


|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|||||
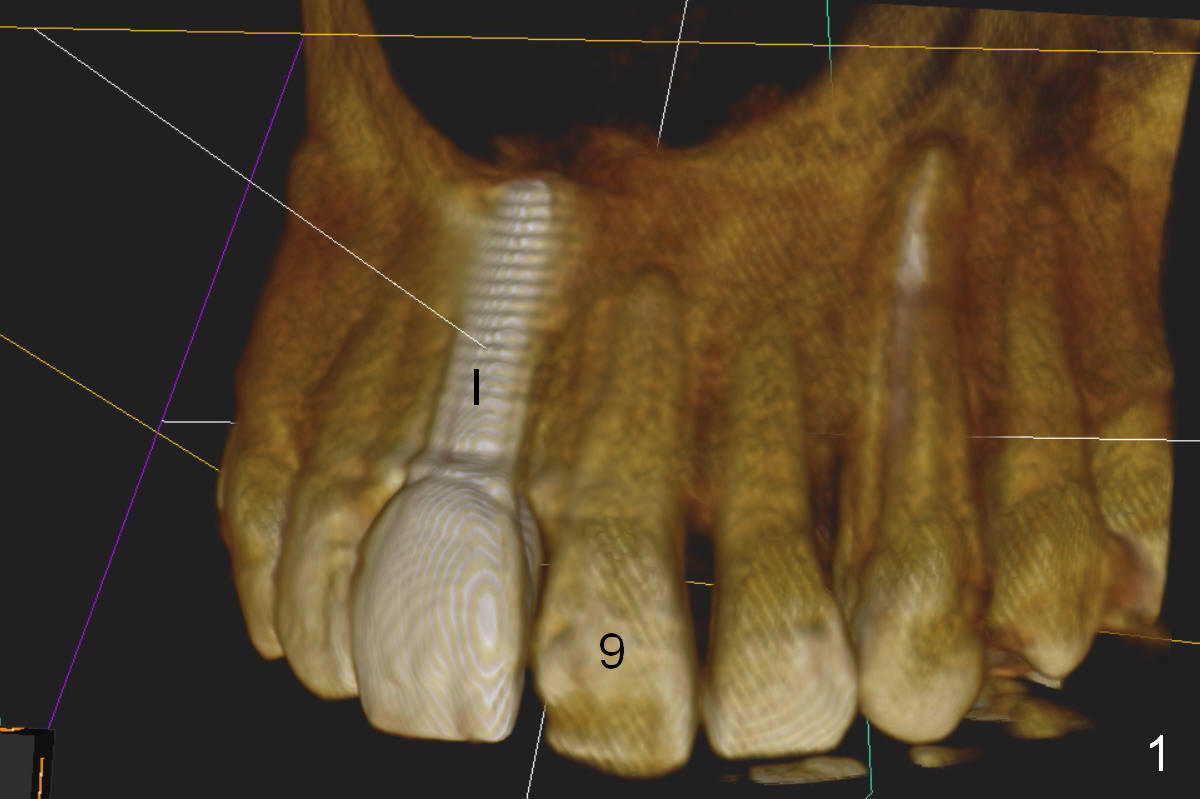
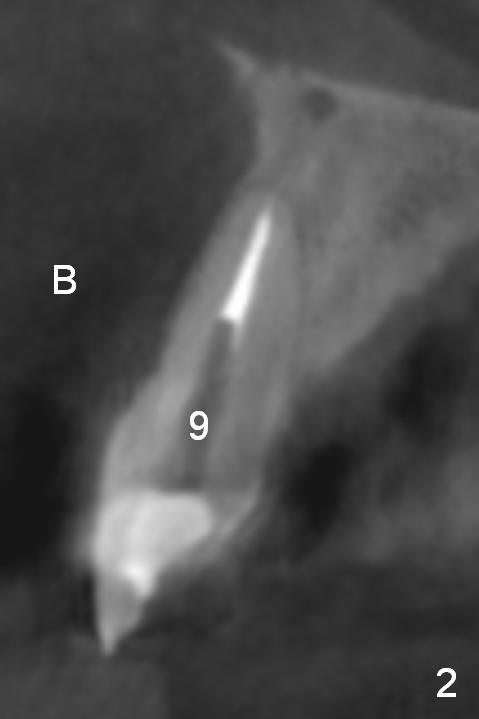
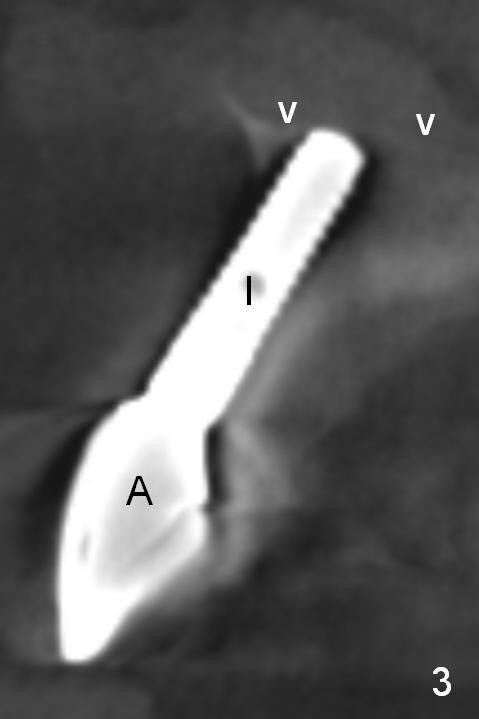
Angled Abutment and Segmental Osteotomy
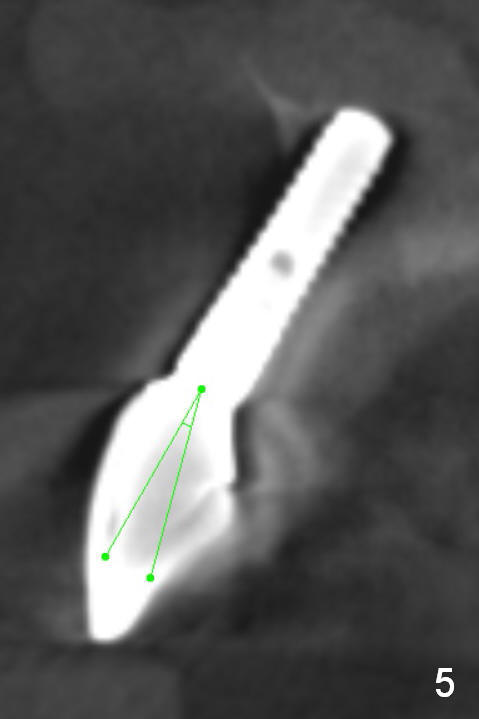
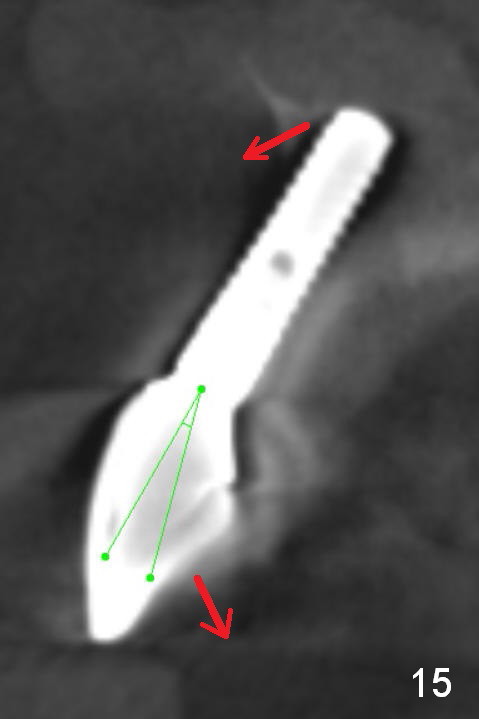
The implant at the site of #8, which was placed ~ 2 years ago, appears devoid of bone buccally (Fig.1 (CBCT 3 D image) I). Fig.2,3 are coronal sections of the tooth #9 (B: buccal) and 8 (A: Zirconium abutment), respectively. Fig.4 is a coronal section of the tooth #5 post-immediate implant with the bone plate (>, different case). With placement of a 15° Titanium abutment (Fig.5 palatal green line), the crown profile may improve.
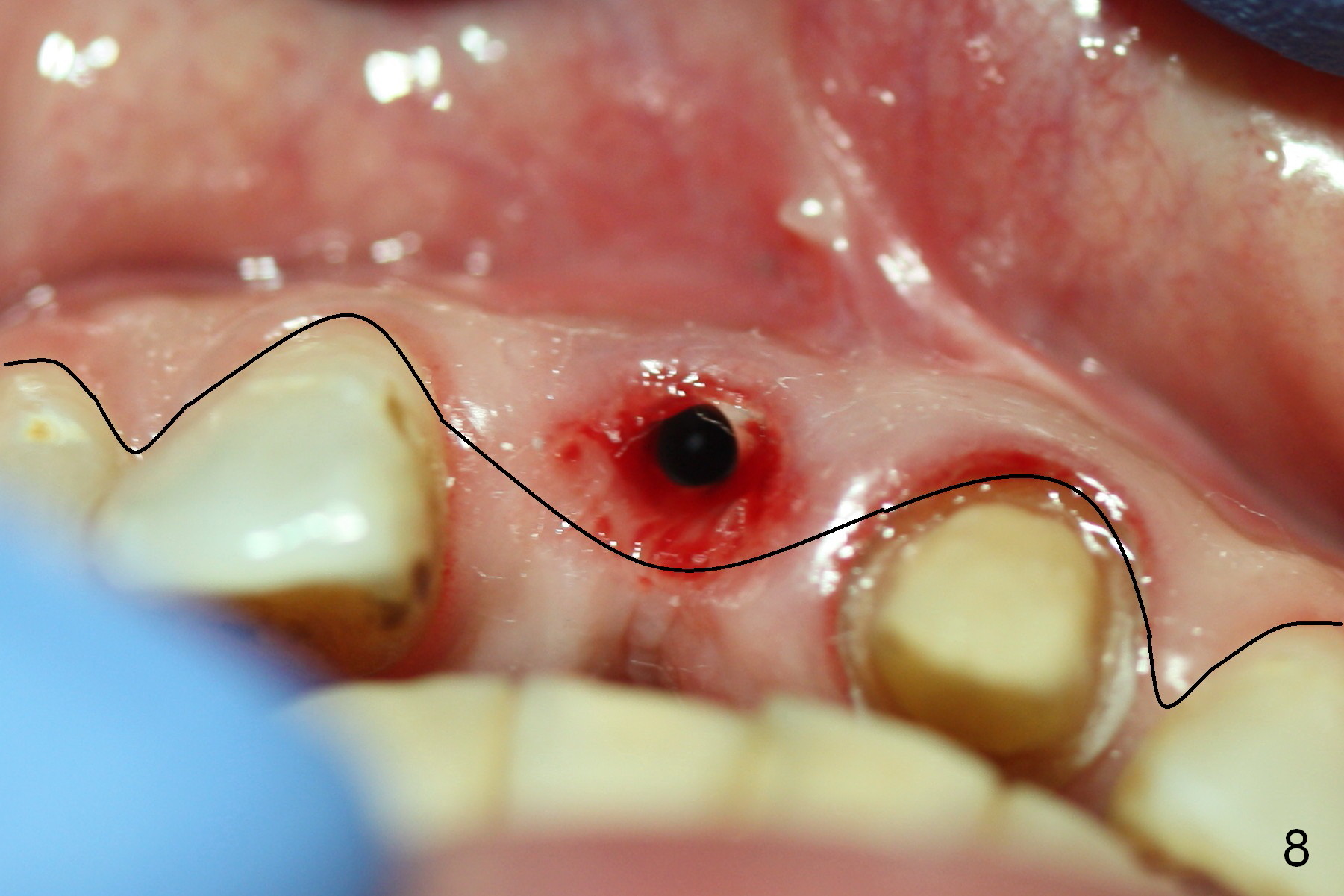
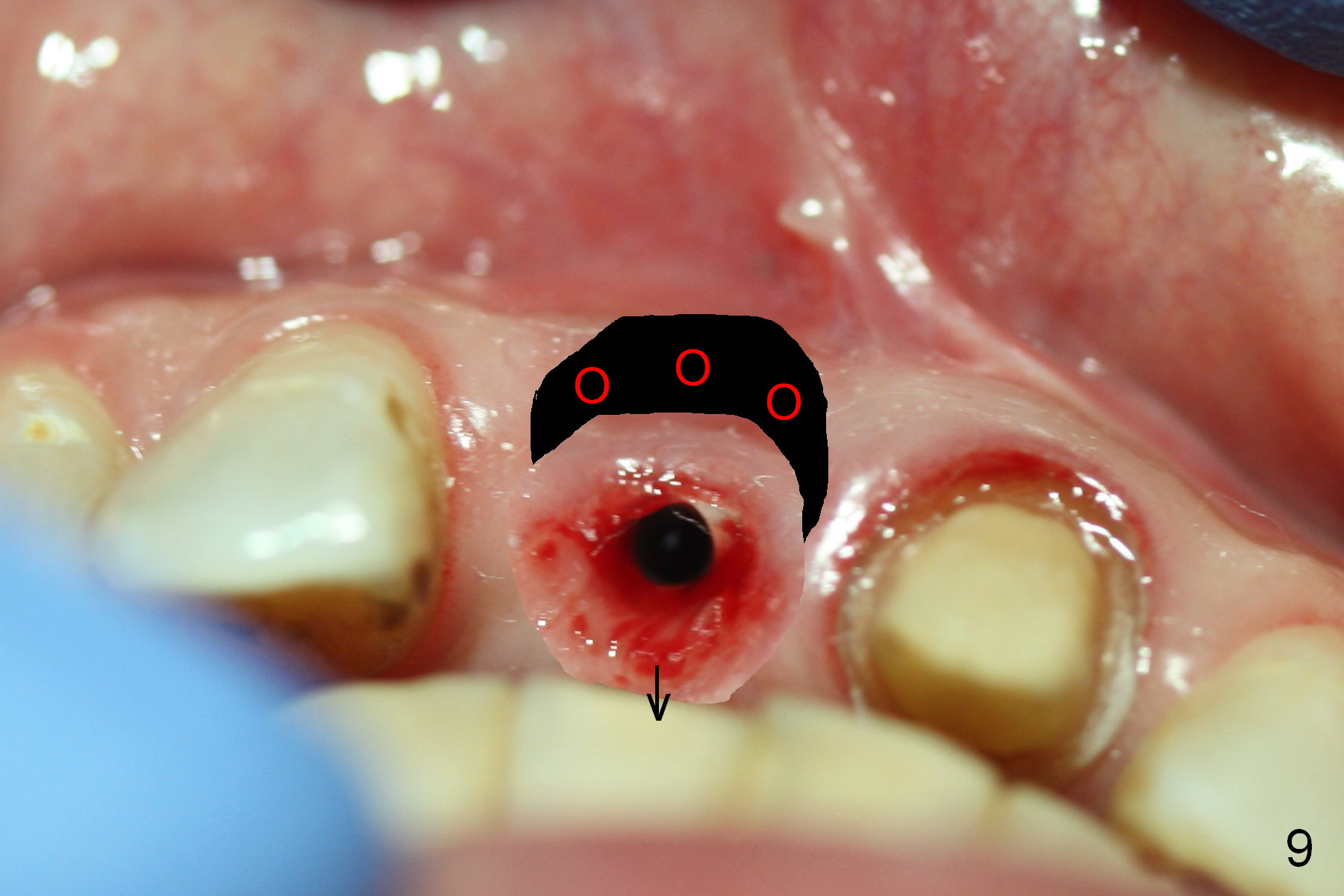
Fig.6,7 were taken a month ago when the Zirconium abutment was fractured, showing the position of the coronal end of the implant. To retrieve the abutment, an envelop incision will be made (Fig.8) with elevation of the buccal flap for the best visibility. Prepare abutment removing drivers (x3) and try in vitro. To improve cosmetics, the implant/bone segment seems to be required to be lingualized ~3 mm (Fig.9 arrow) with bone graft buccally (red circles, possibly chin graft).
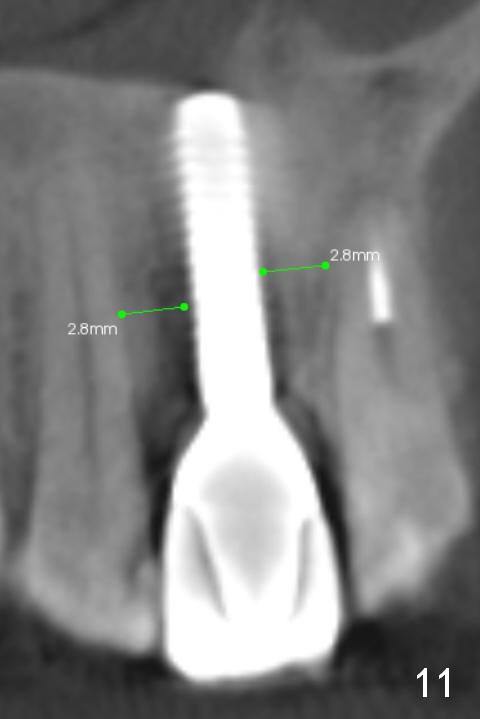
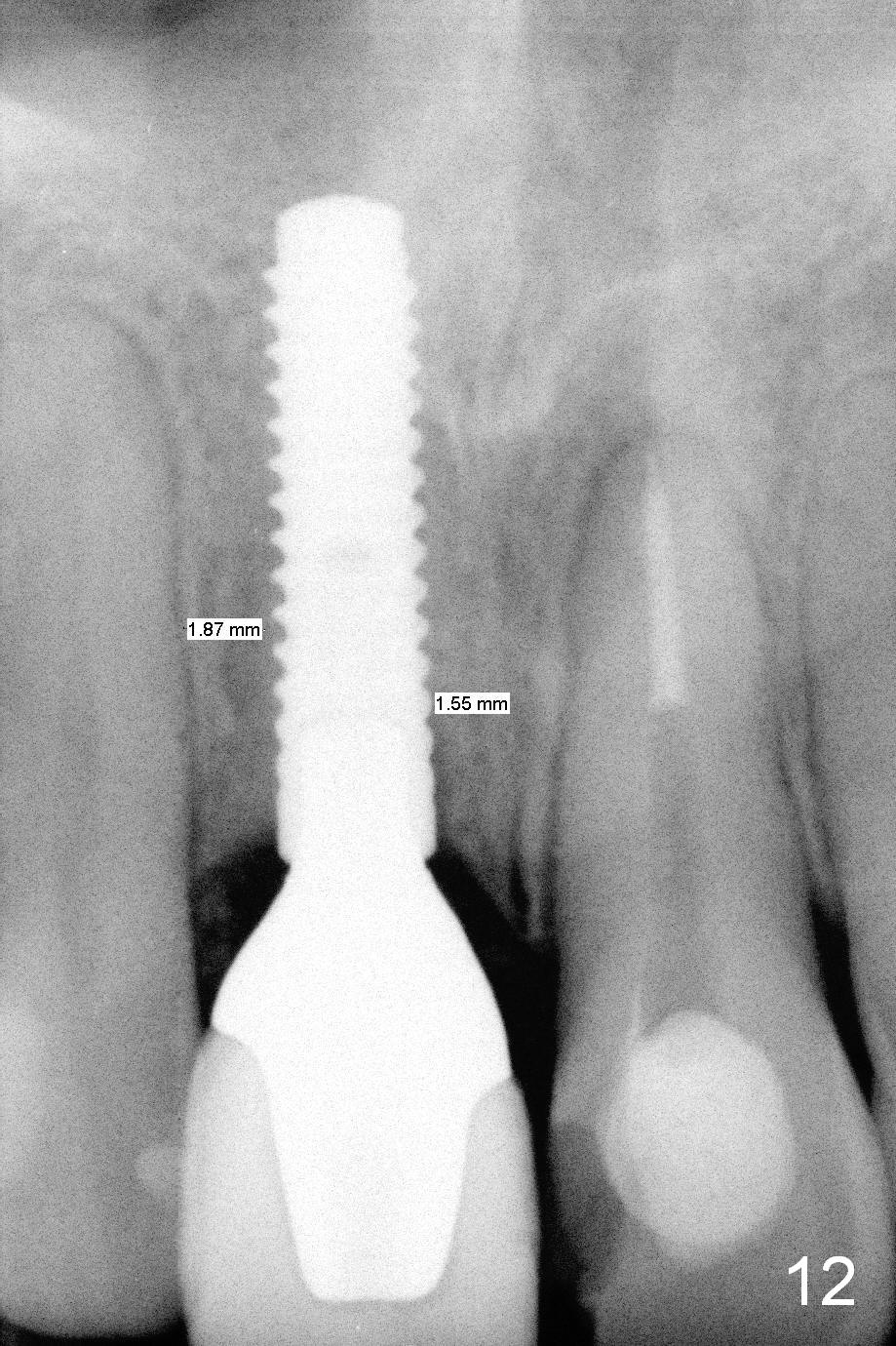
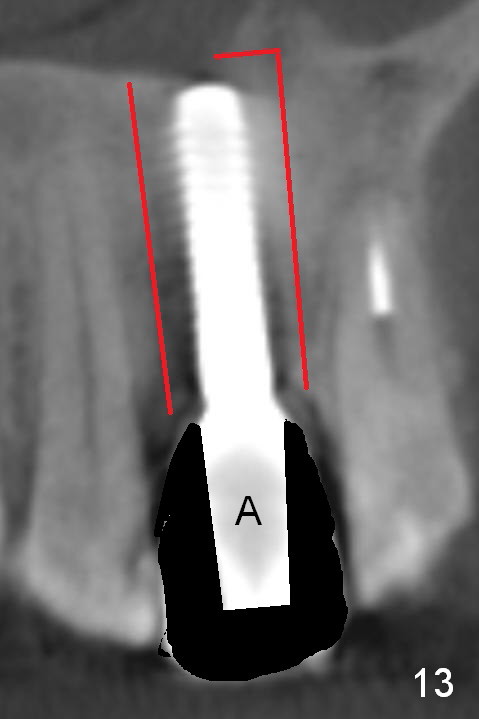
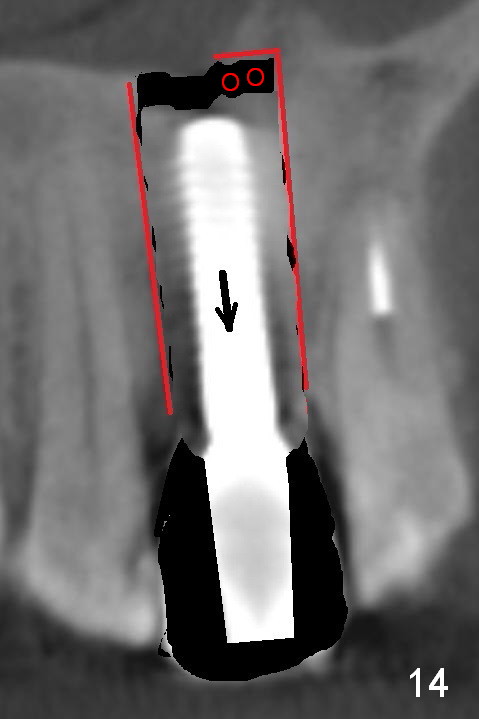
Fig.10 is a sagittal section of the implant (arrowheads: nasal floor). It is apparent that there is enough space (Fig.11,12 (PA)) for osteotomy (Fig.13 red lines: A: angled Titanium abutment). With the palatal mucoperiosteal flap attached the implant/bone segment, it is moved apically (Fig.14). Coronally the coronal portion is repositioned palatally while the apical portion buccally (Fig.15 arrows). Is the segment stable?
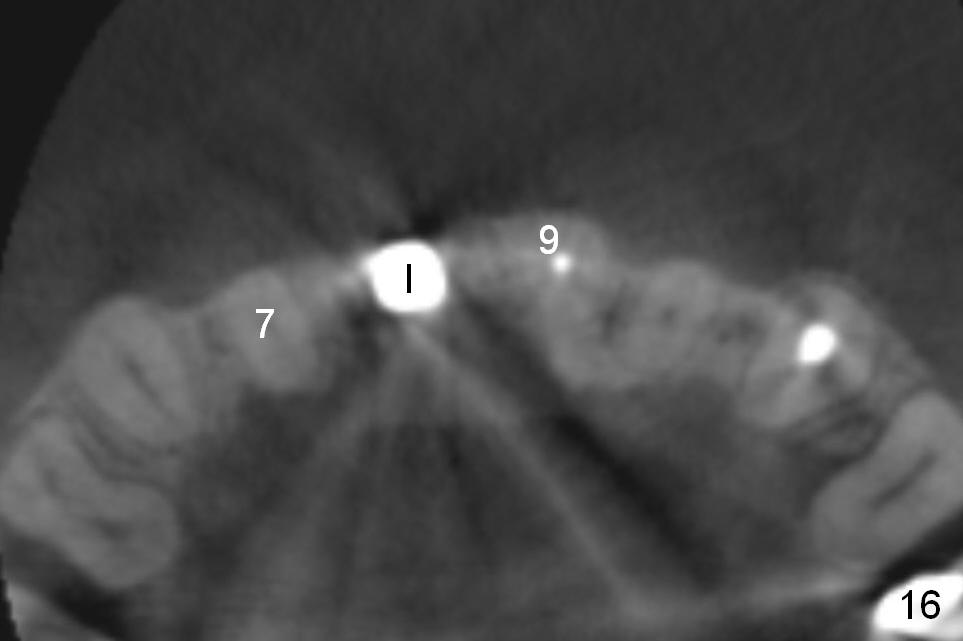
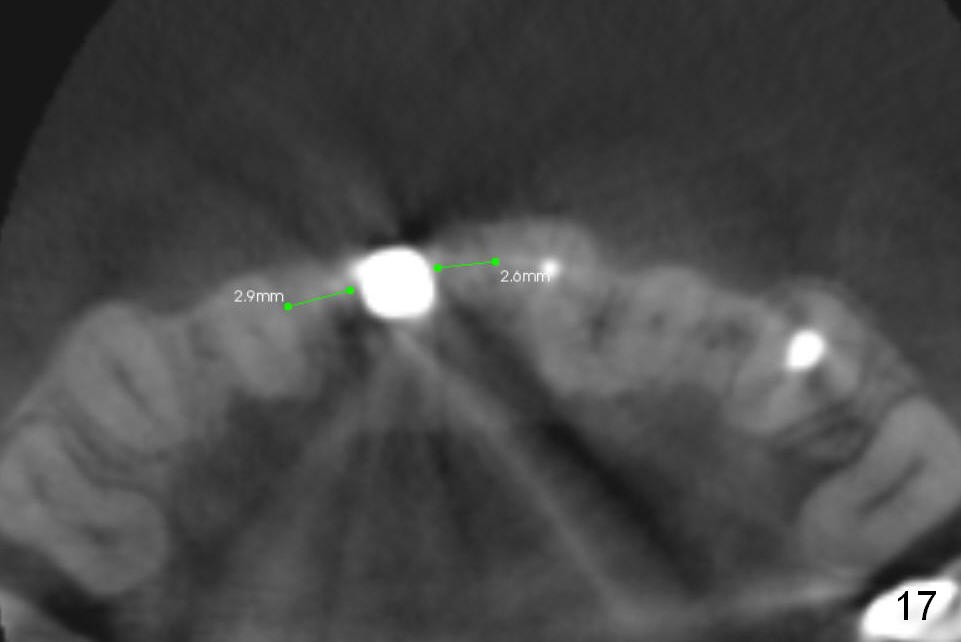
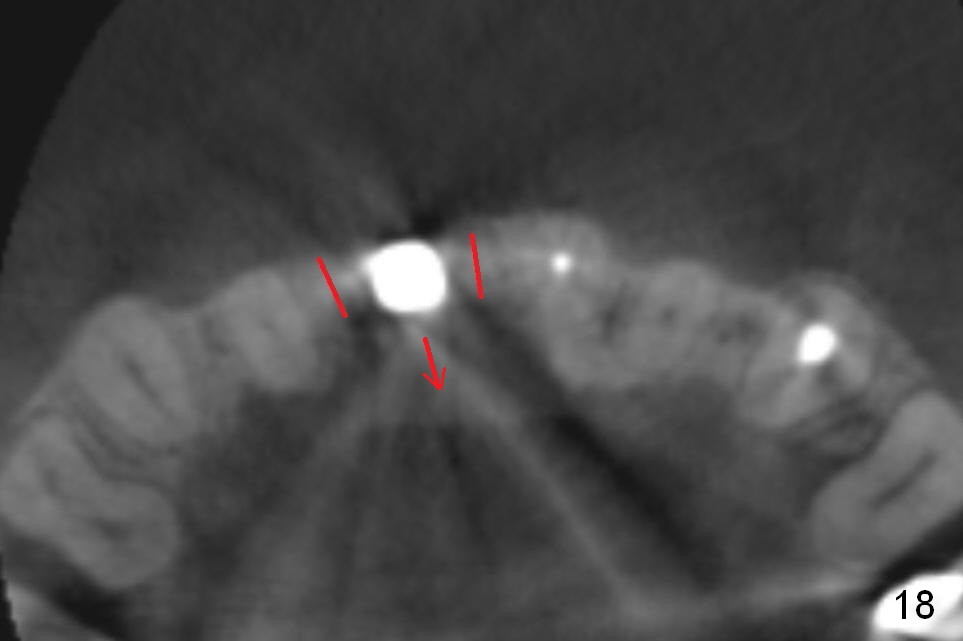
Fig.16 is an axial section of the maxilla. There is sufficient space (Fig.17) for osteotomy (Fig.18 red lines) for repositioning (Fig.18 arrow).
It appears that there is not enough bone left for a new implant to be placed if the existing one is to be removed (Fig.3,5,15). What is the most likely to be seen at surgery?
Return to Professionals,
Upper Incisor Immediate Implant, Chinese
Xin Wei, DDS, PhD, MS 1st edition 02/28/2015, last revision 09/17/2017