

.jpg)



|
|
|
|
|
||
|
|
|
|
|
||
|
|
|
|
|
||
|
|
|||||
Hemorrhage Control in Immediate Implant
Success of immediate implant, especially anterior, depends upon a few steps of initial osteotomy: finding an appropriate position and controlling angulation. Although the initial osteotomy can be finished blindly, clear surgical field without hemorrhage is the most helpful factor. We want to test whether packing 2% Lidocaine with 1:50,000 Epinephrine saturated gauze in the extraction socket is able to reduce hemorrhage.
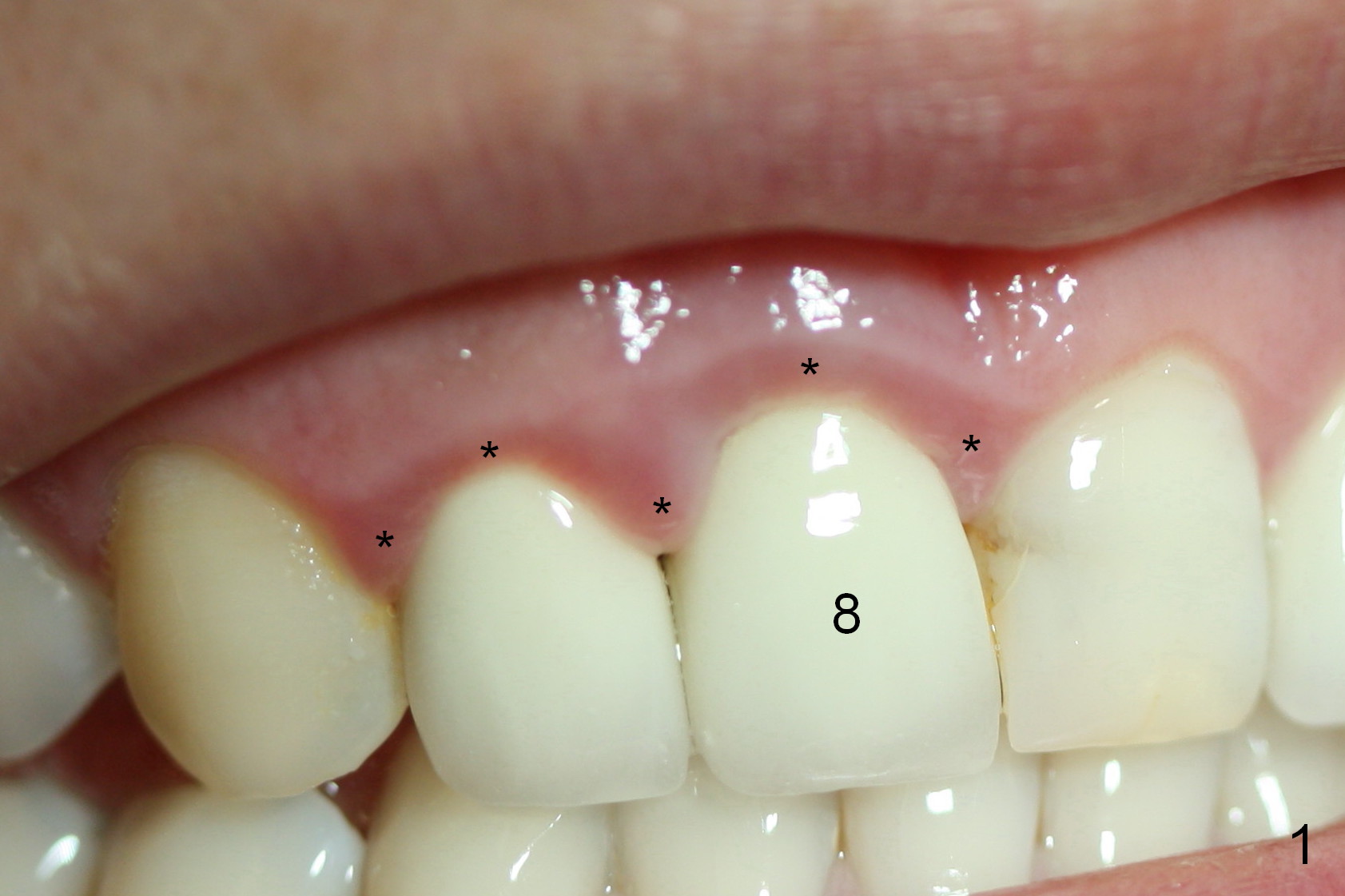
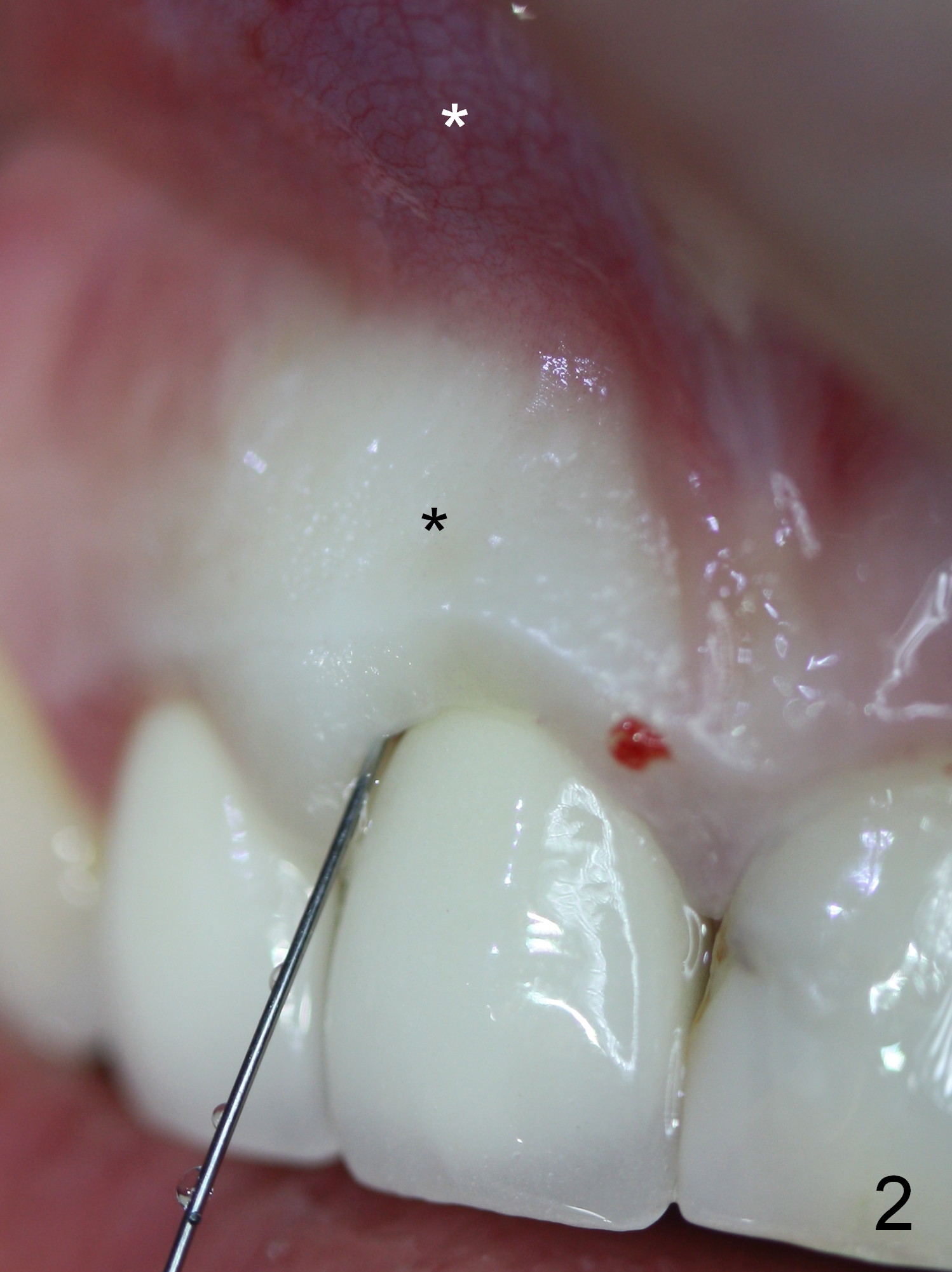
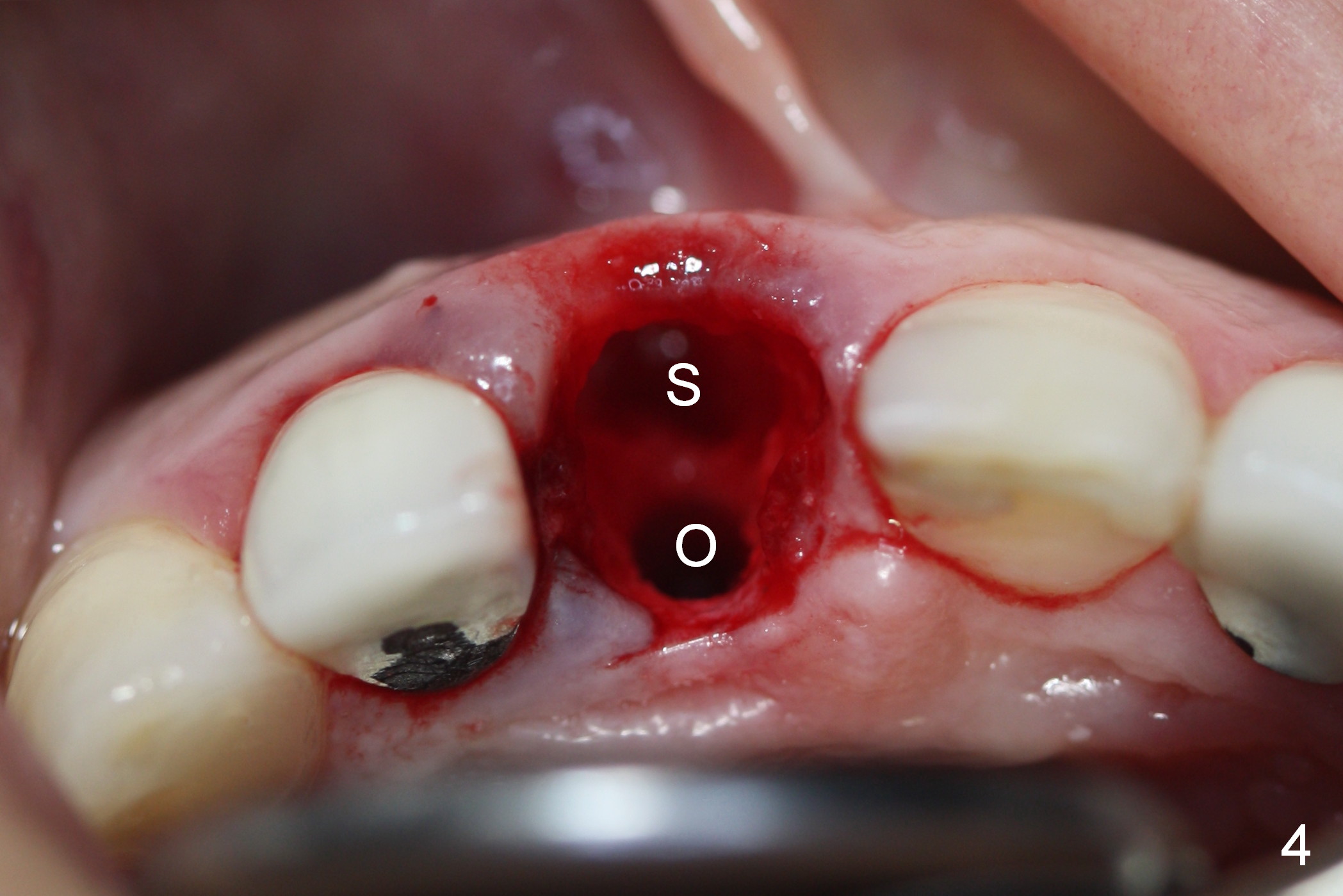
The gingival margin of the teeth #7,8 remains erythematous in spite of diligent brushing after recementation (Fig.1 *). In addition to infiltration in the buccal vestibule (Fig.2 white *), intra-ligamental injection is administered in the affected tooth with the anesthetic mentioned above (black *, for added hemostatic effect). It appears that these two measures have some measurable effect; after initial osteotomy (Fig.3: 2 mm pilot drill; Fig.4 after 3 mm reamer), hemorrhage is minimal (Fig.4 O: osteotomy; S: socket). A 4.5x14 mm implant is placed with insertion torque 55 Ncm (Fig.5). For immediate provisional, the implant is later placed 1-2 mm more apically (Fig.6) and a 4.8x5.5(2) mm abutment (A) is installed.
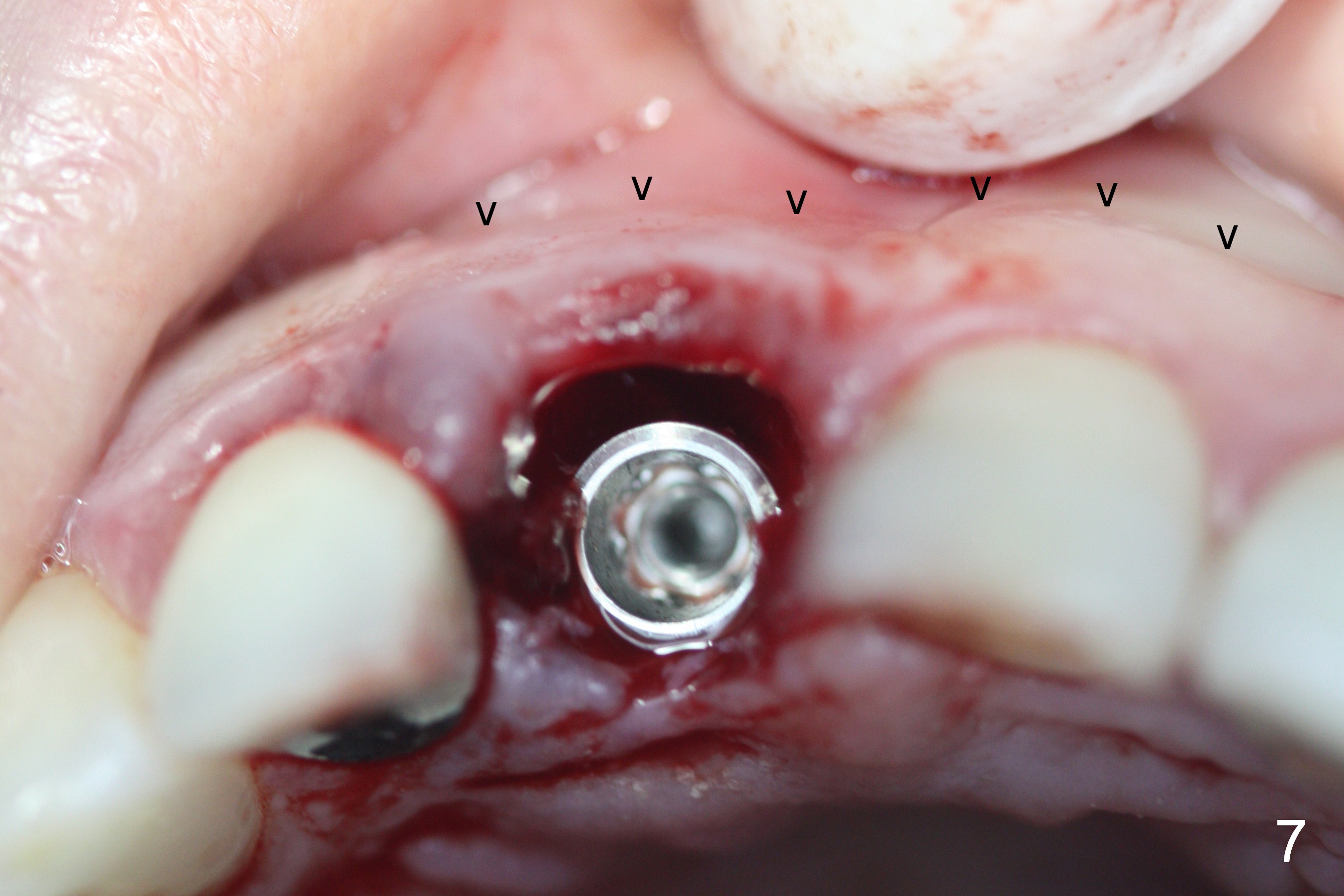
The buccal gingiva appears to collapse when the implant is placed (Fig.7 arrowheads). By the time the abutment and bone graft (Fig.6,8 *) are placed, the buccal gingiva have returned to normal position (Fig.8).
Briefly, 2% Lidocaine with 1:50,000 Epinephrine has hemostatic effect for immediate implant.
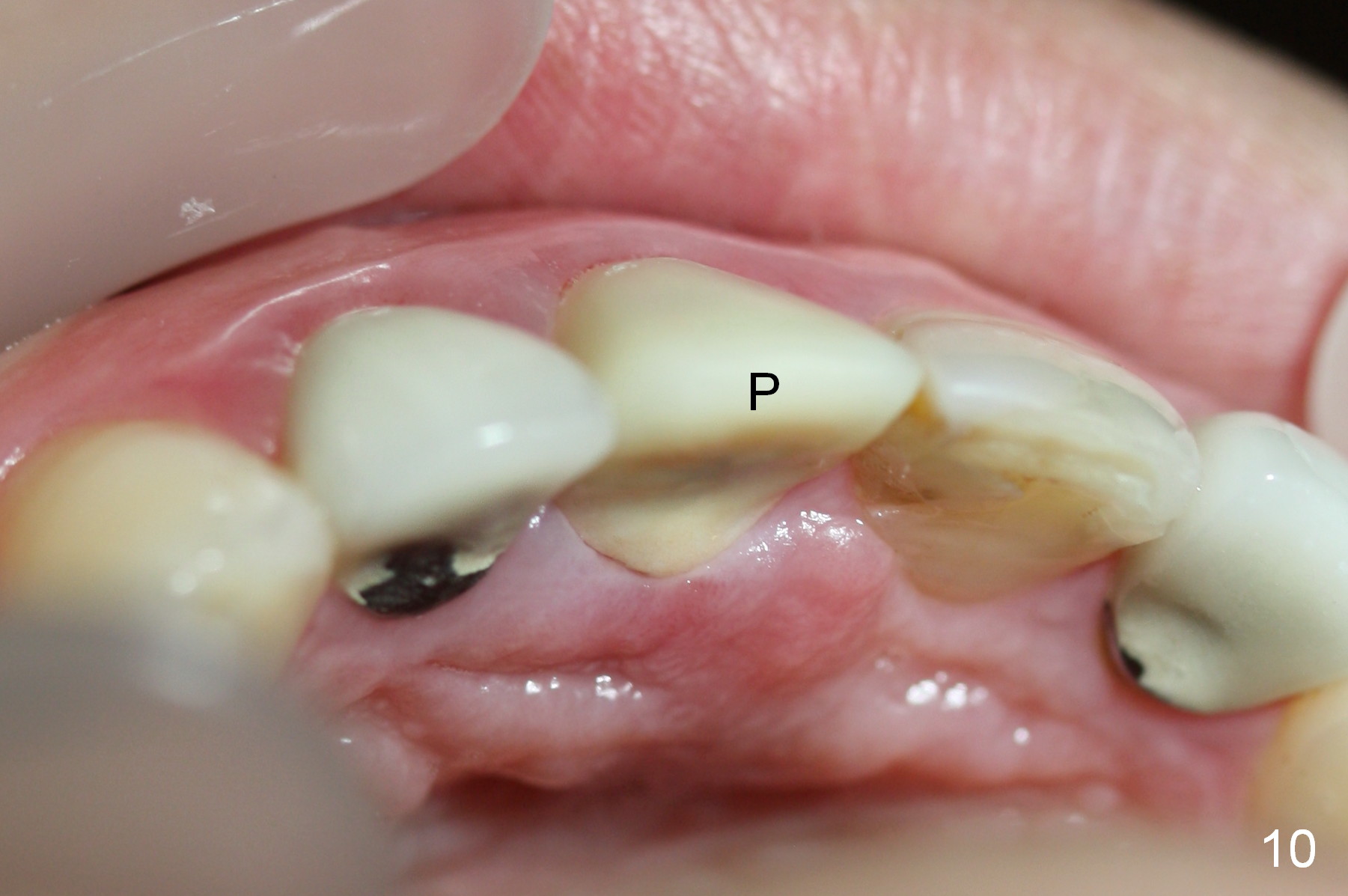
The patient complains of the bulging of the root area at the site of #8 7 days postop (Fig.9), although asymptomatic. The gingiva palatal to the provisional (Fig.10: P) looks less erythematous.
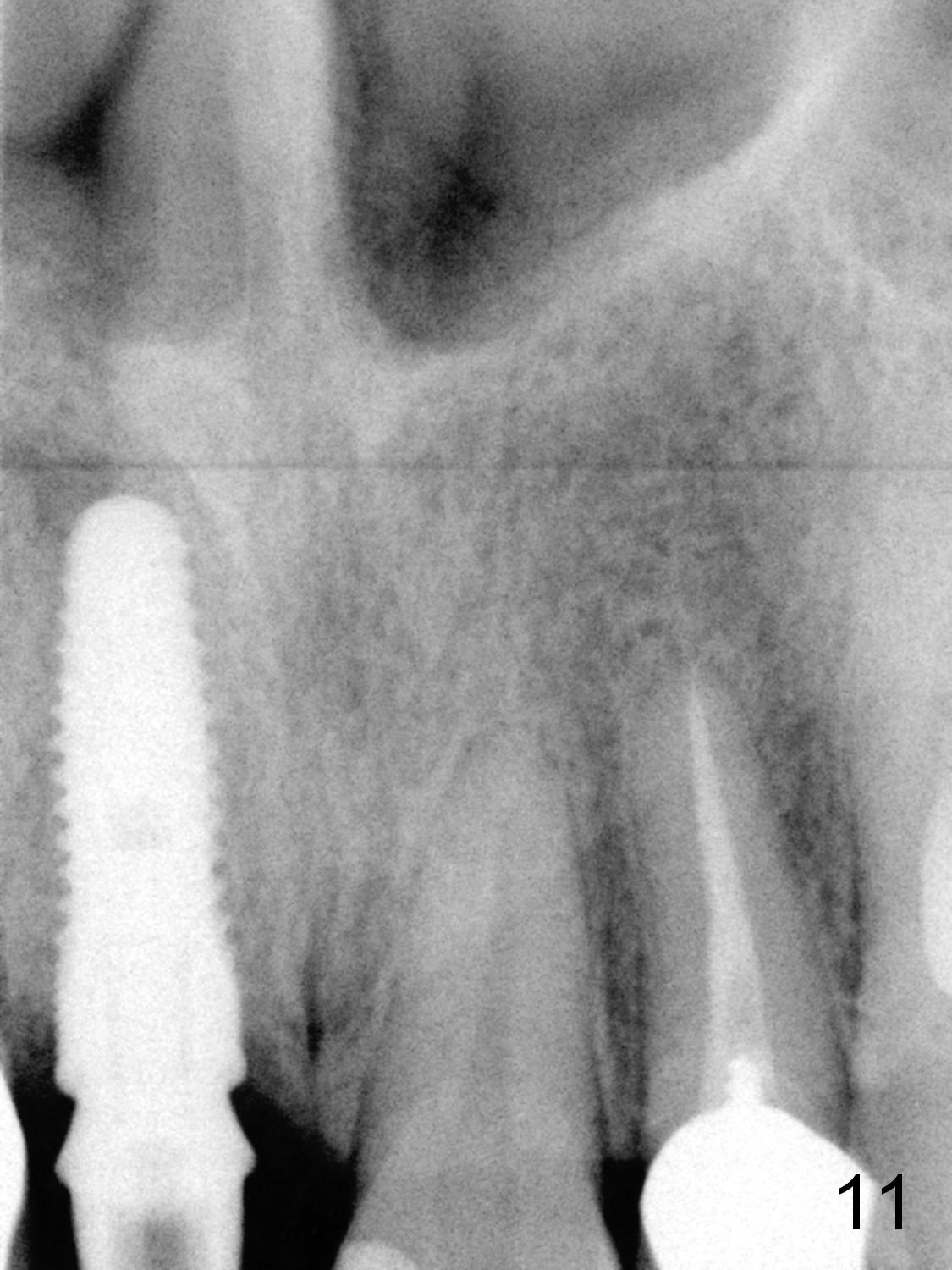
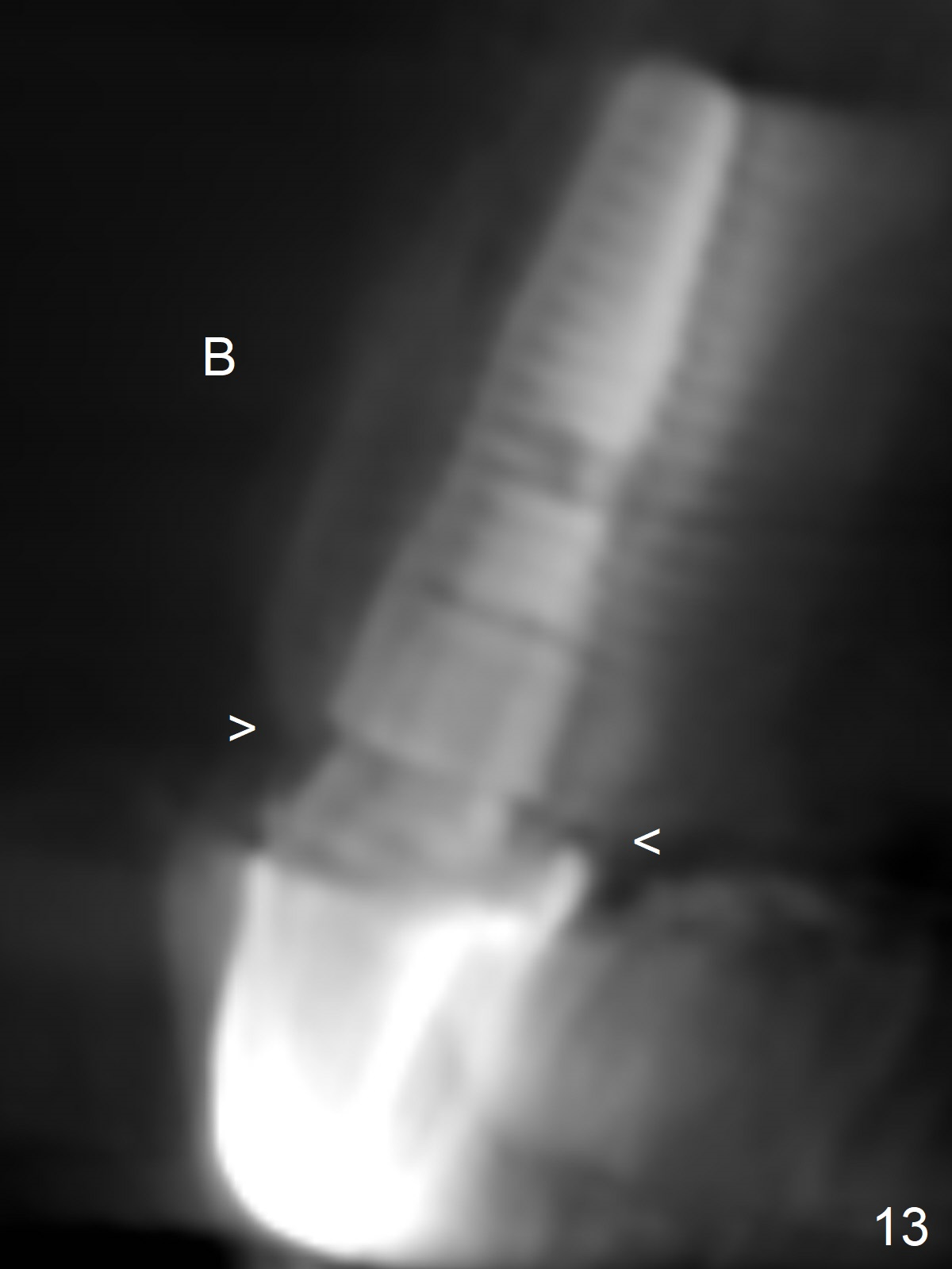
The provisional dislodges 2.5 months postop; bone appears to heal normally around the implant (Fig.11). The abutment is torqued at 35 Ncm, and reprep for impression (Fig.12). CBCT taken 20 months post cementation shows that the implant plateau is apical to the buccal (B) and palatal crests (Fig.13 arrowheads).
Return to Upper Incisor Immediate Implant,
Technicians, #10,30,31,
4
Trajectory/Guided Surgery
Xin Wei, DDS, PhD, MS 1st edition 07/21/2015, last revision 11/01/2020