











|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
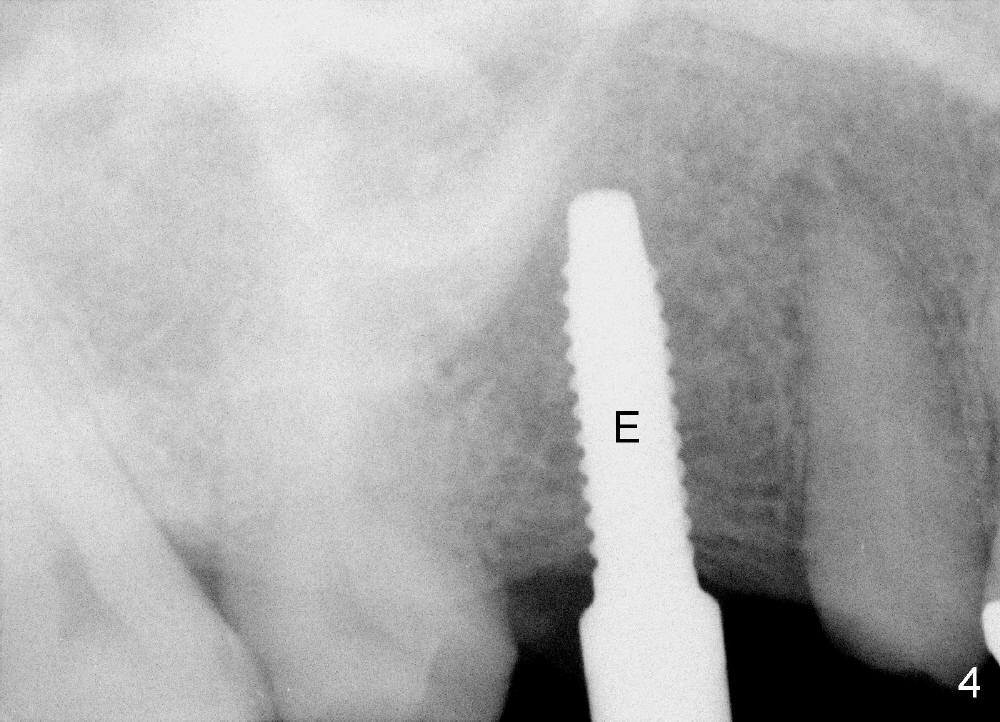
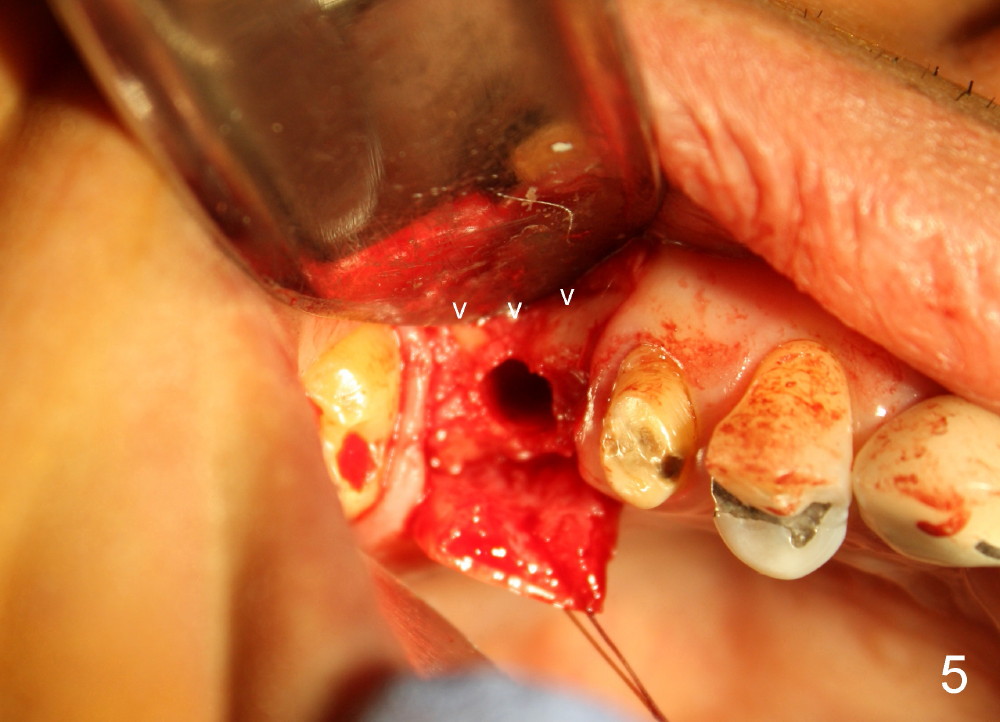
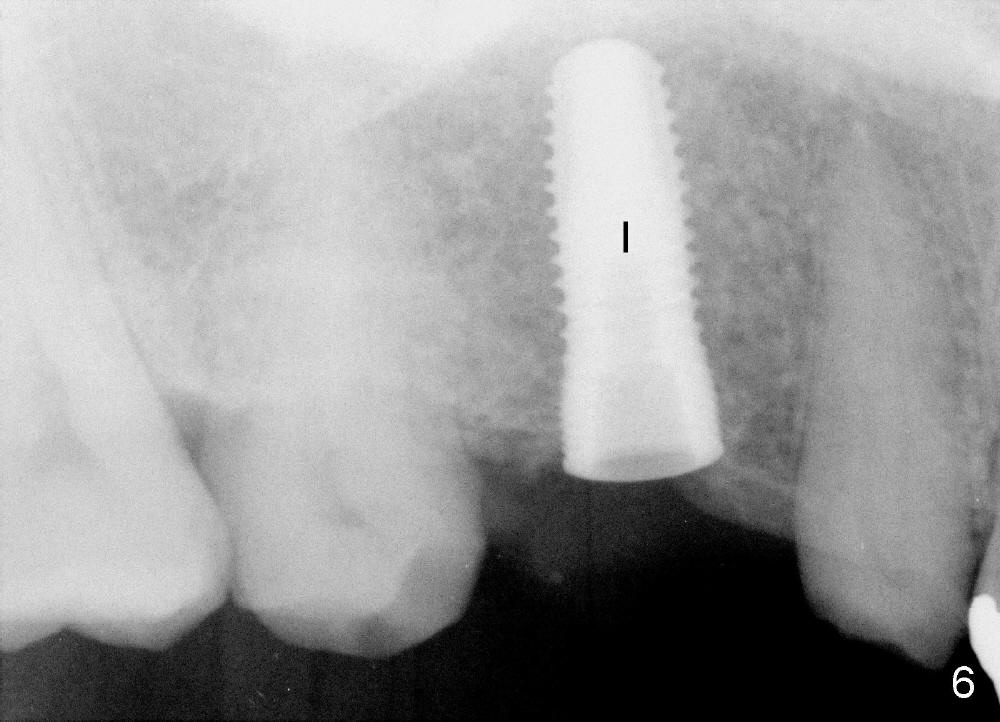
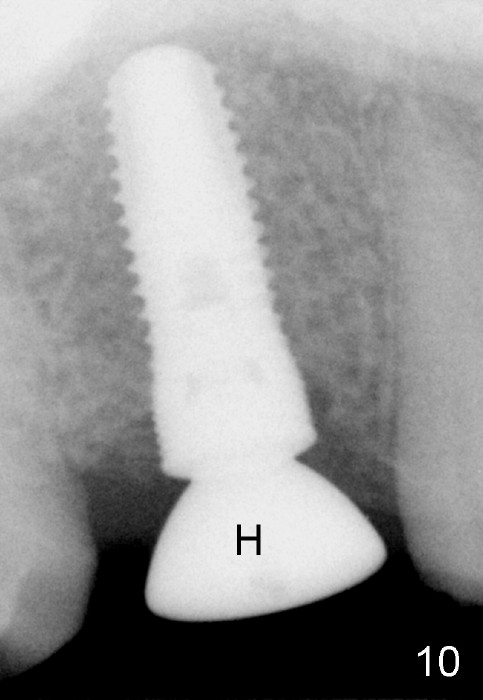
Bone Expansion and Condensation
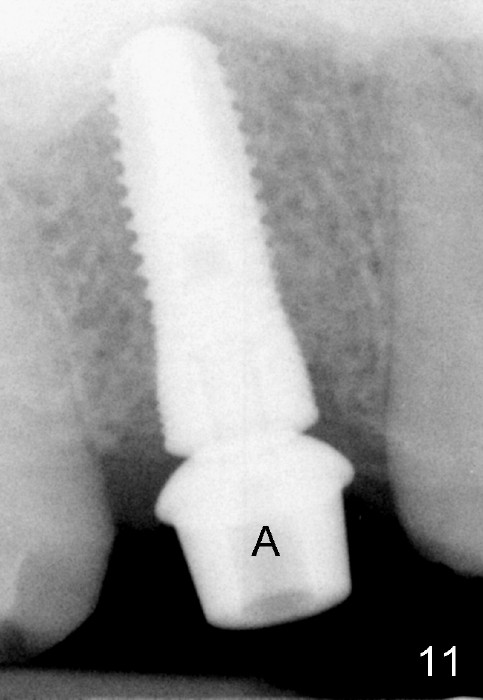
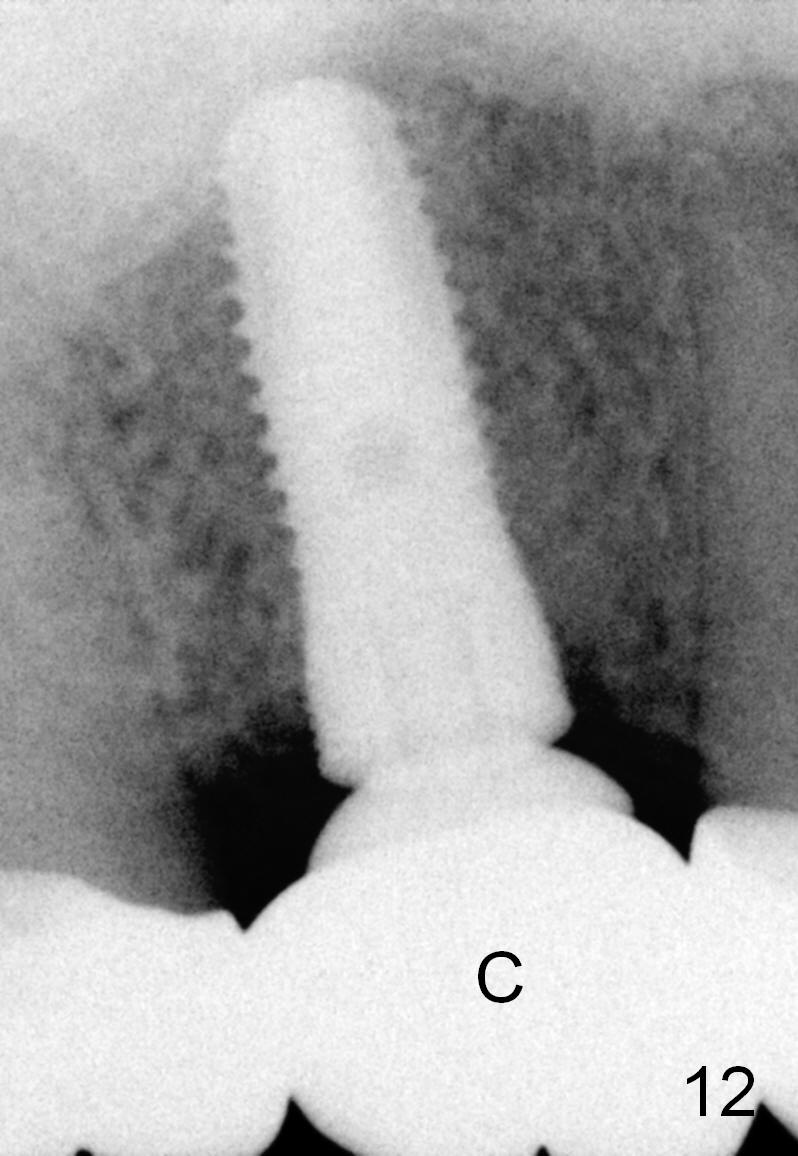
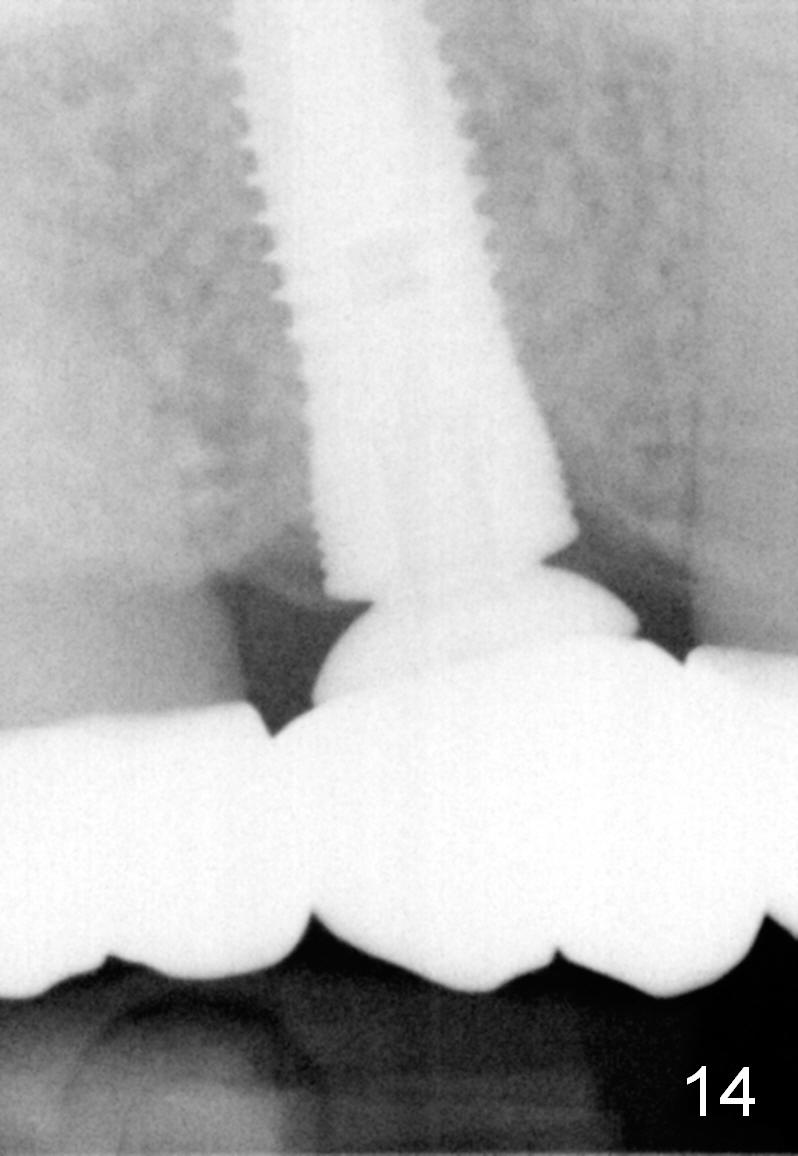
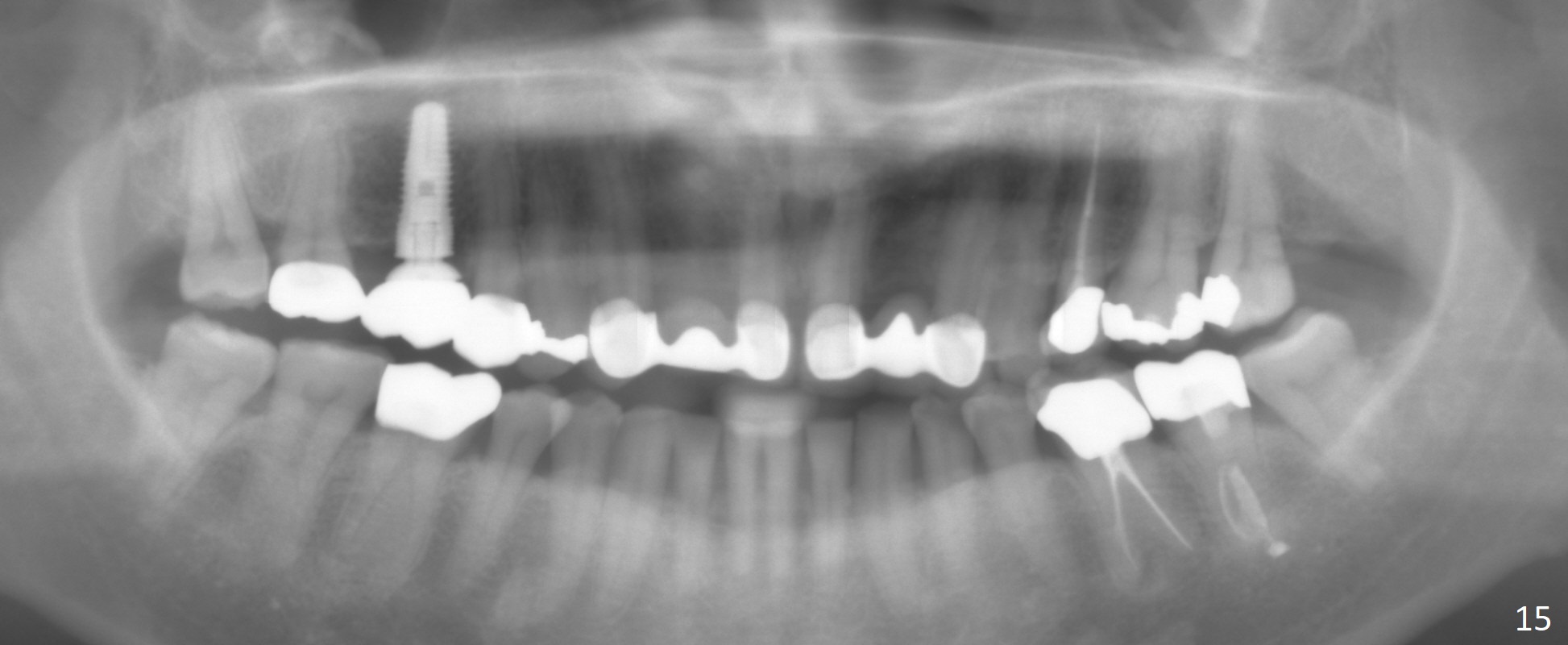
The bone density (Fig.1 white *) at the edentulous area (#3) is lower than that at the dentulous one (black *, 50 year-old man). The buccal plate is also atrophic and concave (Fig.2,3 arrowheads). A series of bone expanders are used to form osteotomy (following 1.6 mm pilot drill) at the depth of 14 mm (Fig.3 E 3.0 mm in diameter). When the last expander (4.3 mm) is removed from the osteotomy, the buccal plate appears to have been moved buccally (Fig.5 arrowheads). A 5.3x14 mm submerged implant (Fig.6 I) is placed with insertion torque >35 Ncm. The buccal plate seems to improve following placement of an 8.2 mm healing abutment and suturing (Fig.7). No bone graft is used. The buccal plate remains normal 12 days postop (Fig.8). It is slightly concave 3 months postop (Fig.9) with minimal bone resorption at the crest (Fig.10 (H: healing abutment),11 (A: cemented abutment). Nine months post cementation (12 months postop), bone resorption at the crest remains minimal (Fig.12) while the buccal plate (Fig.13 *) at #3 remains strong. Bone loss appears not to get worse 22 months post cementation (Fig.14). Soft and hard tissues remain healthy around the implant crown 3 years (Fig.15) and 3.5 years (Fig.16,17) post cementation.
In brief, bone expanders or osteotomes can be used for bone expansion and condensation to improve primary stability of implant placement. No bone graft appears to be needed. The buccal concavity remains minimal 6 years post cementation (Fig.18). In fact he is a bruxer with torus palatinus (Fig.19). The bridge of #9-11 is loose because of subgingival fracture of the abutment of #11 for 2.5 years (Fig.20).
Return to
Instruments
Professionals
Upper Molar Immediate Implant
劈开术
Xin Wei, DDS, PhD, MS 1st edition 08/07/2014, last revision 04/11/2021