|
|
|
|
|
|
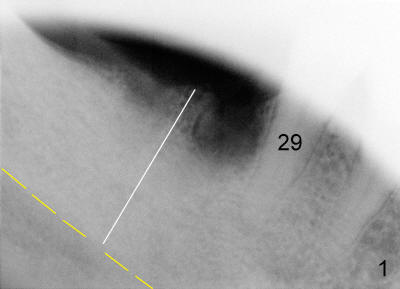
How to Avoid Damage to Inferior Alveolar Nerve
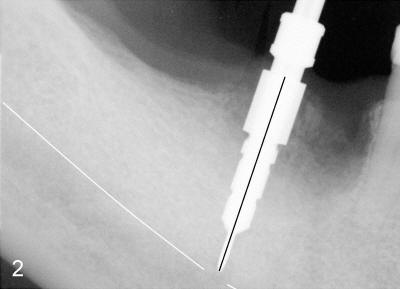
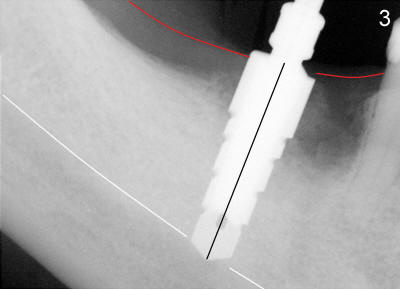
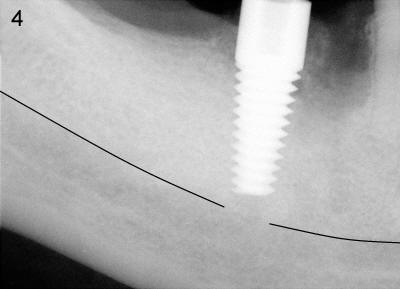
Mr. Chan is 58 years old and otherwise healthy. Three months ago, the tooth #30 was extracted due to vertical root fracture. He returned for implant placement. A pre-op PA was taken without measuring the bone height before surgery. The measurement of bone height (white line in Fig.1) from the ridge of the septum to the upper border of the inferior alveolar canal (IAC, yellow dashed line) was done postop. In fact, it is 17 mm. Effort was exerted to make osteotomy in the septum and parallel to the long axis of the tooth #29. When 2.5x17 tapered drill reached the depth, the patient felt pain. PA was taken (Fig.2). This time the invasion of IAC was overlooked again from the X-ray (Fig.2 white line). The black line indicates the length of the drill (17 mm). So far local infiltration had been used. It was thought that pain was due to incomplete anesthesia. After inferior alveolar nerve block, osteotomy was finished until 6x17 mm with combined bone expansion with Tatum osteotomes and drilling (Fig.3). The invasion of IAC was obvious. The base of the osteotomy was soft (probed with a thin curet) and the depth is more than 17 mm (explorer). Tatum tapered implant (6x17 mm) was placed 2-3 mm short of osteotomy depth (Fig.4). The tapered implant is originally designed to be placed supragingivally.
Postop, Medrol dose pak was prescribed. The patient refused to take antibiotic. As expected, the patient experienced moderate hyperthesia (pain) and mild hypothesia of the left lower lip for the first week. The symptoms improved by the second week.
The lesson learned from this case is that it is very important to take a good pre-op PA that includes IAC. Take time to trace IAC and measure the bone height. Digital image software used in this office (Cliniview) has a measurement program. It is pretty precise, with deviation not more than 1-2 mm. If you are not sure of boundary of the IAC, choose shorter drills, osteotomes and implant. Although CBCT is precise, it may be not available or indicated for every case. For a simple case such as this one, careful analysis of well-taken PA is often good and safe enough to place an implant in the posterior mandible.
Iatrogenic injury to IA nerve is stressful to both clinician and patient. As mentioned above, the symptoms of nerve injury improved by the second week. Fourteen days postop, the patient called office, complaining of sudden gum swelling and pain around the implant with formation of pus. Can you guess what happened?
Xin Wei, DDS, PhD, MS 1st edition 07/27/2011, last revision 09/03/2011