
|
|
|
|
||
|
|
|
|
|
|
|
|
||||
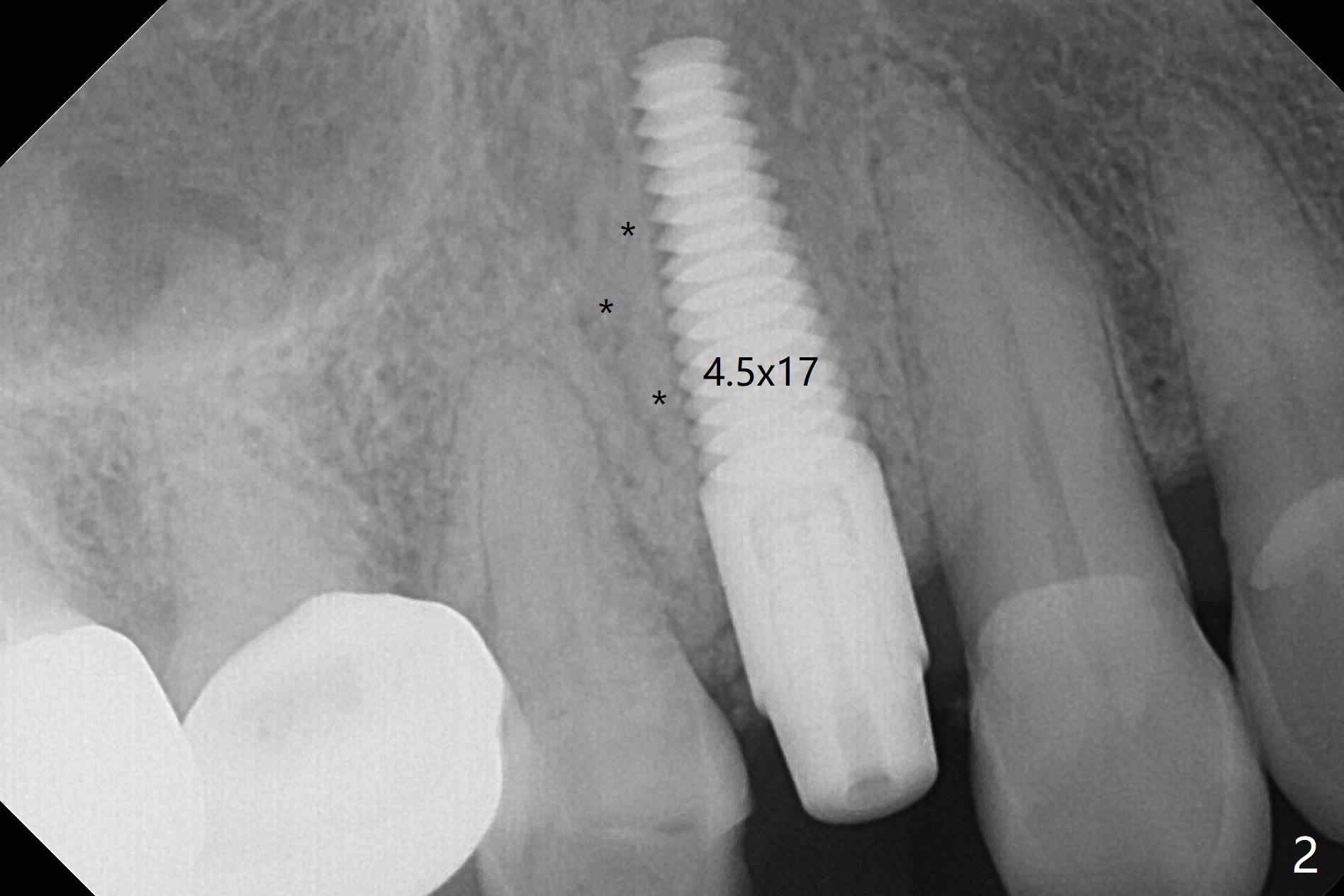
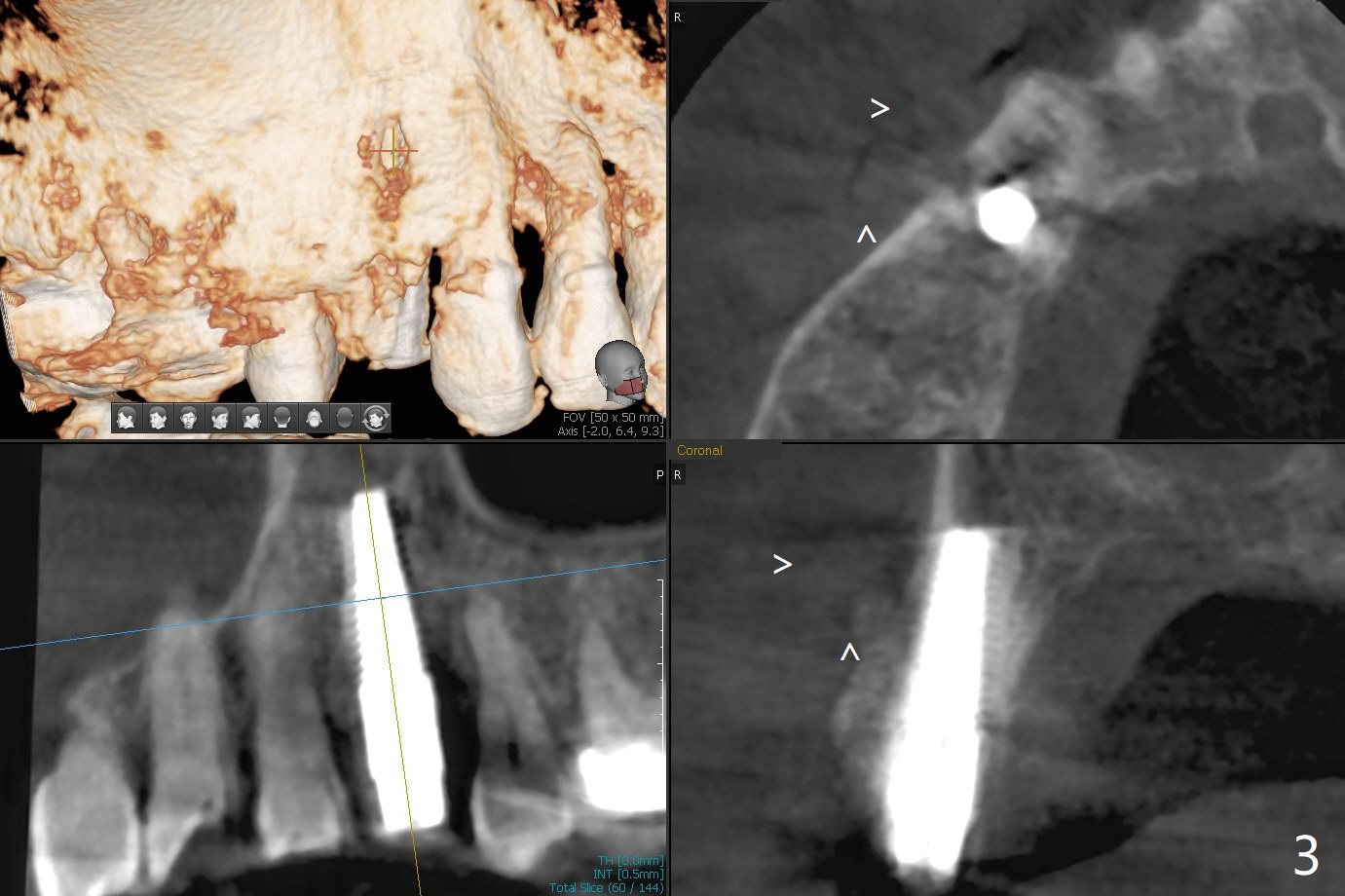
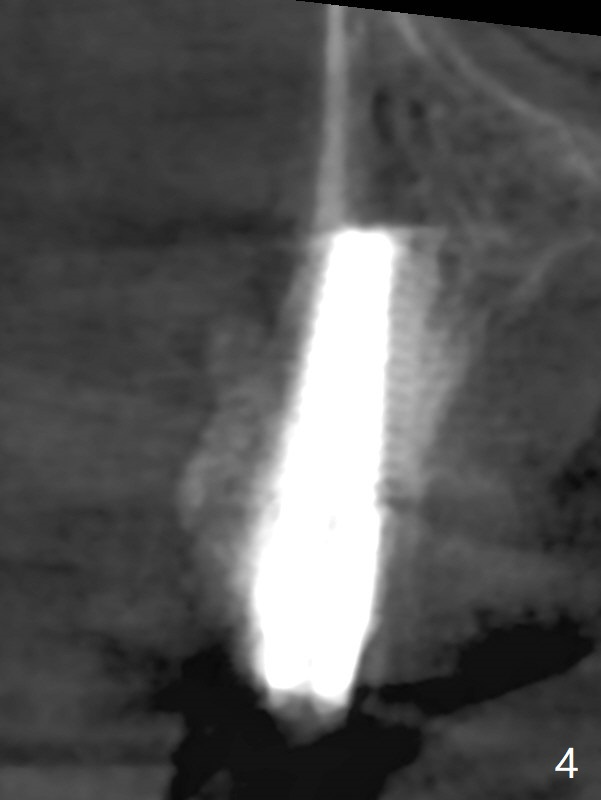
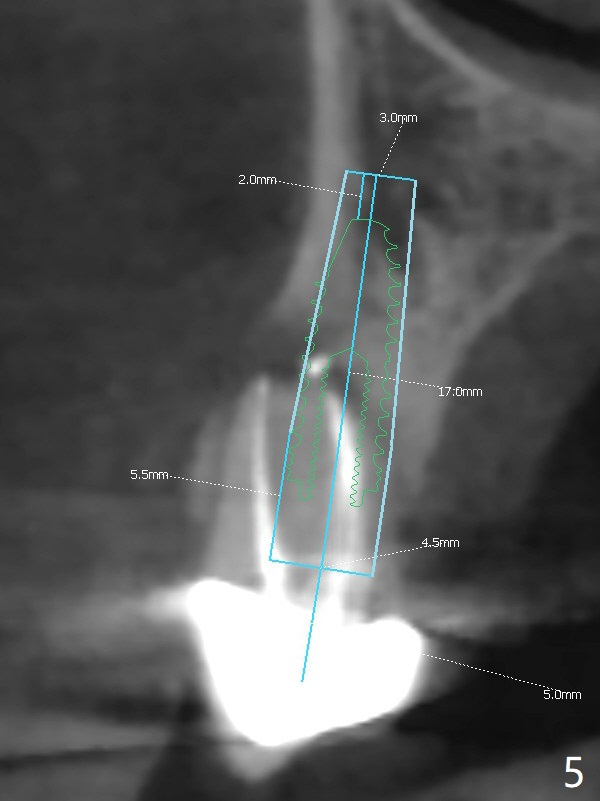
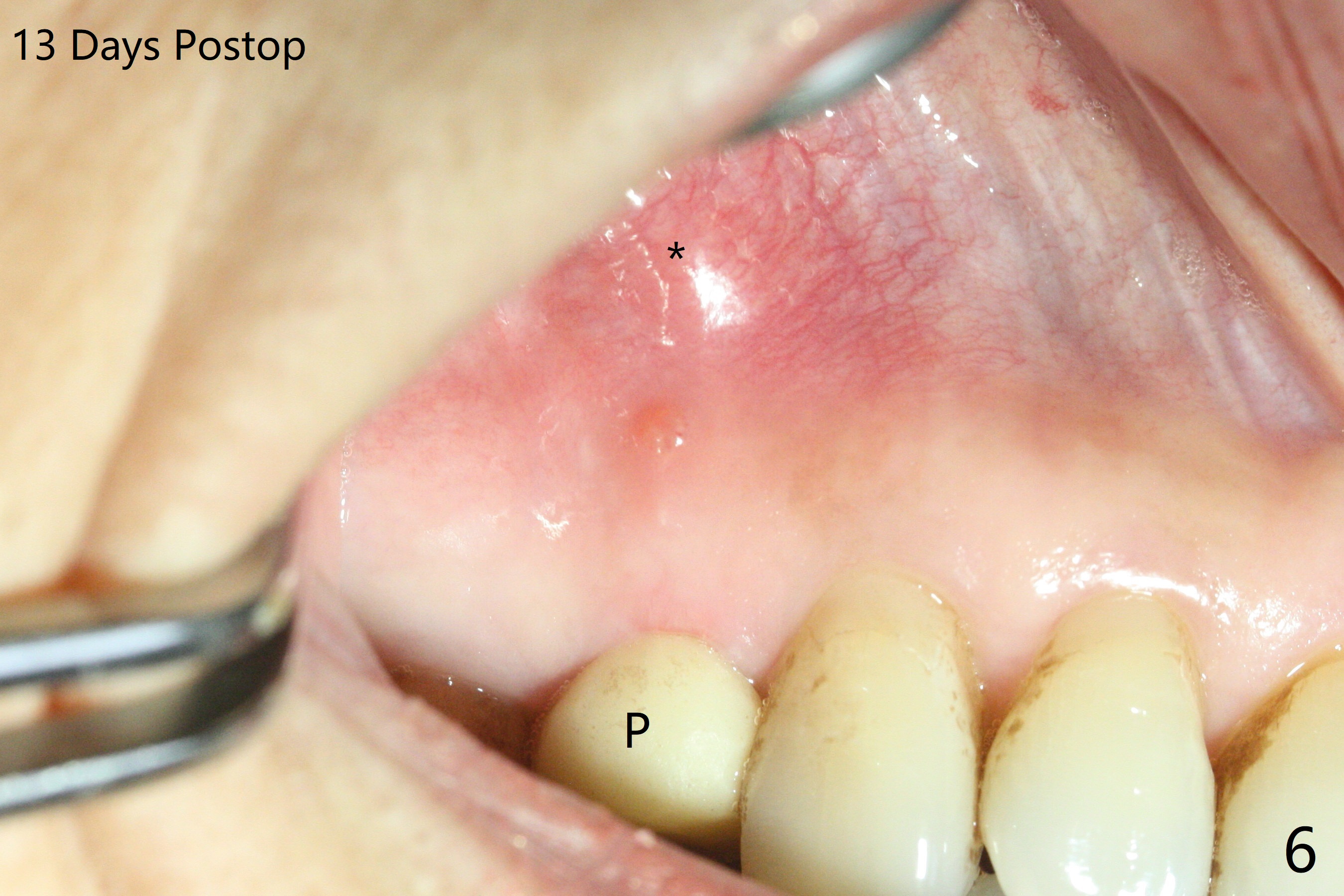
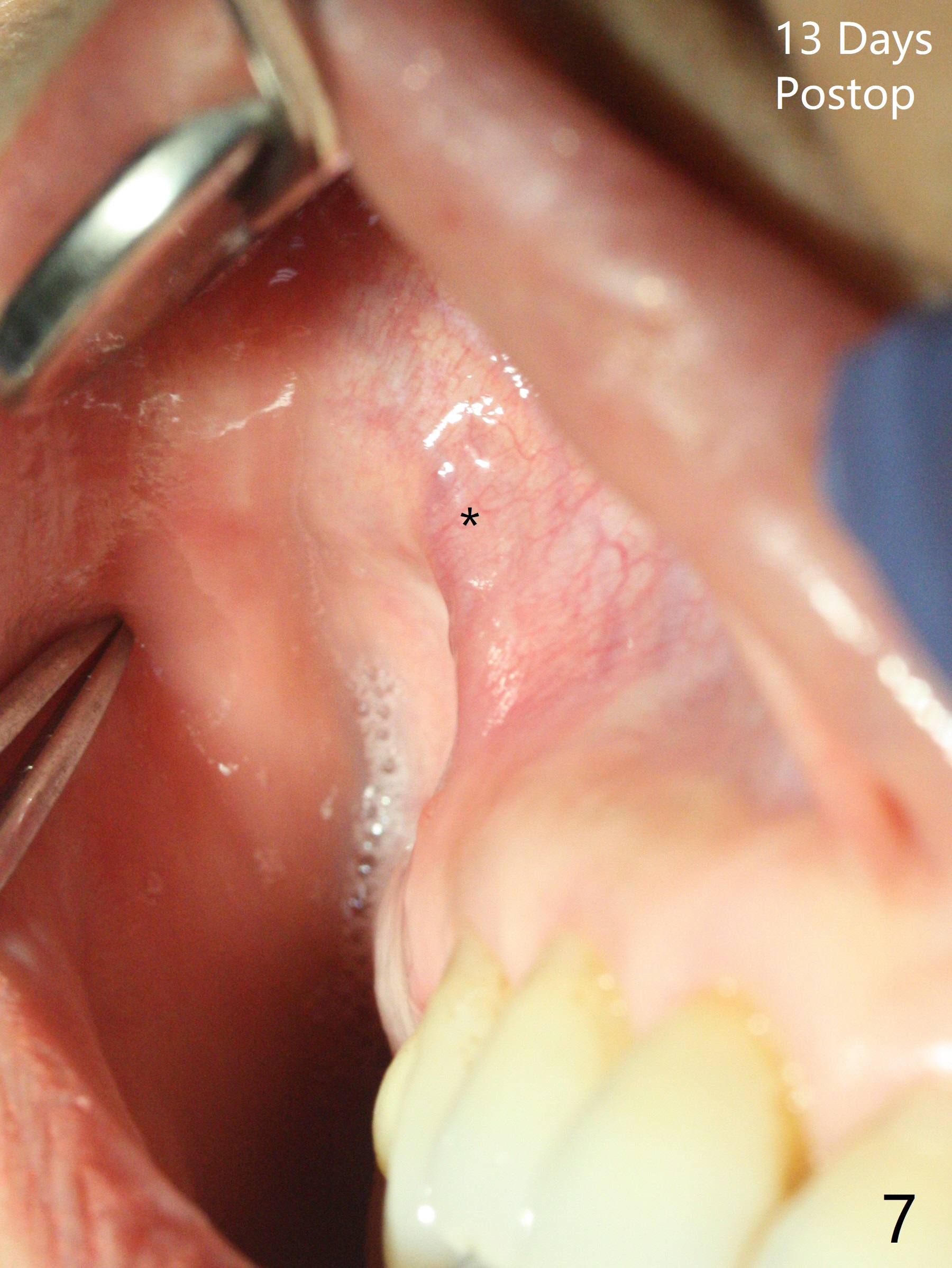
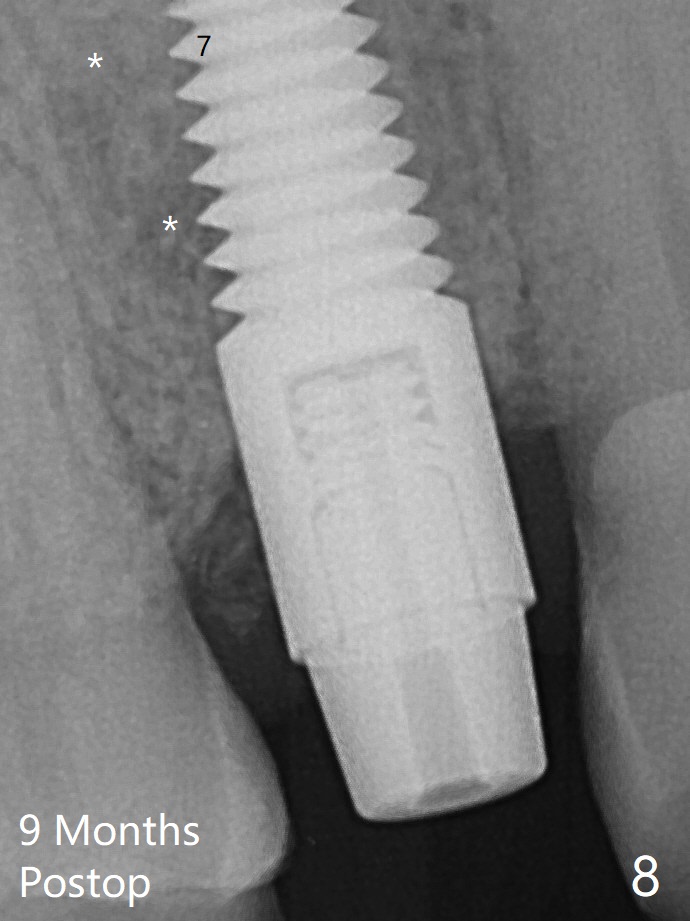
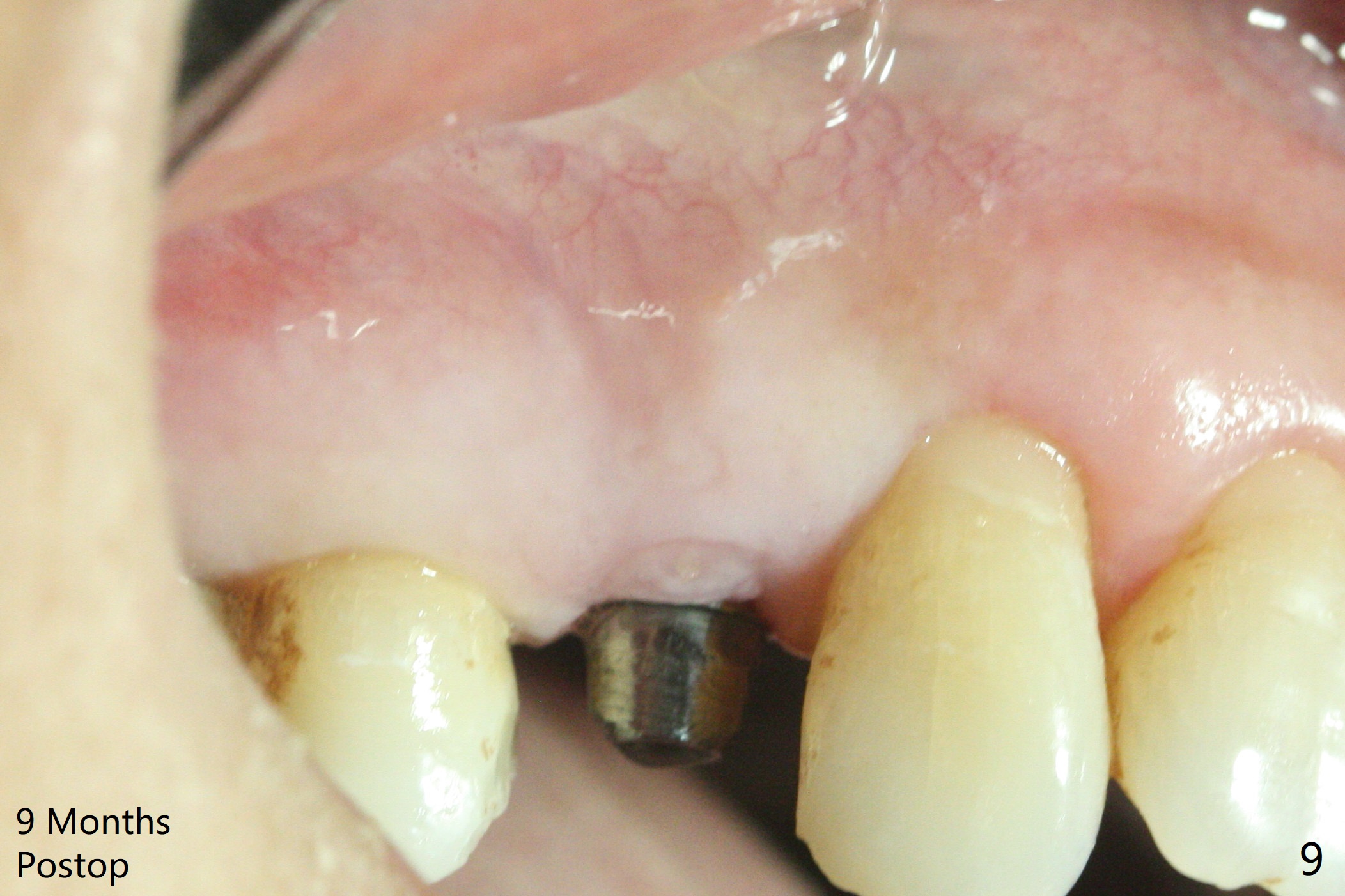
Repair Buccal Defect
After extraction of the tooth #4 with fistula (Fig.1), the buccal bony defect is superior to the fistula. Before placement of a 4.5x17 mm tissue-level implant (Fig.2) and after osteotomy for bone-level one, PRF and mixture of autogenous bone and allograft are pushed from the socket through the buccal defect for repair (Fig.3 arrowheads). The trajectory of the implant (Fig.4) is consistent with design (Fig.5). The fistula reduces in size and in redness, while the apical elevation (as related to the underlying bone graft) remains prominent 13 days postop (Fig.6,7 *). The distal defect has been apparently repaired 9 months postop (Fig.8 *, as compared to immediately post bone graft in Fig.2). The distal defect has been apparently repaired 9 months postop (Fig.8 *, as compared to immediately post bone graft in Fig.2). The fistula disappears (Fig.9).
Return to
Upper Premolar
Immediate Implant,
Trajectory II
Xin Wei, DDS, PhD, MS 1st edition
08/09/2019, last revision
05/14/2020