


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Blind Osteotome Osteotomy for Upper Molar Immediate Implant
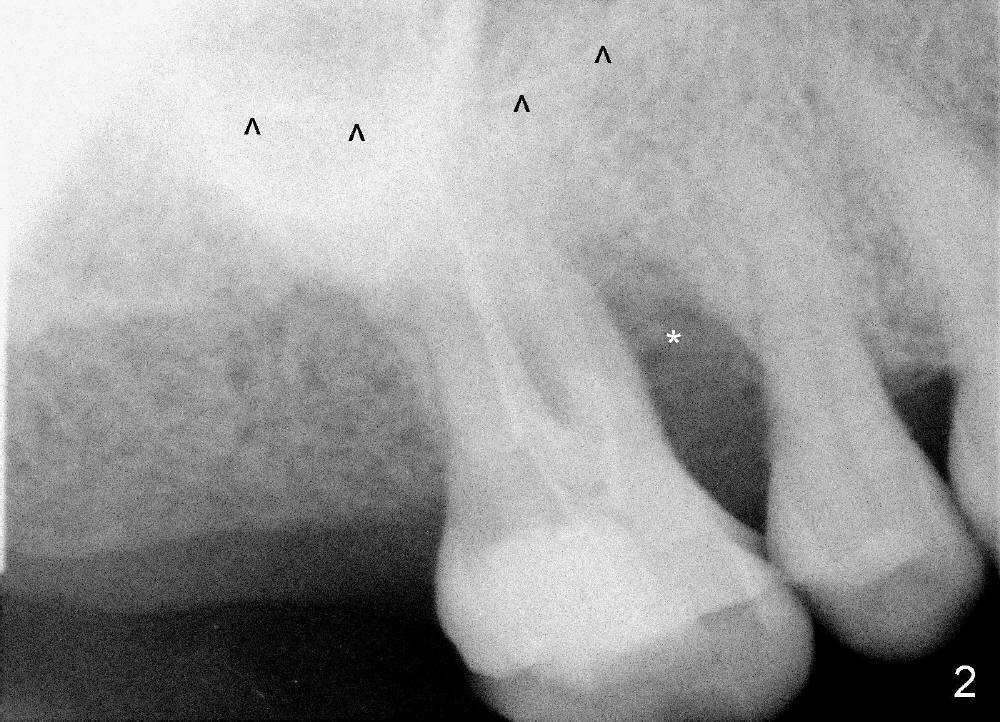
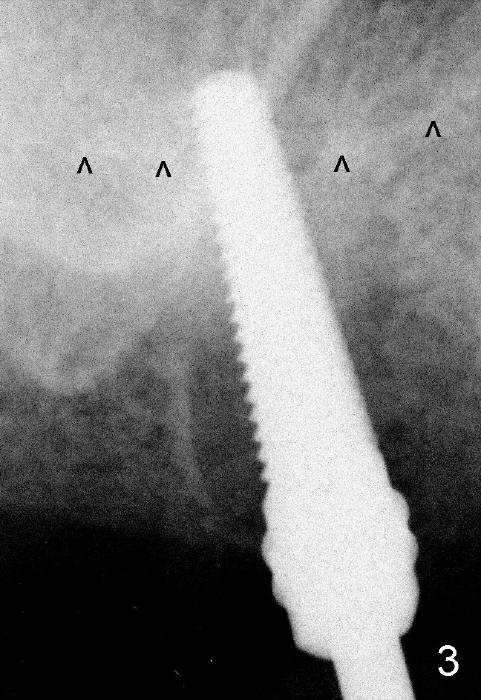
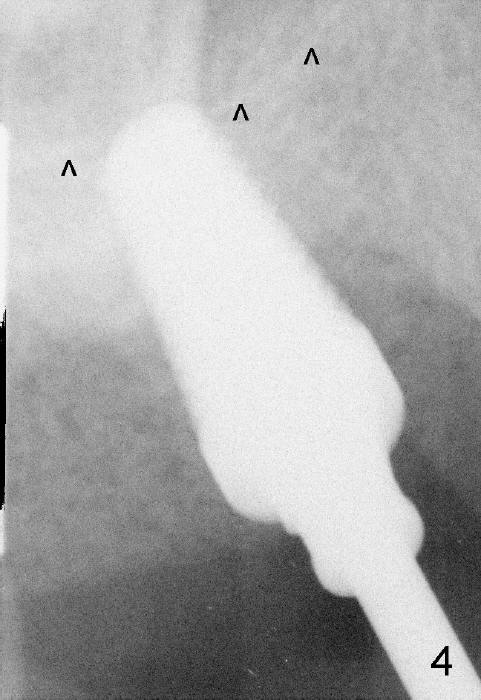
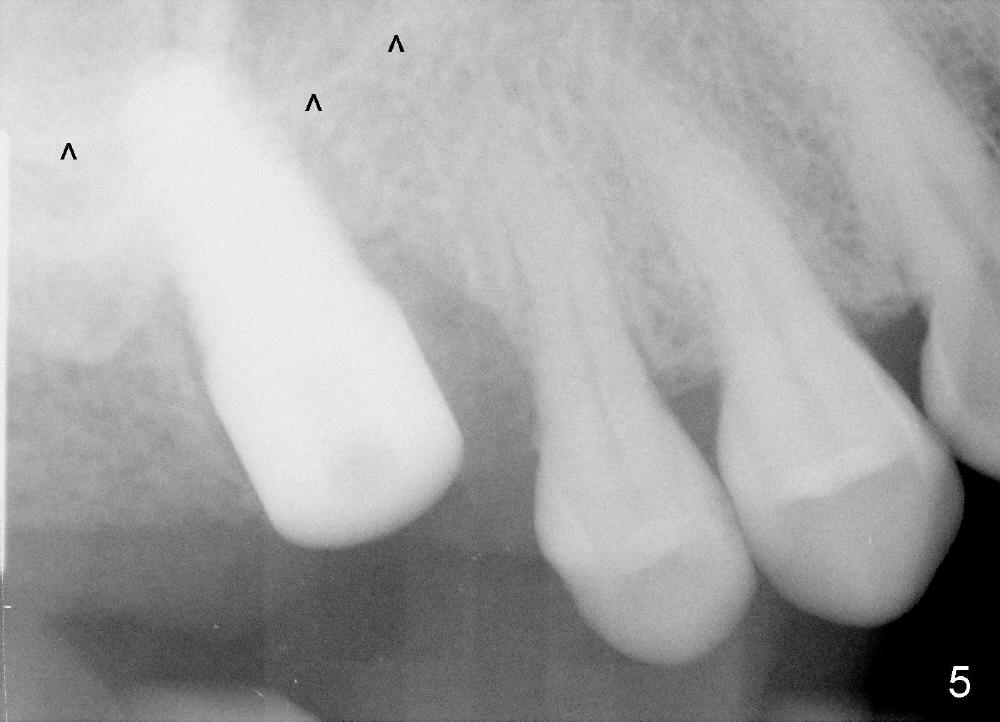
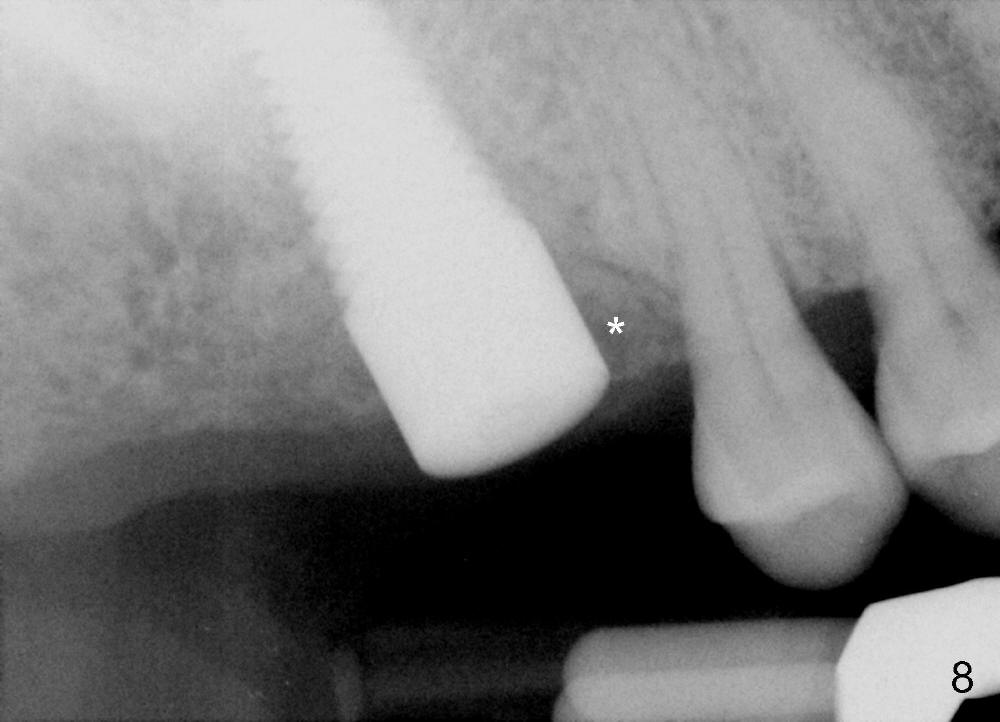
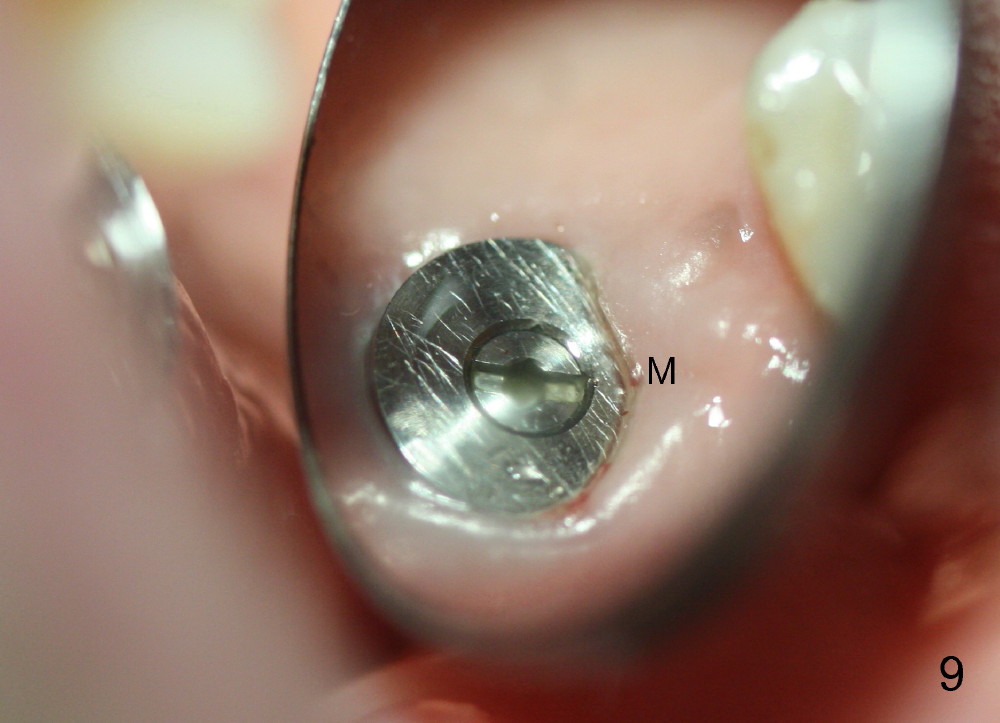
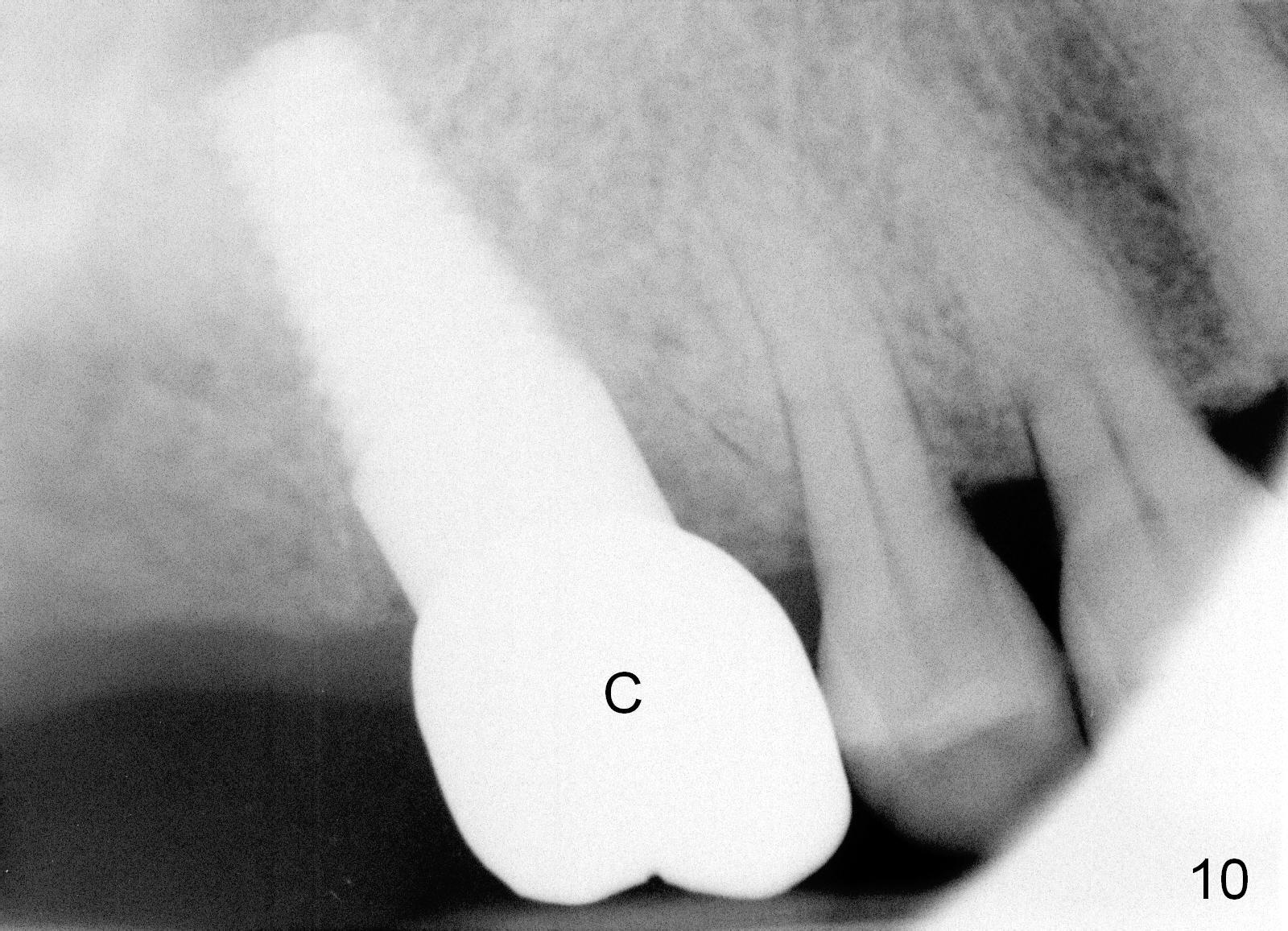
The upper right 1st molar fractures, the lingual portion mobile (Fig.1). There are deep pockets mesiolingually and distolingually. Fig.2 is preop PA, showing mesial bone resorption (*). The 84-year-old lady agrees extraction and immediate implant. Extraction is difficult due to not only root fracture but also hemorrhage. Following debridement of granulation tissue, the 3 sockets are packed with gauze for hemostasis. Even so, there is oozing from the bone. The septum can not be seen clearly. Its position is determined by an explorer. Osteotomes have to be used for osteotomy in the septum, followed by taps. The first intraop PA shows that 5x20 mm tap penetrates the sinus floor (Fig.3 ^). The osteotomy is further enlarged until 7x17 mm tap with stability (Fig.4). So far there has been no sign of sinus membrane perforation. Mixture of freeze dry mineralized bone and Osteogen is placed in the socket and pushed to the buccal and lingual walls as well as into sinus using a 4 mm flat end osteotome. A 7x17 mm implant is initially difficult to be inserted possibly due to blockage by bone graft. The osteotomy have to be recreated by a series of osteotomes and taps before placement of the 7x17 mm implant. It appears that the apical threads have been engaged into the sinus floor for primary stability (Fig.5). The insertion torque is 40 Ncm. According to our experience (1,2), this is not enough; finally the torque is increased to 60 Ncm by turning the implant more apically. The large implant obliterates the socket mesiodistally; the buccal and lingual gaps are filled with bone graft, followed by a collagen membrane (Fig.6 *) and suture. In order to protect the membrane, a short abutment is placed (A) and perio dressing (Fig.7*) is placed without occlusal interference. The abutment is removed 1 month postop, as the perio dressing has been dislodged. The patient returns for restoration 8 month postop. Bone regeneration occurs apparently in the coronal aspect of the implant (Fig.8), especially mesially (*, as compared to Fig.5). The gingiva-level implant is slightly subgingival mesially (Fig.9 M), probably due to high placement (compare to Fig.6). There is no bone resorption 6 months post crown (Fig.10 C) cementation.
Immediate Implants,
Upper Molar Immediate Implants
Xin Wei, DDS, PhD, MS 1st edition 04/24/2014, last revision 12/21/2019