

|
|
|
|
|||
|
|
|
|
|
||
|
|
|
|
|
||
Under Prep for Upper Immediate Implant
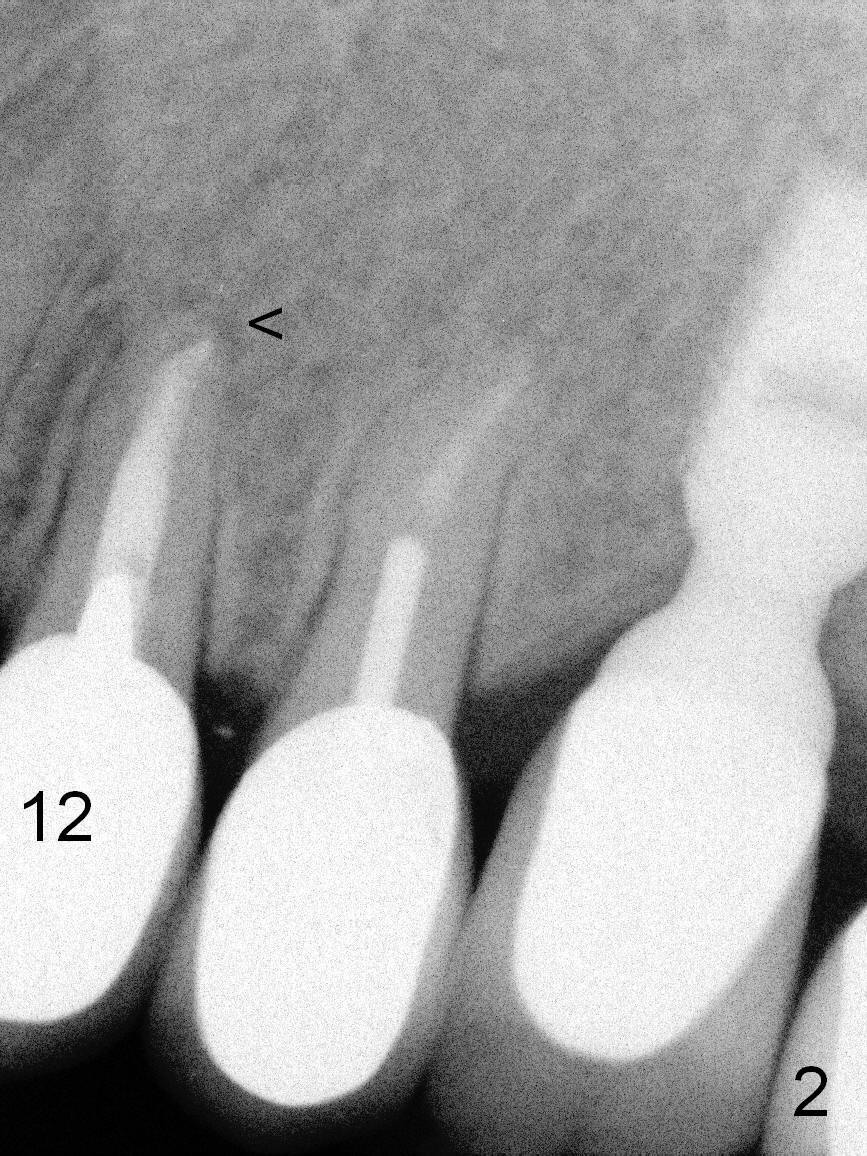
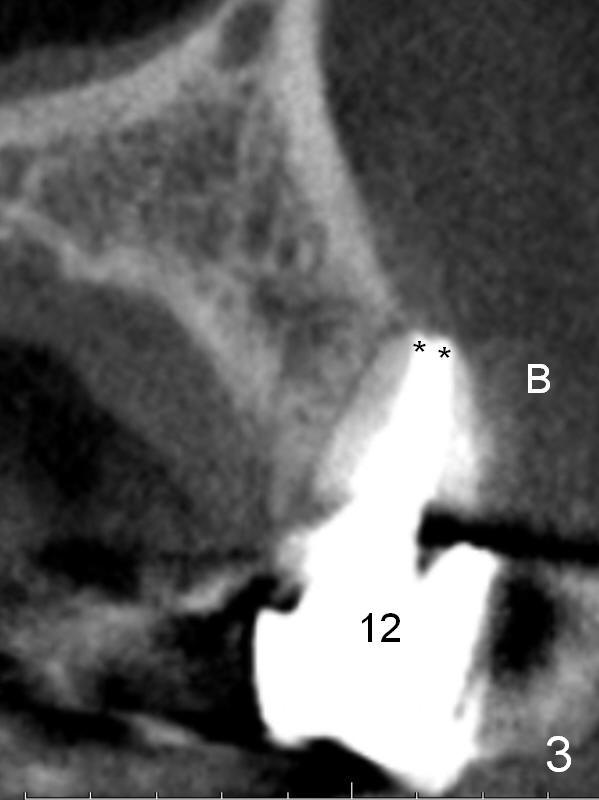
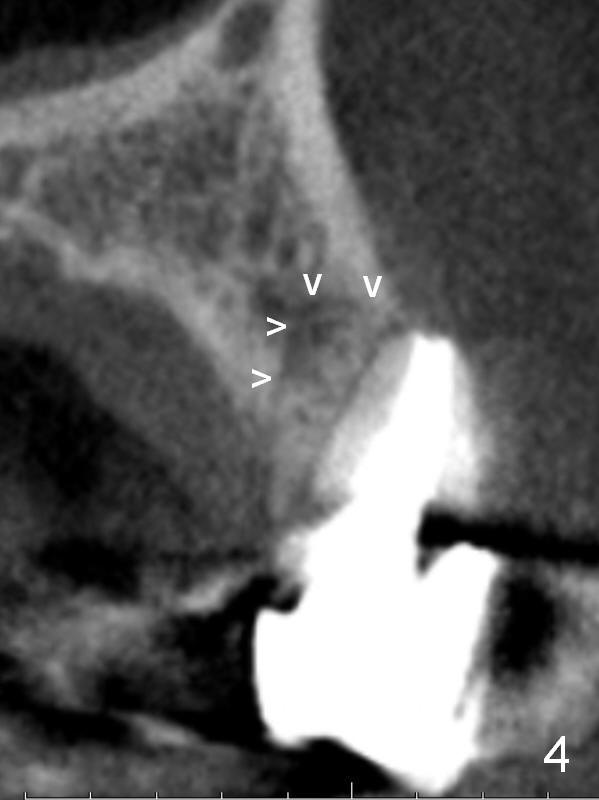
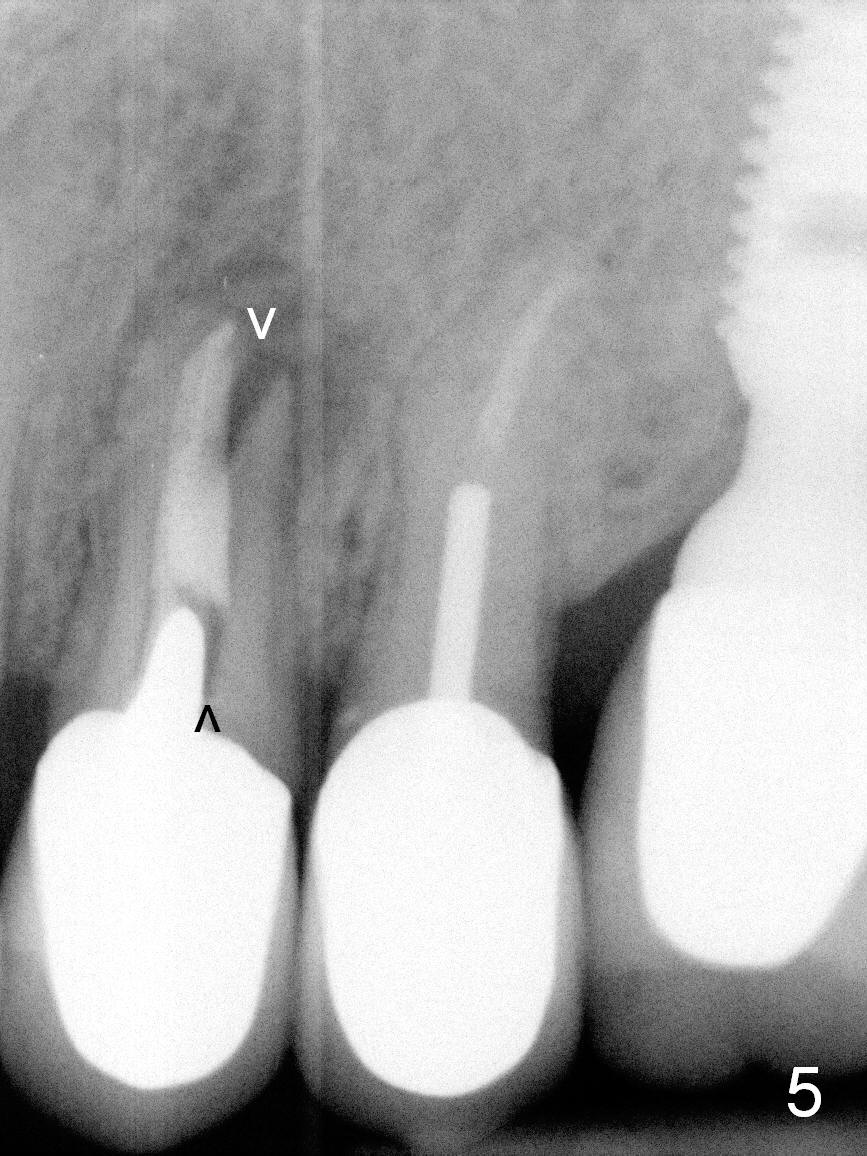
A 57-year-old lady had poor dentition, including periapical radiolucency of the tooth #12, 8 years ago (Fig.1 *, 2007). After comprehensive treatment, the pathology is apparently under control (Fig.2 <, 2011). CBCT shows the pathology not completely resolved (Fig.3,4, coronal section, 2012). Early this year, there was sign of crack tooth at #12 (Fig.5 arrowheads). Last Saturday she returned because of dislodgement of the crown and post. The tooth is found to be non salvageable.
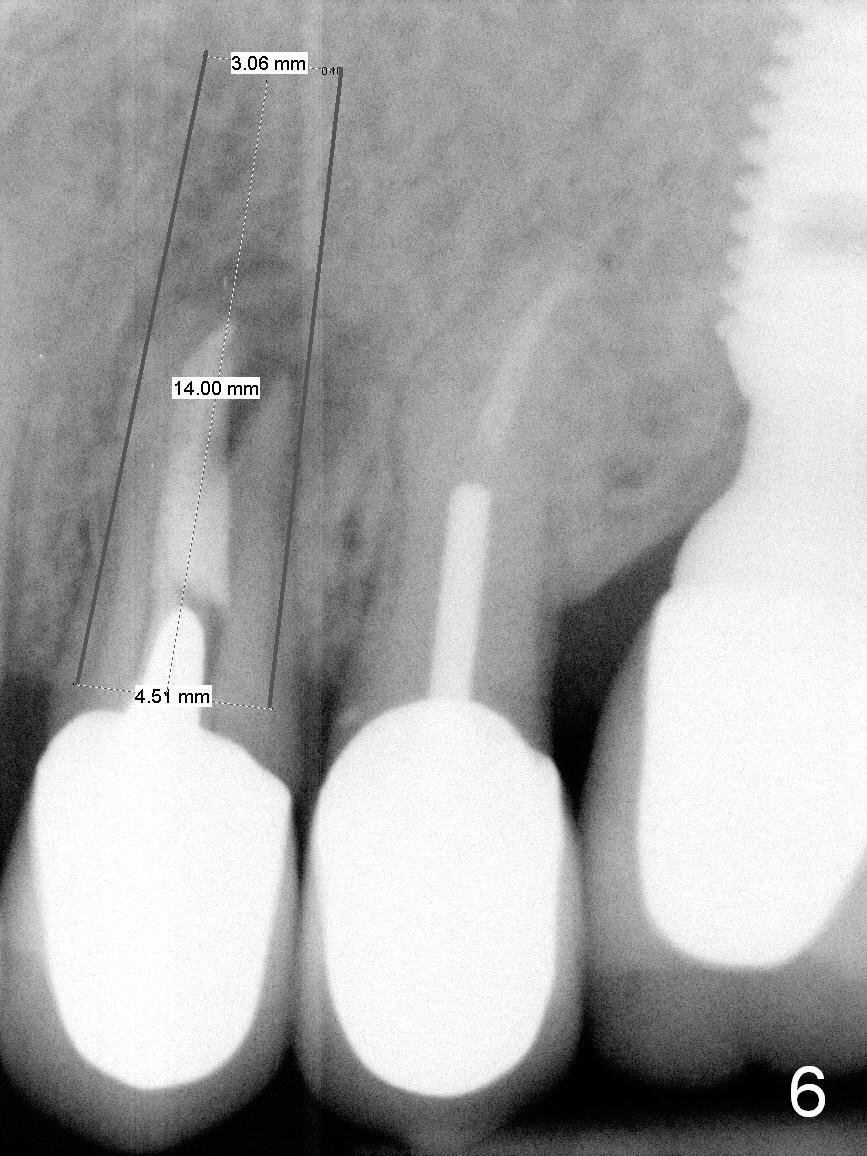
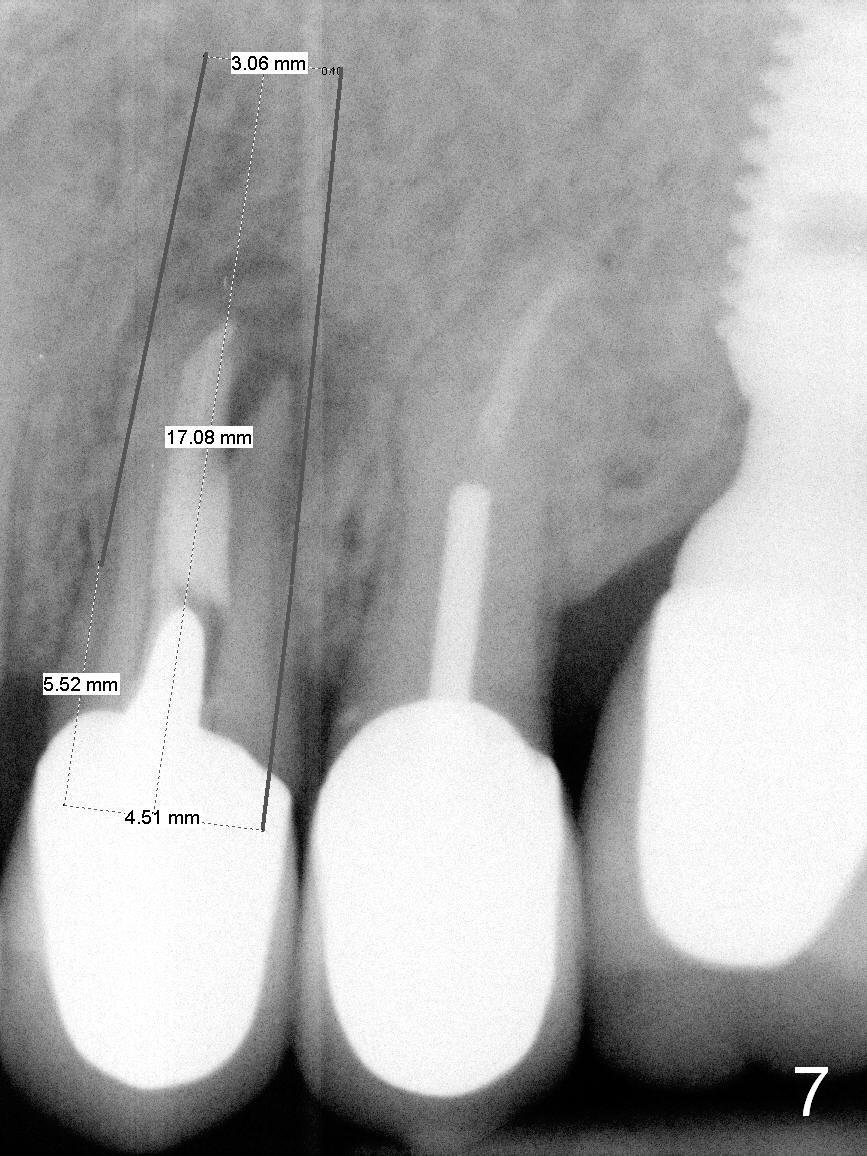
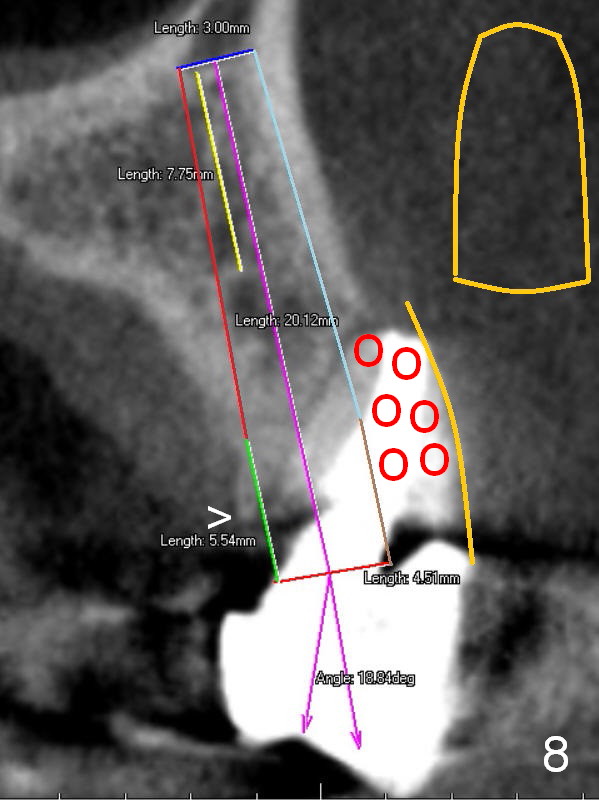
A 4.5x14 mm bone-level or 4.5x17 mm tissue-level implant appears to be appropriate for the site according to the PA (Fig.6,7). CBCT shows that there is enough bone to place a 4.5x20 mm tissue-level implant (Fig.8). This is more appropriate, considering the large radiolucency (Fig.5), the age of the patient (possibly osteoporosis), and the maxilla (bone softer than that of the mandible). The implant will be supported by approximately 8 mm solid bone apically (Fig.8).
In addition, osteotomy will be under prep. The depth of a 2 mm pilot drill, 2.5 mm and 3 mm reamers will be 20 mm, 17 mm and 14 mm, respectively. A 4.5x20 mm tap will be inserted 17 mm before placing the corresponding implant. Intraop PAs are to be taken following the pilot drill, tap and implant.
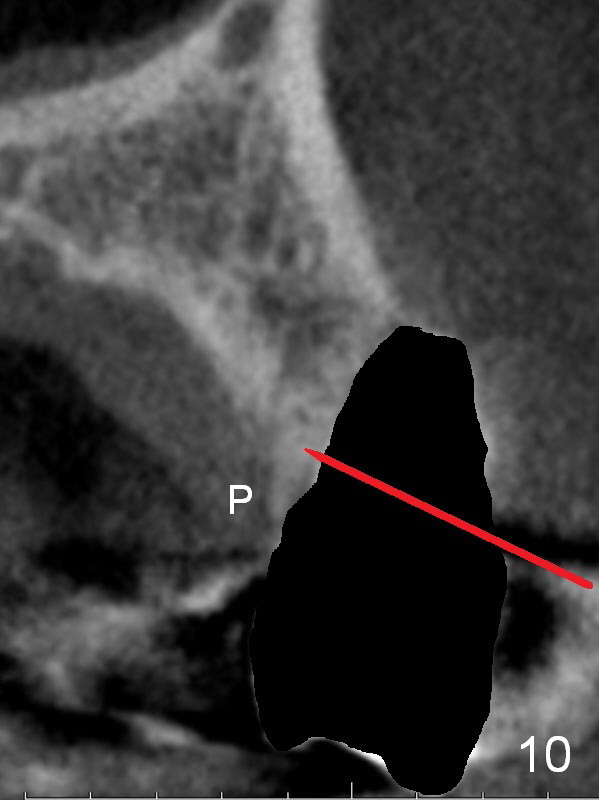
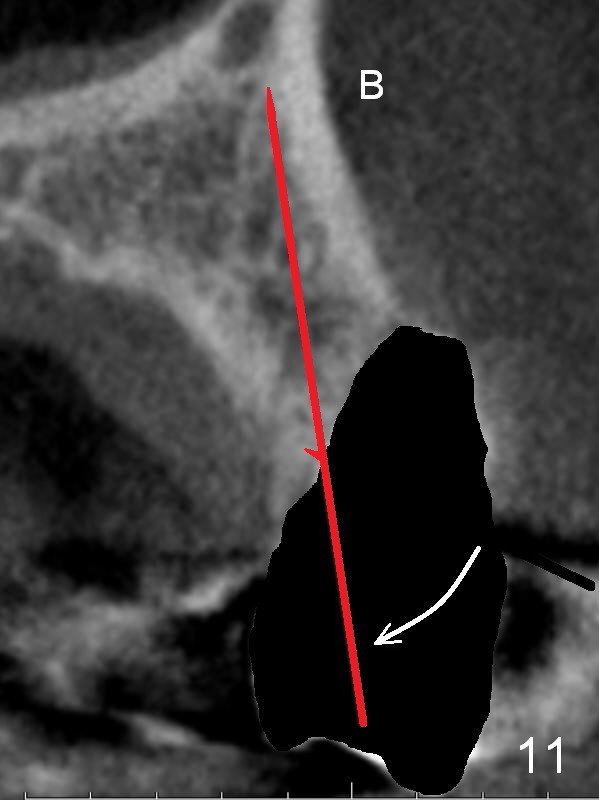
After extraction, the bottom of the socket must be oblique (Fig.9 arrowheads). As usual, osteotomy is initially at the junction of palatal (Fig.10 P) 1/3 and middle 1/3 perpendicular to the plate. Once the drill gets engaged, the trajectory is to be changed (Fig.11 curved arrow) so that the apical end of the osteotomy (red line) is as close to the buccal plate (B) as possible. The purpose is to keep the palatal end of the osteotomy as palatal as possible. In spite of the effort, an angled abutment is expected, as large as 20 degree (Fig.8 purple angle).
After preparation of the implant and abutment and fabrication of an immediate provisional, a cone-shaped Osteo-tape (Fig.8 orange outline) is inserted against the buccal socket wall (most likely completely soft tissue), followed by bone graft (red circles, to the level of the palatal crest (>)).
Return to Upper Bicuspid Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 07/09/2015, last revision 01/19/2018