


|
|
|
|
|
|
|
|
|
|
|
|
Septum Removal for Apical Lesion Removal
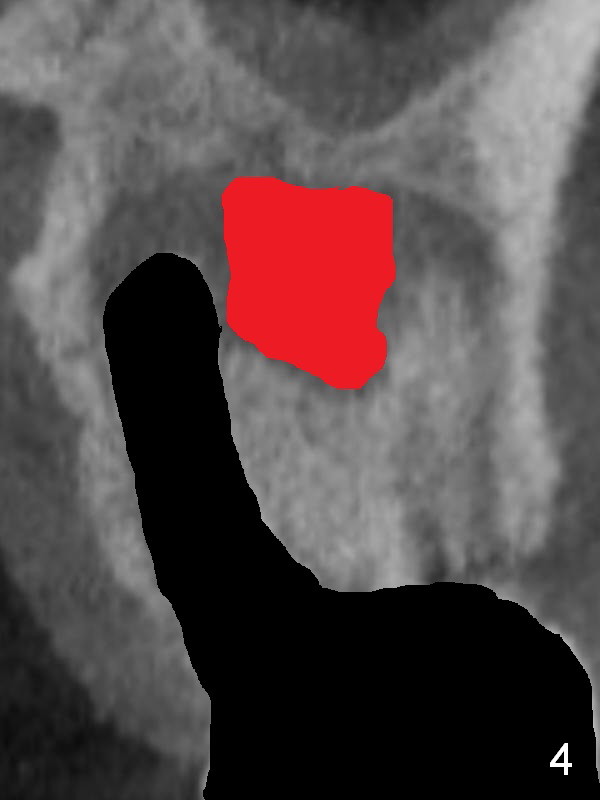
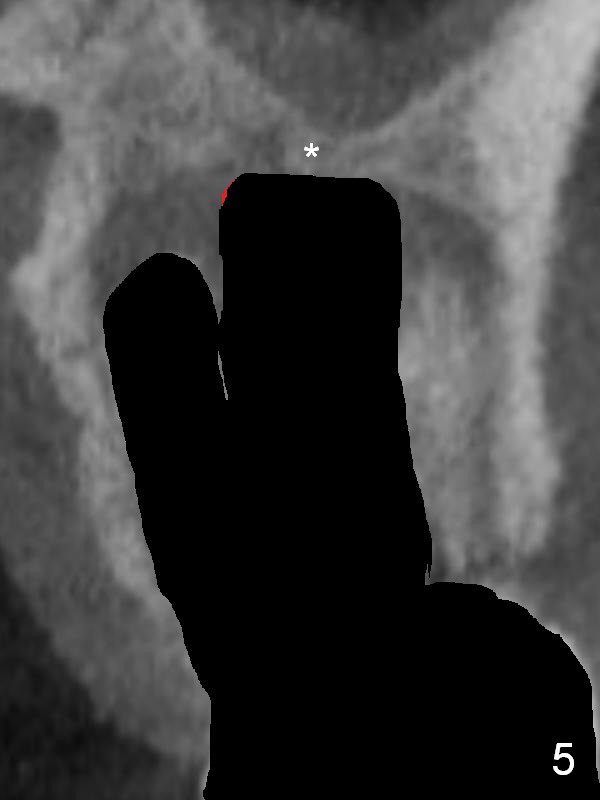
There is purulent discharge from the mesiobuccal fistula (Fig.1 <) during the tooth #14 extraction. Fig.2 is a coronal section of CBCT of the affected tooth showing a large apical lesion (*). When the tooth is removed (Fig.3), limited amount of granulation tissue is removed apical to the palatal root (P in Fig.2). The granulation tissue (Fig.4 red area) above the septum (Fig.3 S) is thoroughly extirpated when the septum is removed (Fig.5 black area).
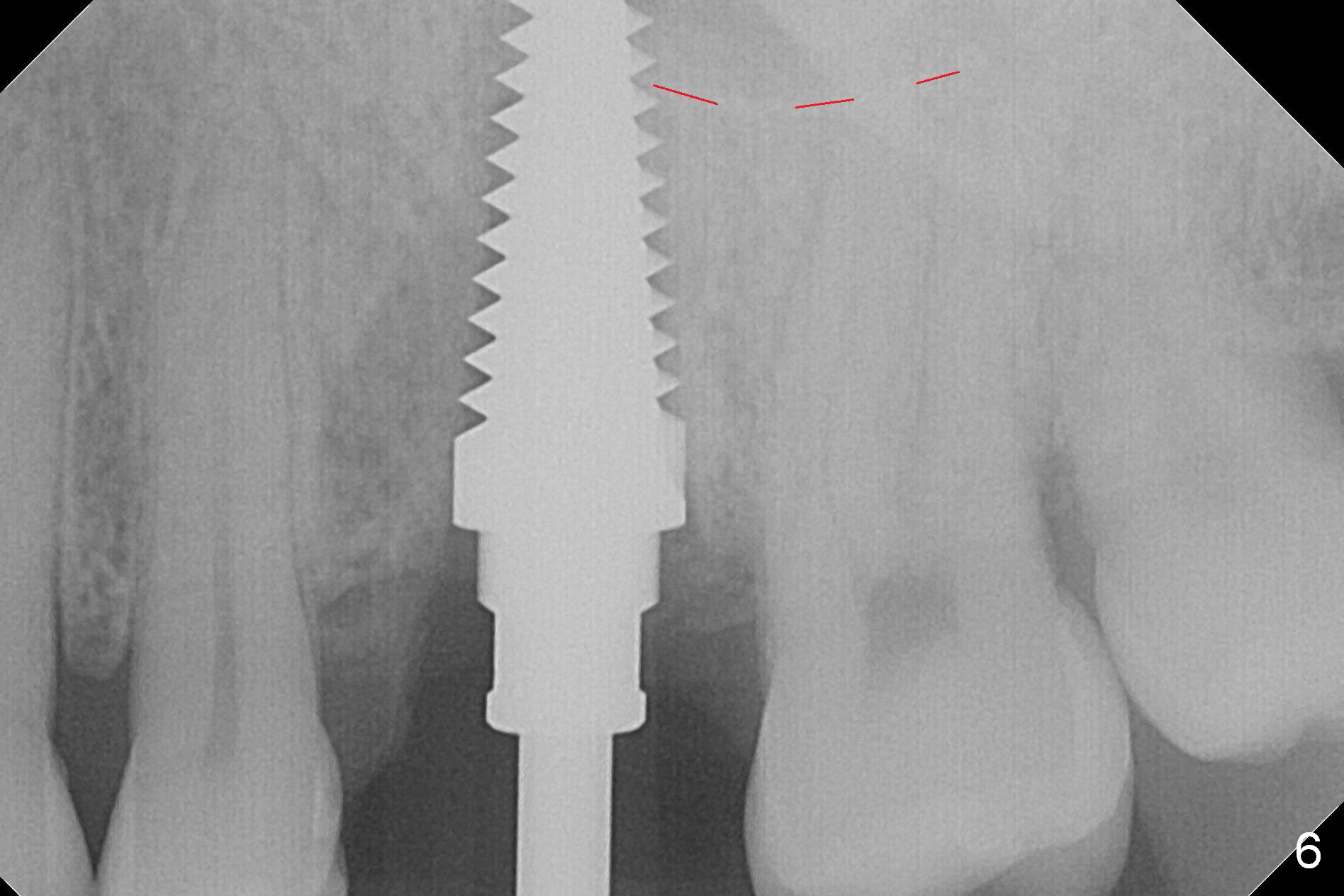
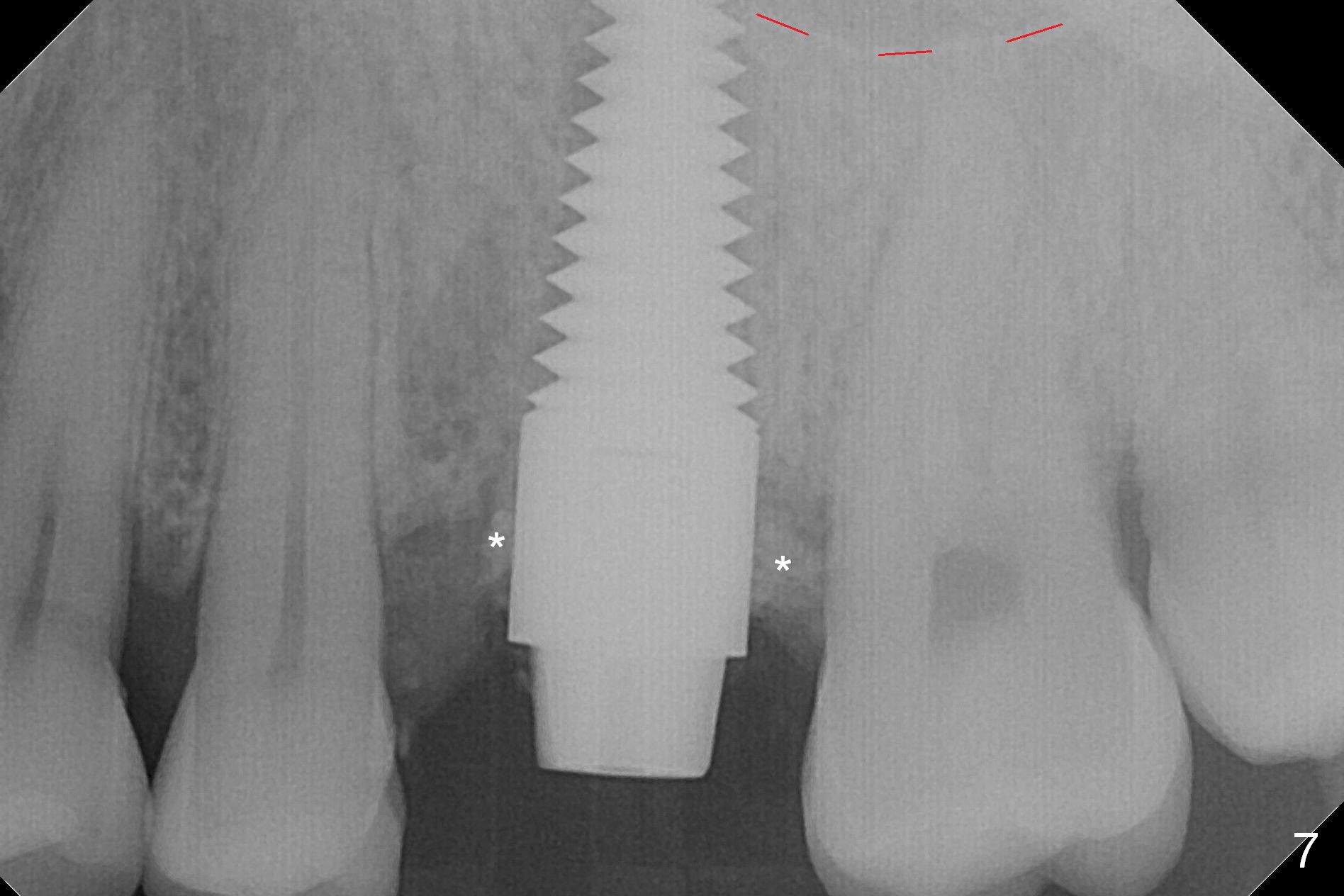
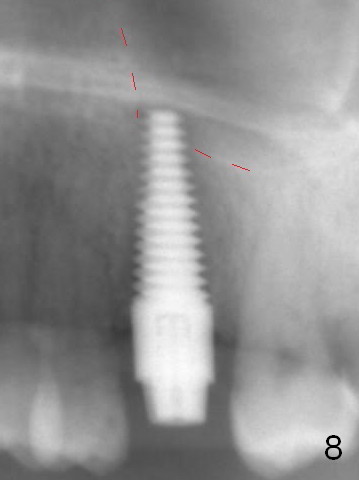
The septum perforates into the distobuccal socket when 4.3 mm drill is being used. The sinus floor bone (Fig.5 *, Fig.6-8 red dashed line) has to be used for primary stability. Finally a 6x20 mm tap achieves stability apparently by engaging to the mesial and distal walls of the socket (Fig.6). The insertion torque of a 6x20 mm tissue-level implant is > 60 Ncm (Fig.7) with allograft packed into the remaining socket (*).
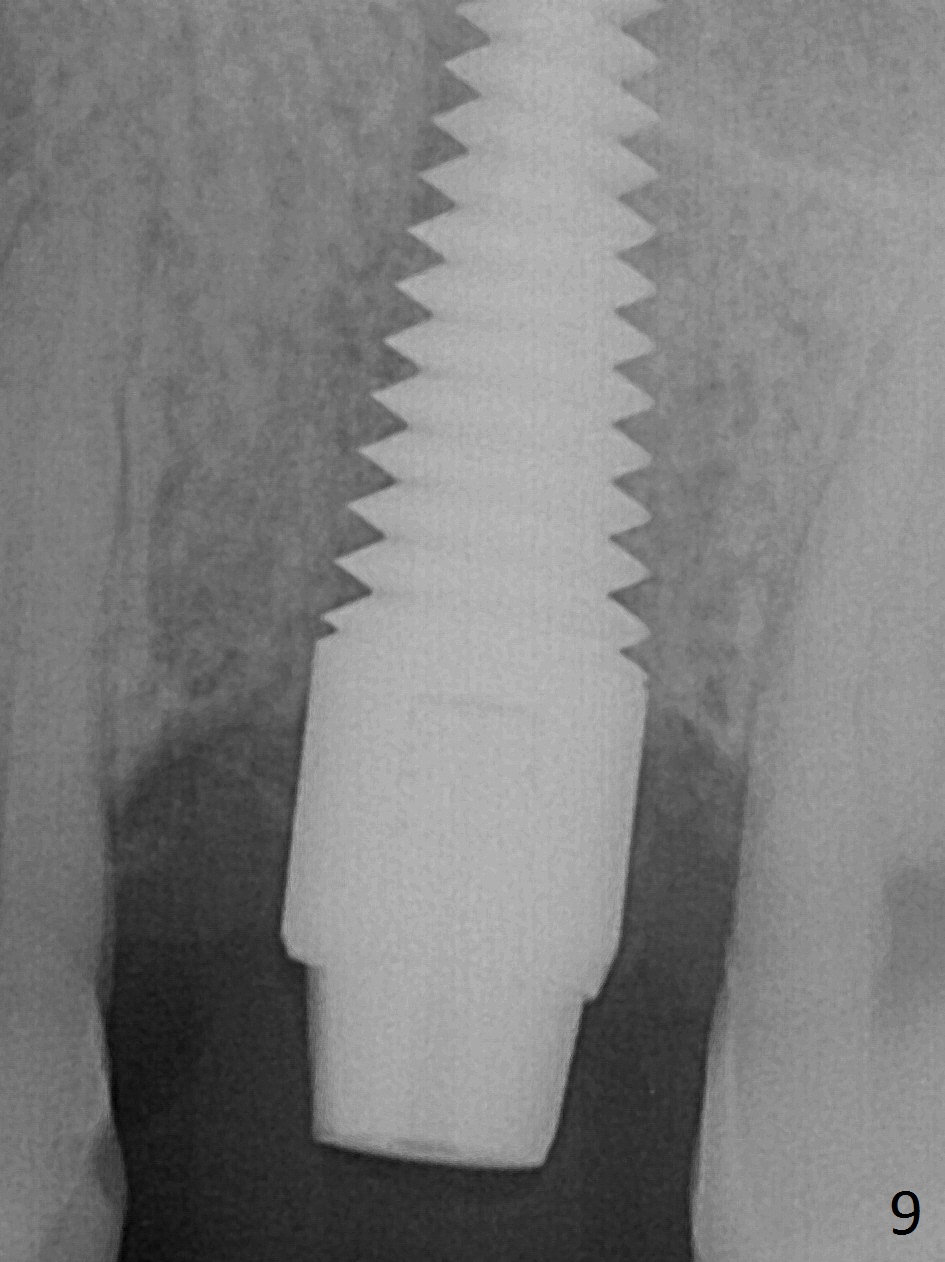
A much smaller implant should be used (e.g.4.5 mm) in order to save the septum. But the apical granulation tissue above the septum cannot be removed completely. There is no bone loss around the implant 4 months postop (Fig.9), although the gingiva is unhealthy because of lack of oral hygiene locally. The immediate provisional is not reseated with oral hygiene instruction. Impression will be taken in 2 weeks. Take photos to show disappearance of the fistula.
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), IBS
Xin Wei, DDS, PhD, MS 1st edition 02/16/2017, last revision 06/14/2017