
|
|
|
|
|
|
|
|
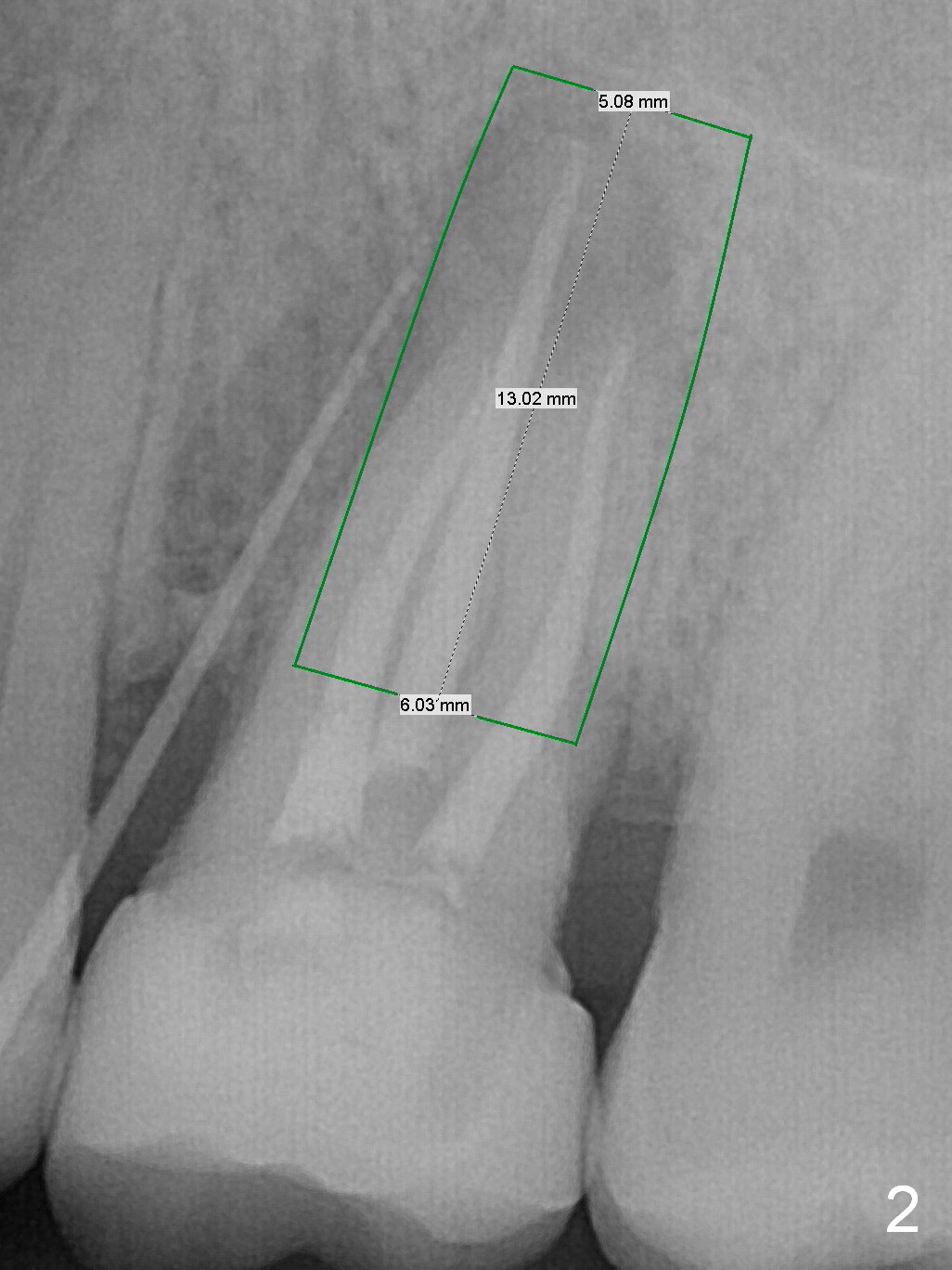
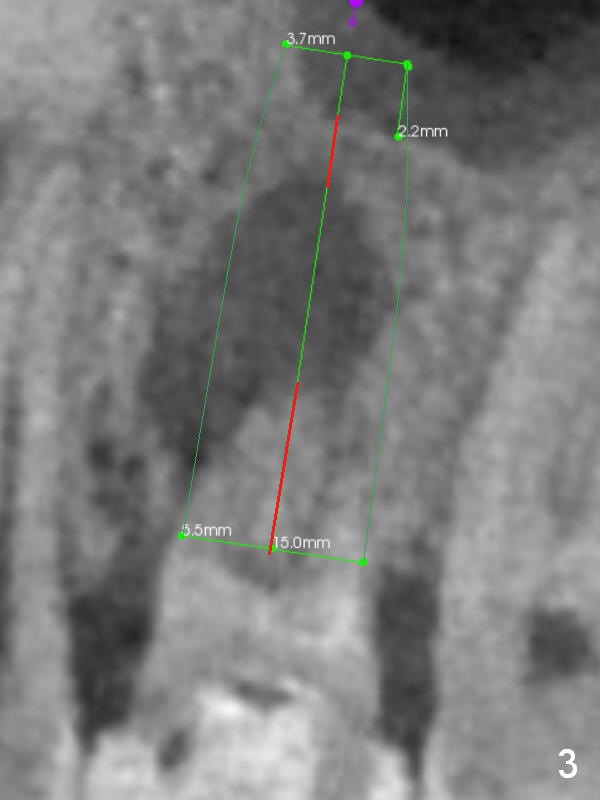
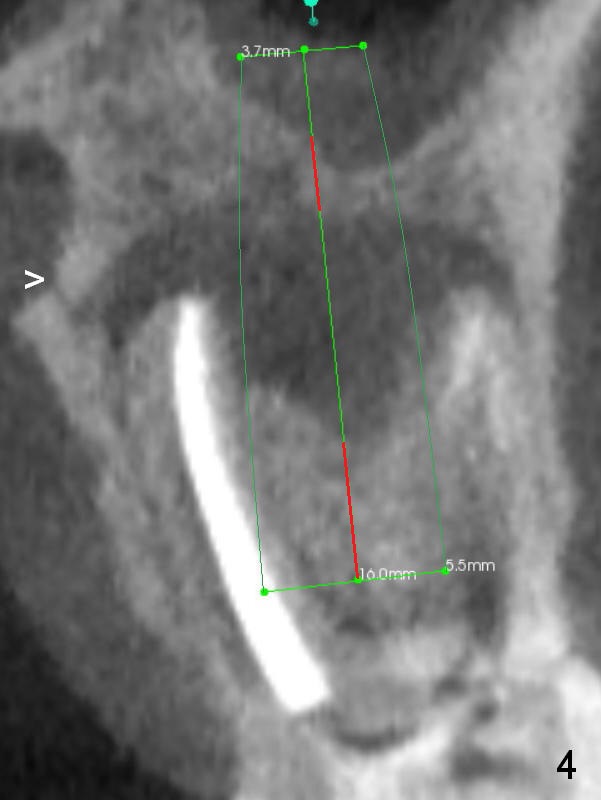
Long Implant Bypasses Defects with 2-Point Fixation
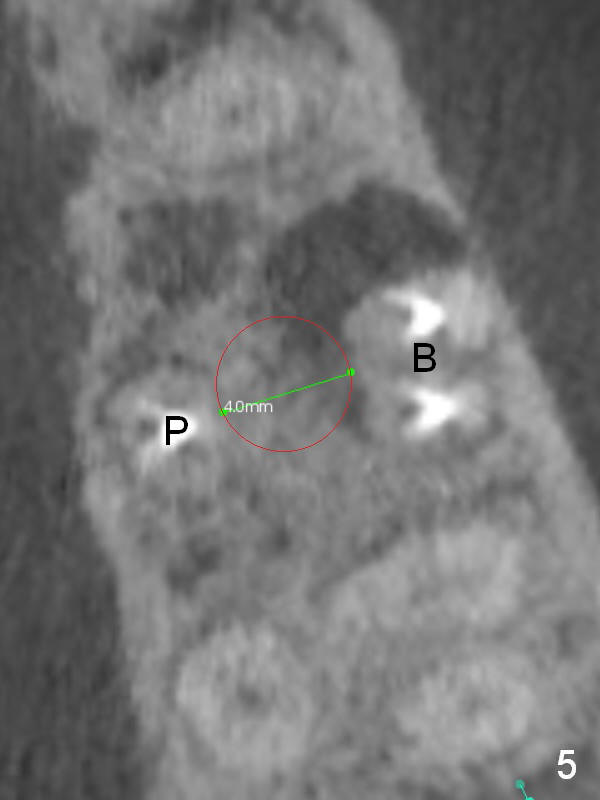
A 34-year-old man has persistent large periradicular radiolucency (Fig.1) after root canal therapy with a fistula (Fig.2). It appears that immediately after extraction (no Antibiotic) a long implant (15 or 16 mm, green outline) should be placed to bypass the bony defect with 2-point fixation (septum and sinus floor; Fig.3 (CBCT sagittal section), 4 (coronal section) red line). A shorter implant, which is placed at the septum (4-5 mm tall), is not expected to be stable. The diameter of the implant is to be determined after sequential osteotomy. The minimal will be 4 mm (Fig.5 axial section) as long as the implant or osteotomy does not perforate the palatal (P) or buccal (B) socket substantially. The bone density at the septum and the sinus floor is 1100 and 200-400 units, respectively. Drills and osteotomes (Tatum or Magic Expanders) will be used for osteotomy in these 2 segments, respectively.
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), IBS
Xin Wei, DDS, PhD, MS 1st edition 02/11/2017, last revision 02/17/2017