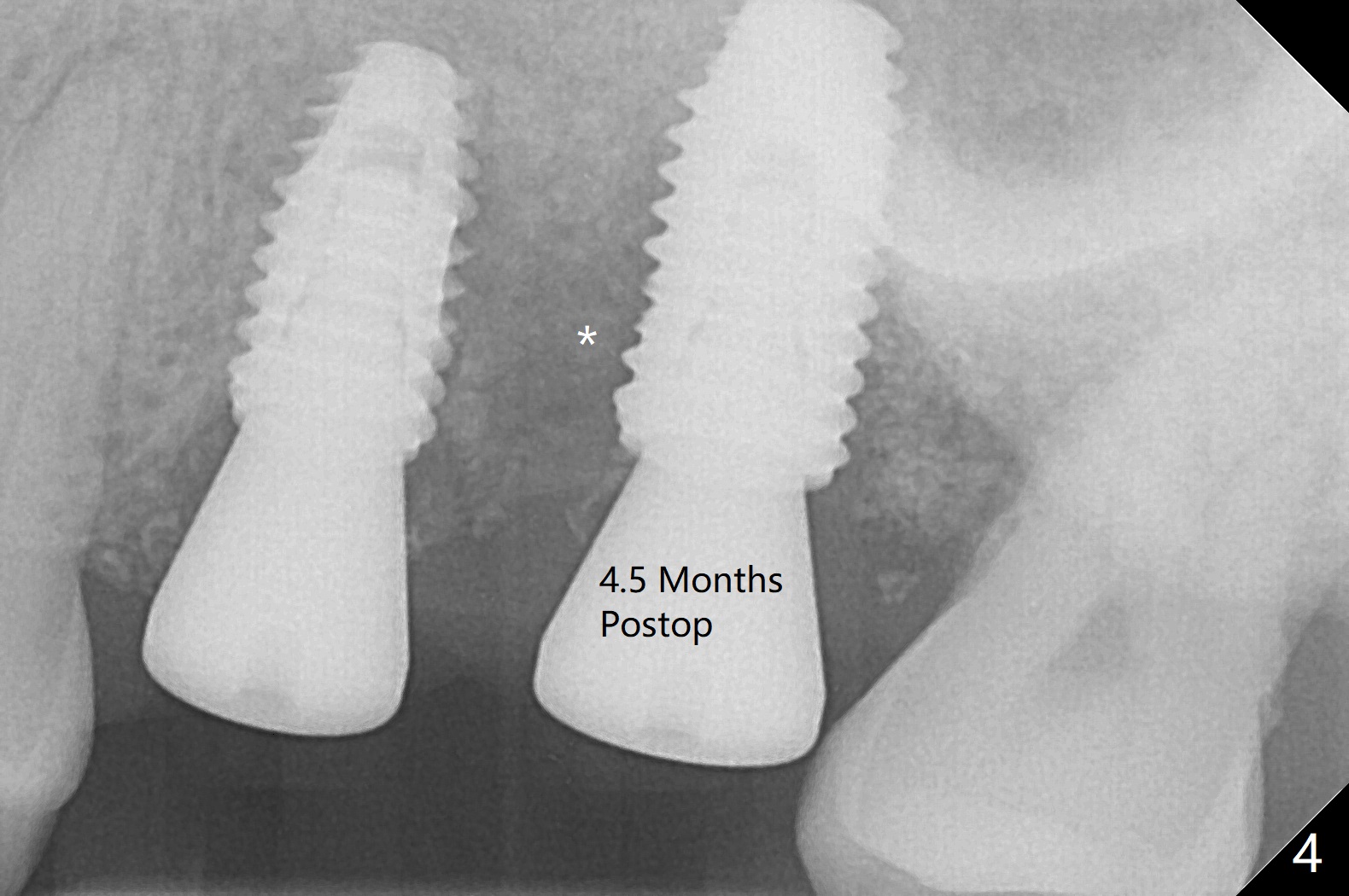
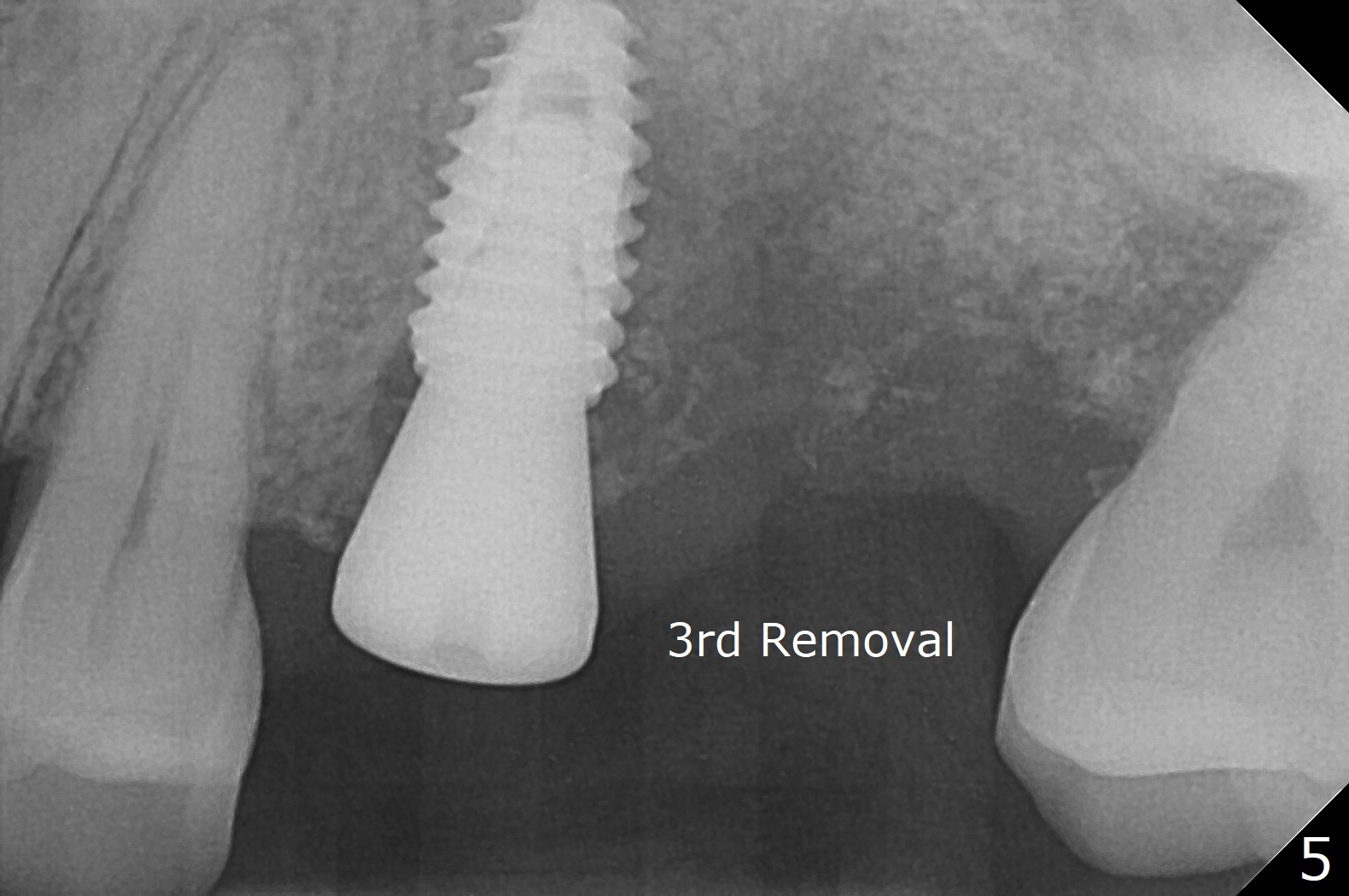
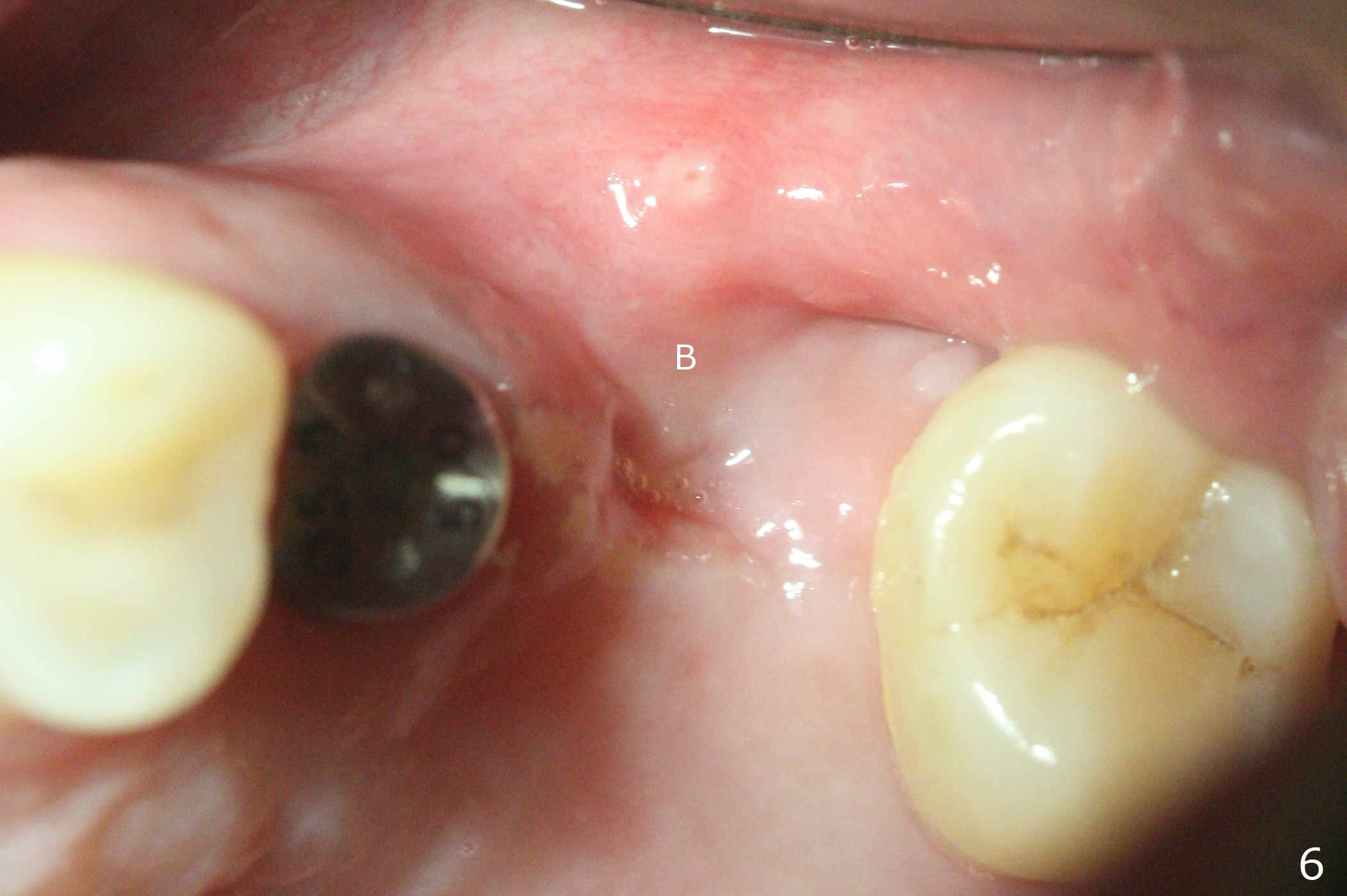
Fixture mount does not fit at #13 as an anchor. After 3.5x7.3 mm drill with 10.5 mm offset at #14, sinus lift drills (3.6x18 and 19 mm) are used. The sinus floor is intact. A 9 mm offset should be used. Following 4.0x10 mm dummy implant is placed for ~ 8.5 mm, the sinus floor is perforated while the sinus membrane is intact. After water lift, PRF membrane and allograft are inserted and pushed upward with the 4.0x10 mm dummy implant for ~ 10 mm (Fig.1). One more piece of PRF membrane and bone graft are lifted with a 4.5x10 mm dummy implant. A small dose of bone graft is elevated with a definitive implant (Fig.2,3, 5x10 mm). Is there enough bone to cover the apical part of the implant when the latter heals? When the patient returns for restoration 4.5 months postop, local oral hygiene is not good with light gingival erythema. There is tenderness when the healing abutment is being removed. It appears that osteointegraton is to occur; the mesial bone density is low (Fig.4 *). Healing abutment should be not placed when sinus lift repeatedly fails. In fact the implant is removed with the healing abutment 6.5 months postop. The buccal plate is missing, while the sinus floor is intact. Ossogen is placed, covered by Osteogen plug and sutured with PGA (Fig.5). The buccal plate remains concave 8 days postop (Fig.6 B). In the 4th trial, incision will be made, flaps dissected extensively with suture fixation. The existing guide is used to start osteotomy with point drill, followed by bone expansion. Reload the guide to place a narrower implant 4 or 4.5 mm with cover screw, and place sticky bone buccal. The latter is covered with PRF and suture. If stability is insufficient, perforate the sinus floor. Place a cemented abutment at #13 to hold periodontal dressing. Use profile drill if needed.Return to Upper Molar Immediate Implant, Trajectory II Xin Wei, DDS, PhD, MS 1st edition 08/13/2019, last revision 02/13/2021