












|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
||||
Setback is a Precursor to Success
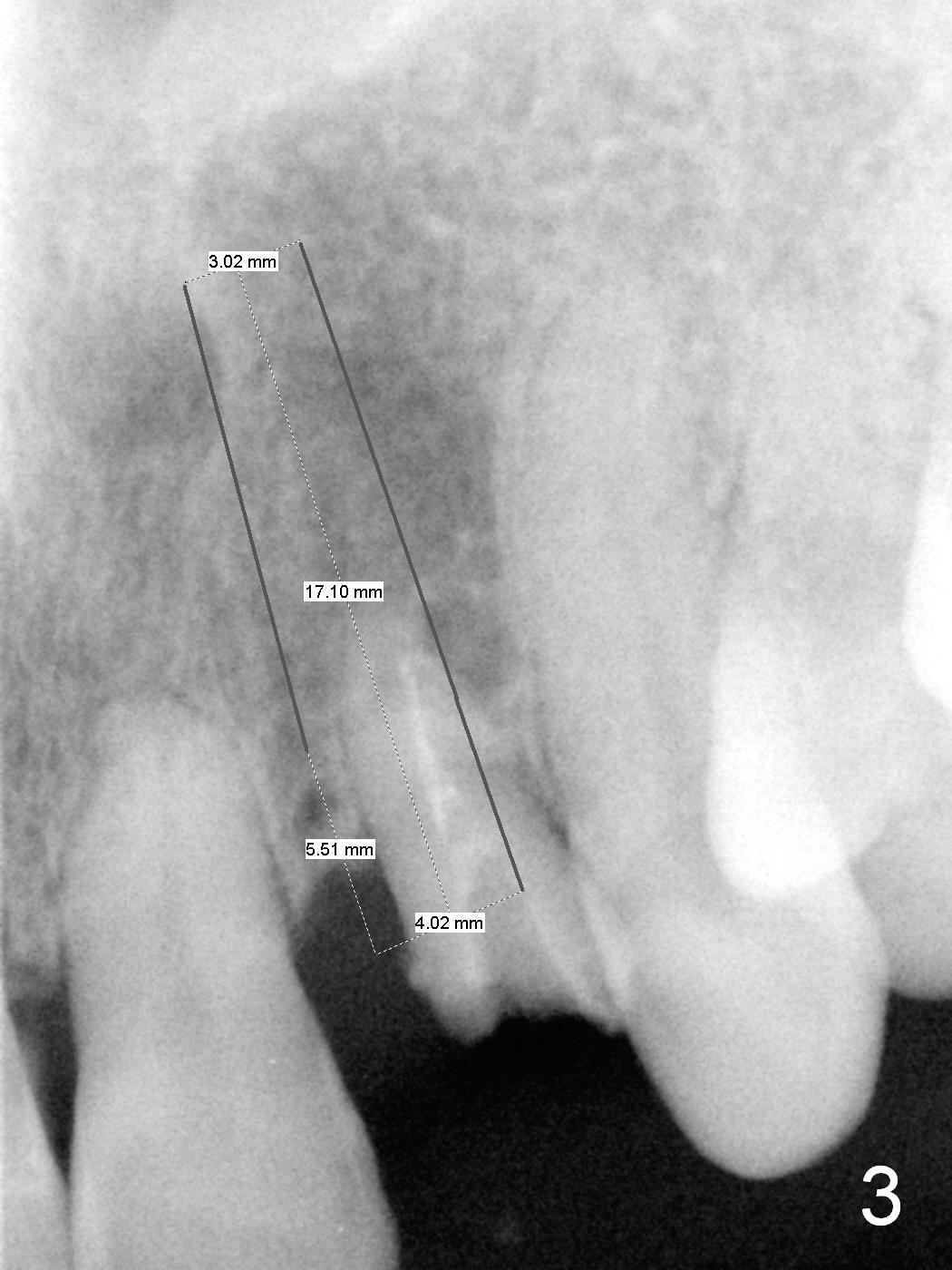
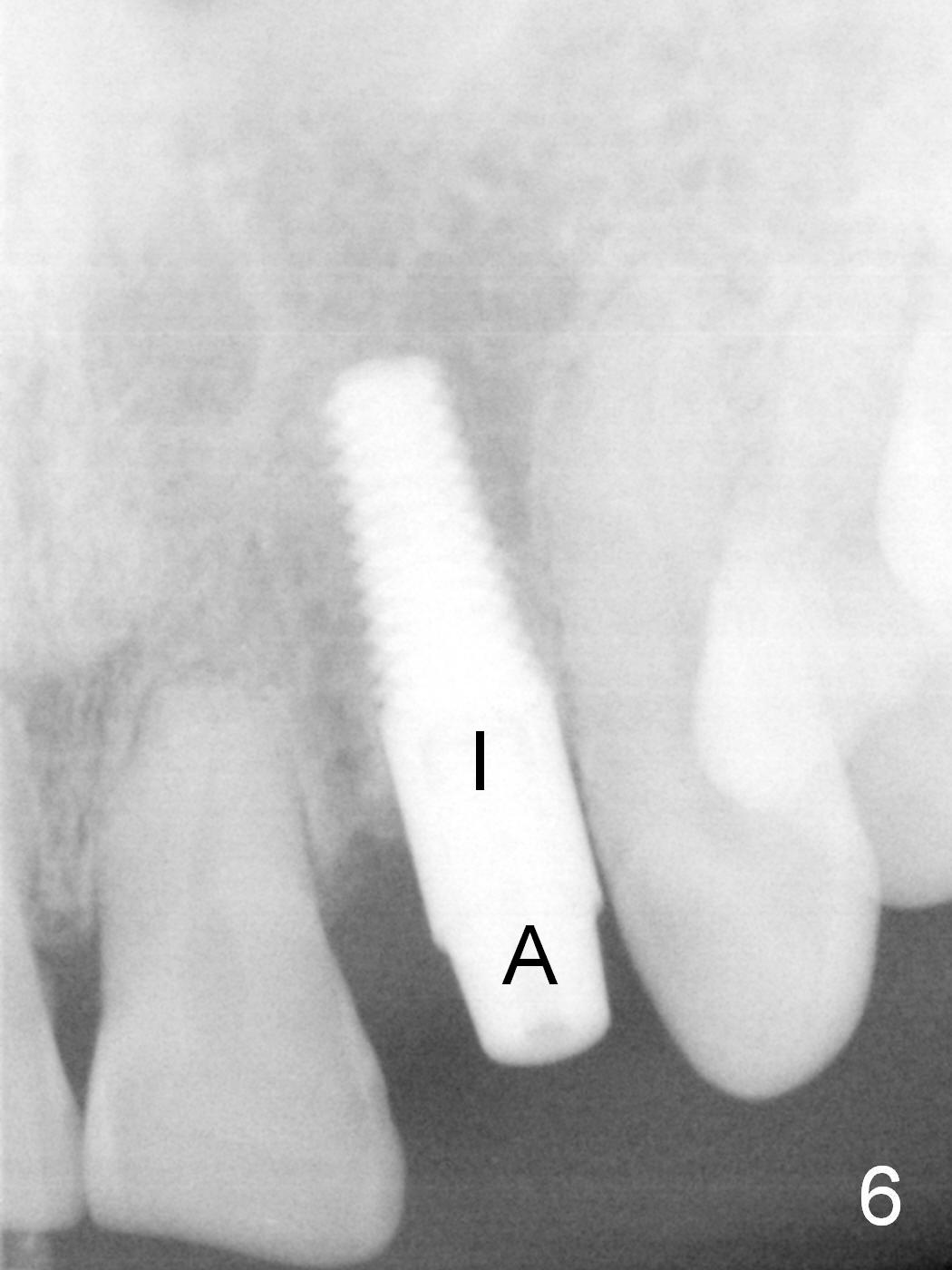
A 57-year-old lady returns to clinic for #10 crown emergency re-cementation. The tooth is deemed non-salvageable. She does not want to reschedule for immediate implant. After re-arranging the schedule, we start the case. The challenge is that the residual root is deviated distally (Fig.1,2 arrow). The implant is intended to be placed in the right position (Fig.3). Clinically a 2 mm pilot drill is placed as mesially as possible, but X-ray does not confirm it (Fig.4). The trajectory is changed as shown in Fig.5. The change is minimal, because the bone is soft. A 4x14 mm implant is placed with insertion torque of 35 Ncm (Fig.6 I). It is deviated distally. The immediate provisional is difficult to be fabricated because of the deviation of the implant. The provisional is dislodged by the evening. The problem is due to using a short abutment (A: 3 mm).
The deviation of the implant should have been fixed by overcorrecting the position (not just angle) of the initial osteotomy (Fig.7).
The deviation of the implant affects stability of the immediate provisional. The patient returns with the dislodged provisional. After using a longer abutment (5 mm) and adjustment, the provisional is stable 15 days postop (Fig.8 P). By then the gingival inflammation have been resolved, as compared to Fig.1.
The patient returns for final restoration 3.5 months postop (Fig.9-14). The crestal bone continues its modulation and adaptation to the implant 4 months post cementation (Fig.15 (arrow), compare to Fig.6,9).
Return to Upper Incisor Immediate Implant,
Technicians
Xin Wei, DDS, PhD, MS 1st edition 05/30/2015, last revision 01/19/2018