%20mm,%20graft,%202.7%20mm%20into%20sinus.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|||
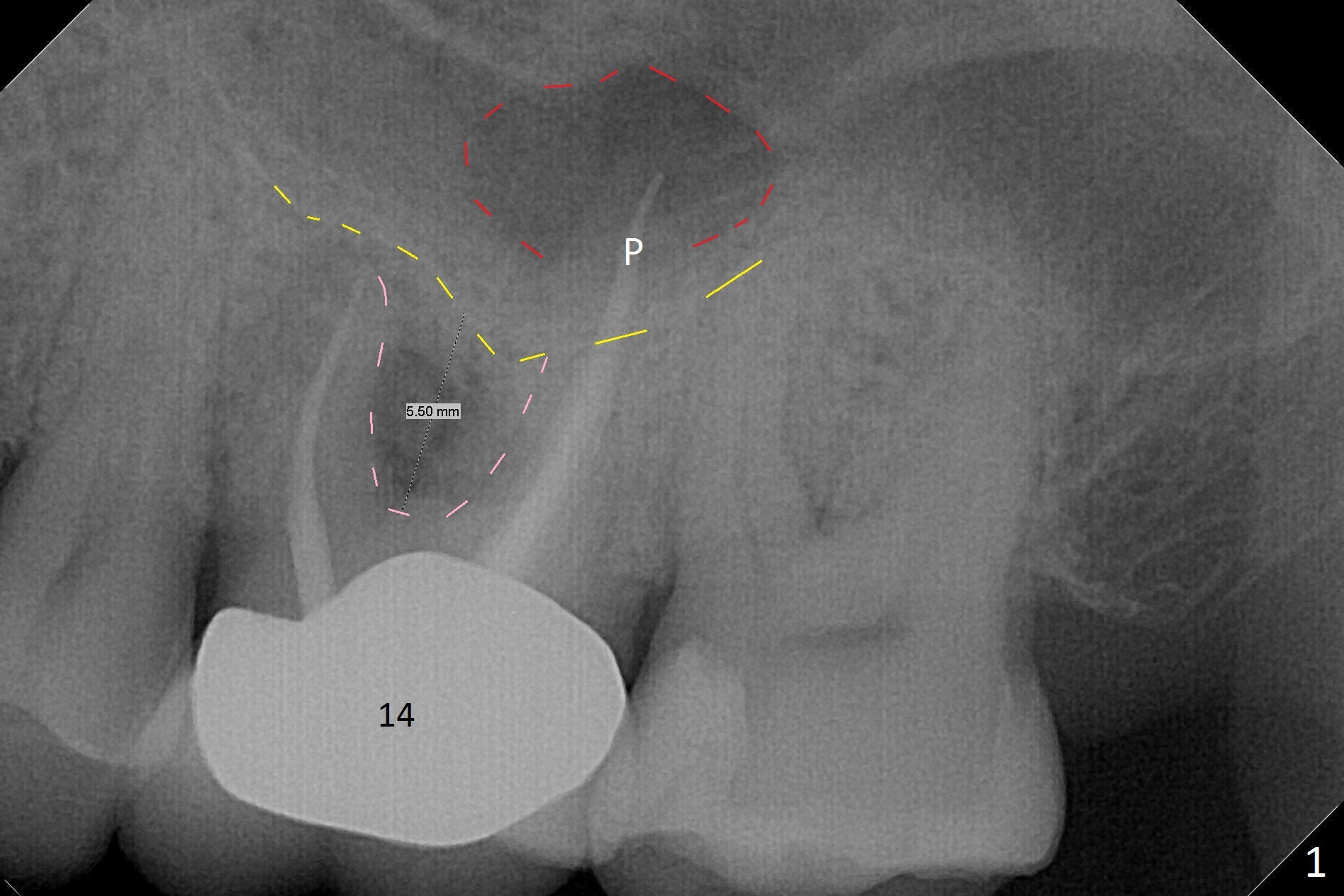
Initial Osteotomy Should be Below Sinus Floor
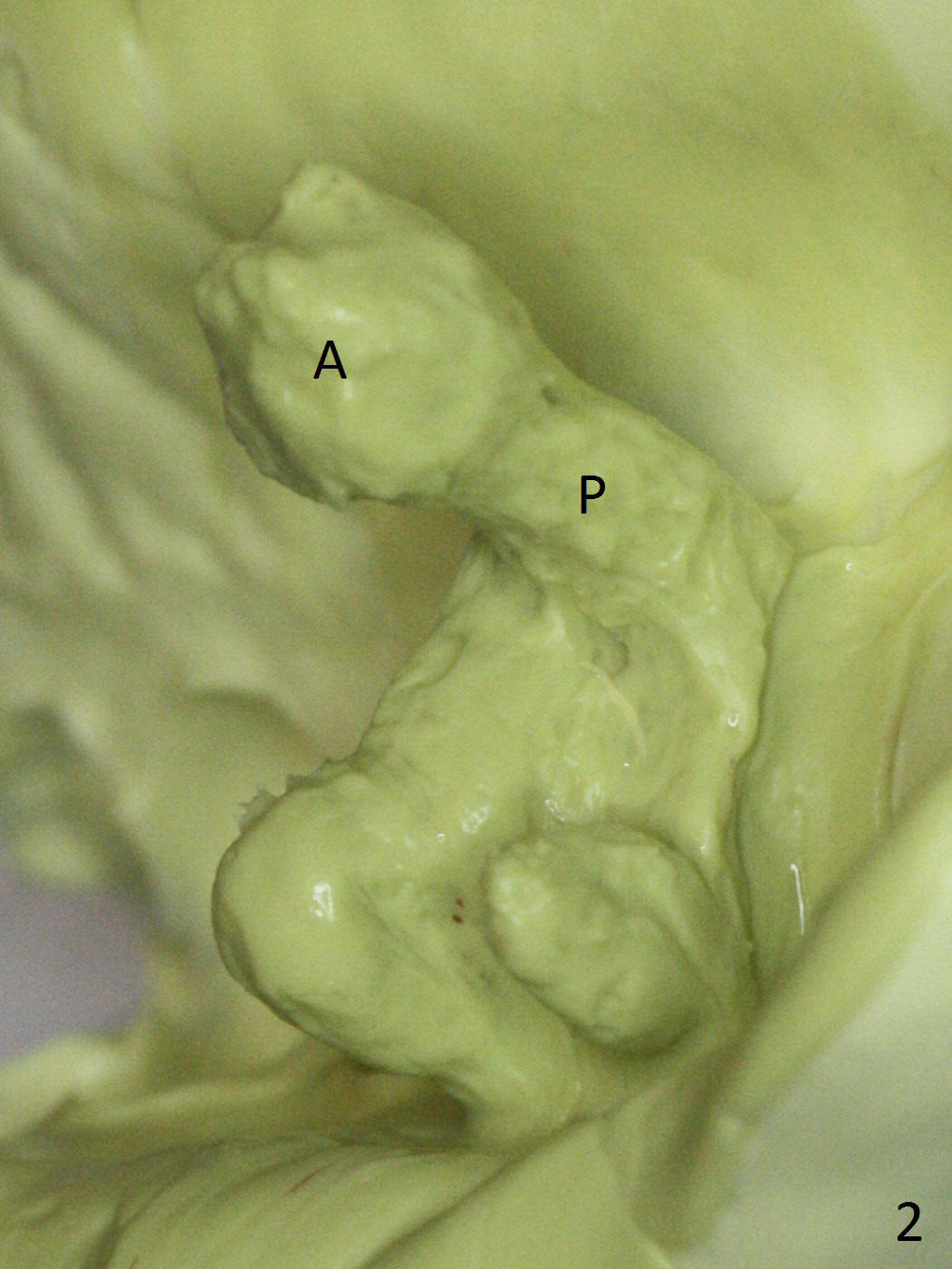
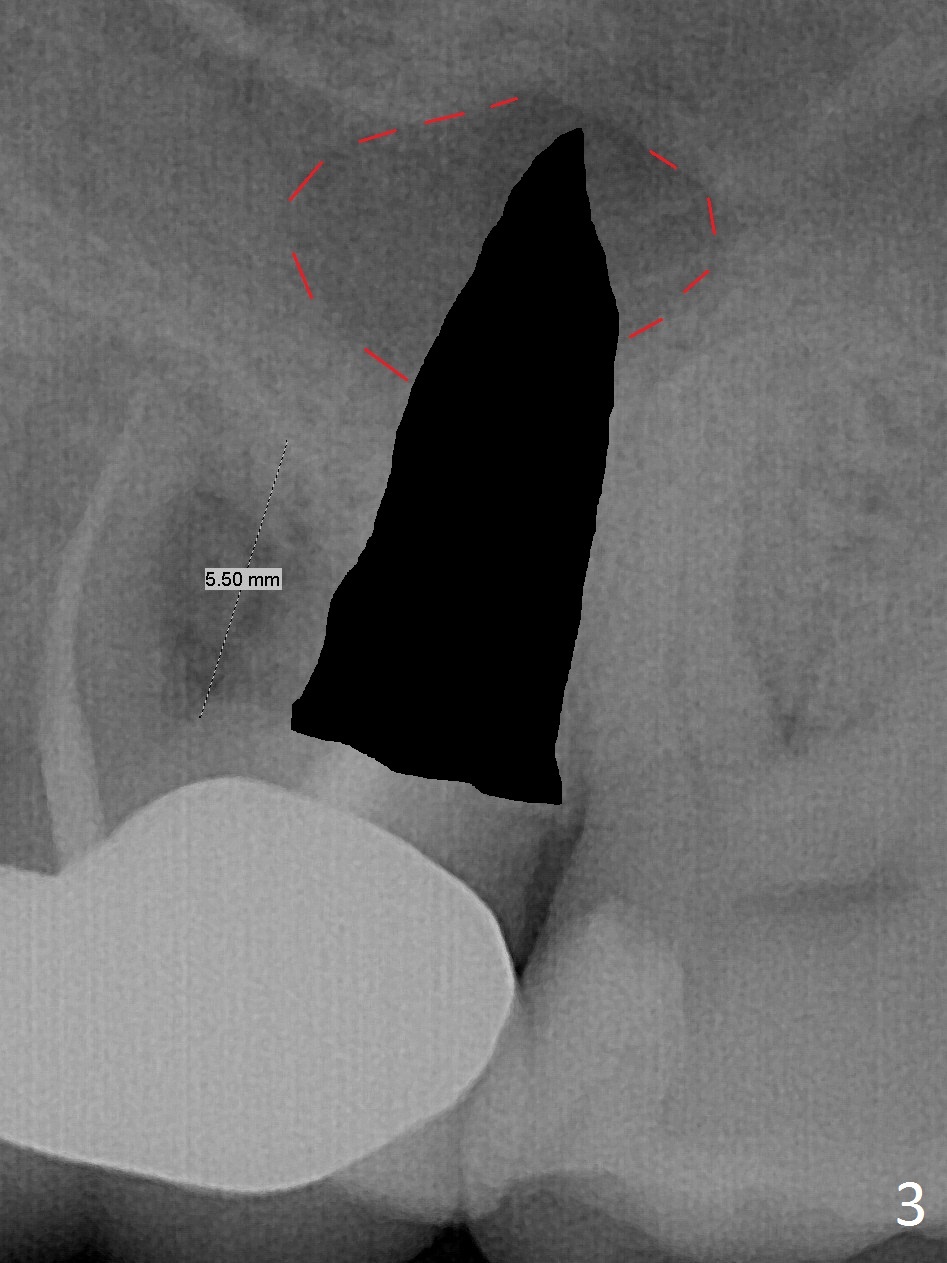
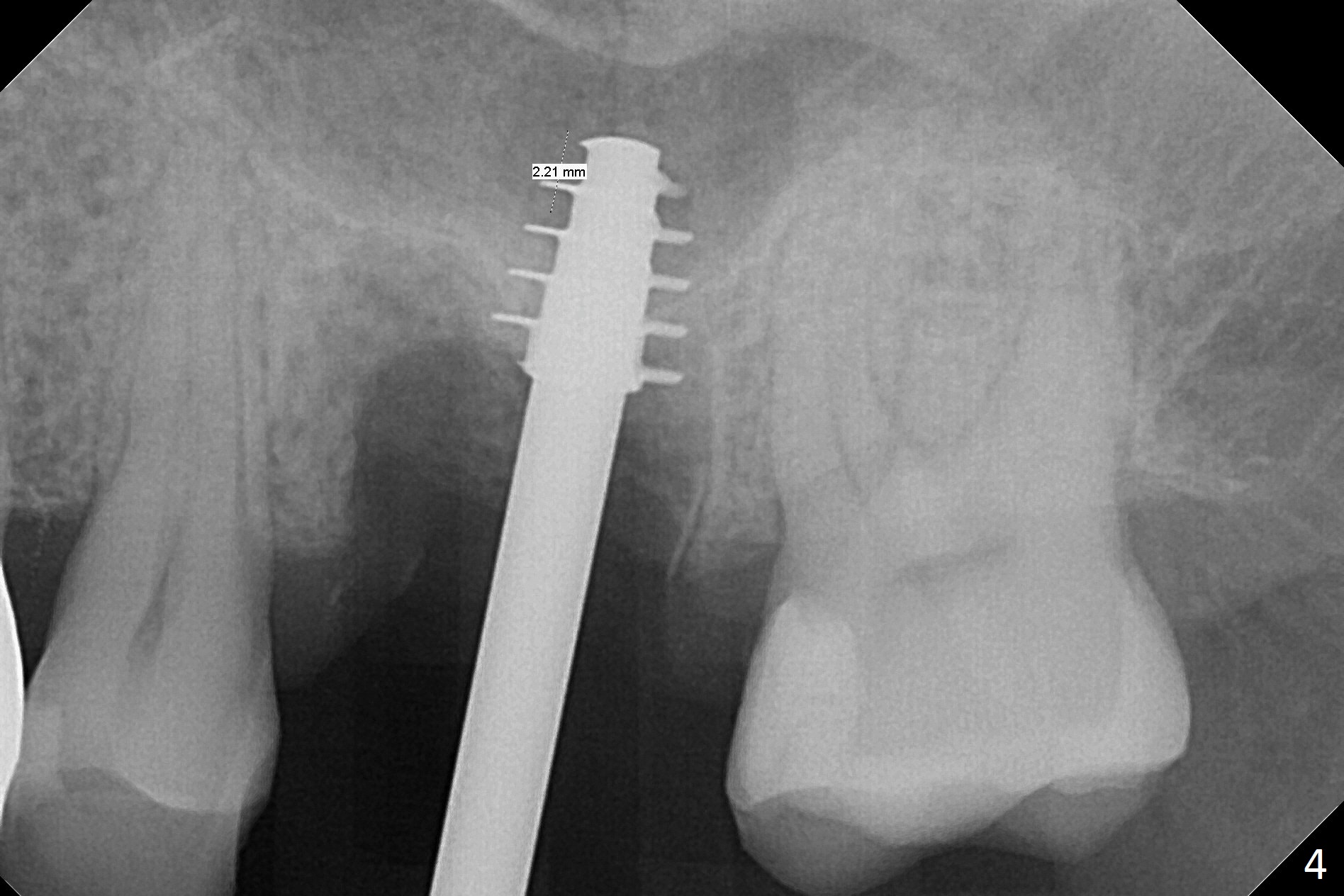
What is unclear preop is the large periapical radiolucency (Fig.1 red dashed line) of the palatal root (P) of the tooth #14. When the tooth is extracted, it is difficult to remove granulation tissue from the palatal apical socket, which is enlarged (Fig.2 (impression of sockets),3). The small dimension of the septum (~4x5 mm (Fig.1 pink) is also unrecognized preop, which leads to sinus perforation when 4.8 mm Magic Drill is used. In spite of use of PRF plug and membrane, allograft does not stay in the osteotomy after placement of 4x11 mm dummy implant or 5 mm tap drill (Fig.4 for 9 mm). Finally a 5.5x7 mm IBS implant is placed with 30 Ncm (Fig.5). After placement of Osteogen plug in the apical portion of the sockets, allograft/Osteogen is placed in the remaining sockets (Fig. 5 *). The latter is partially contained by a 6.5x4(3) mm abutment (A) and ultimately by an immediate provisional.
To avoid sinus membrane perforation, the initial osteotomy should be coronal to the sinus floor by 1 mm.
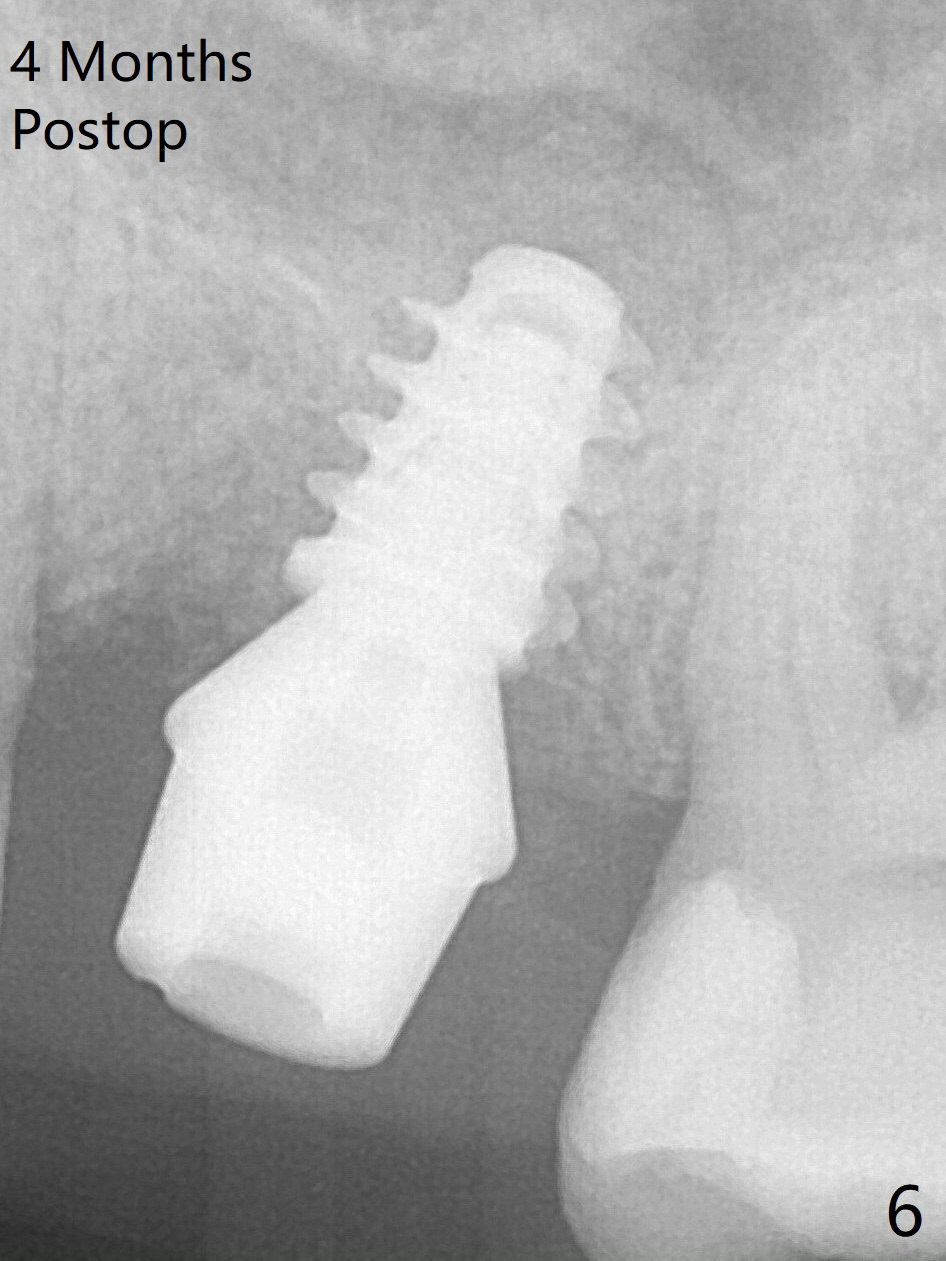
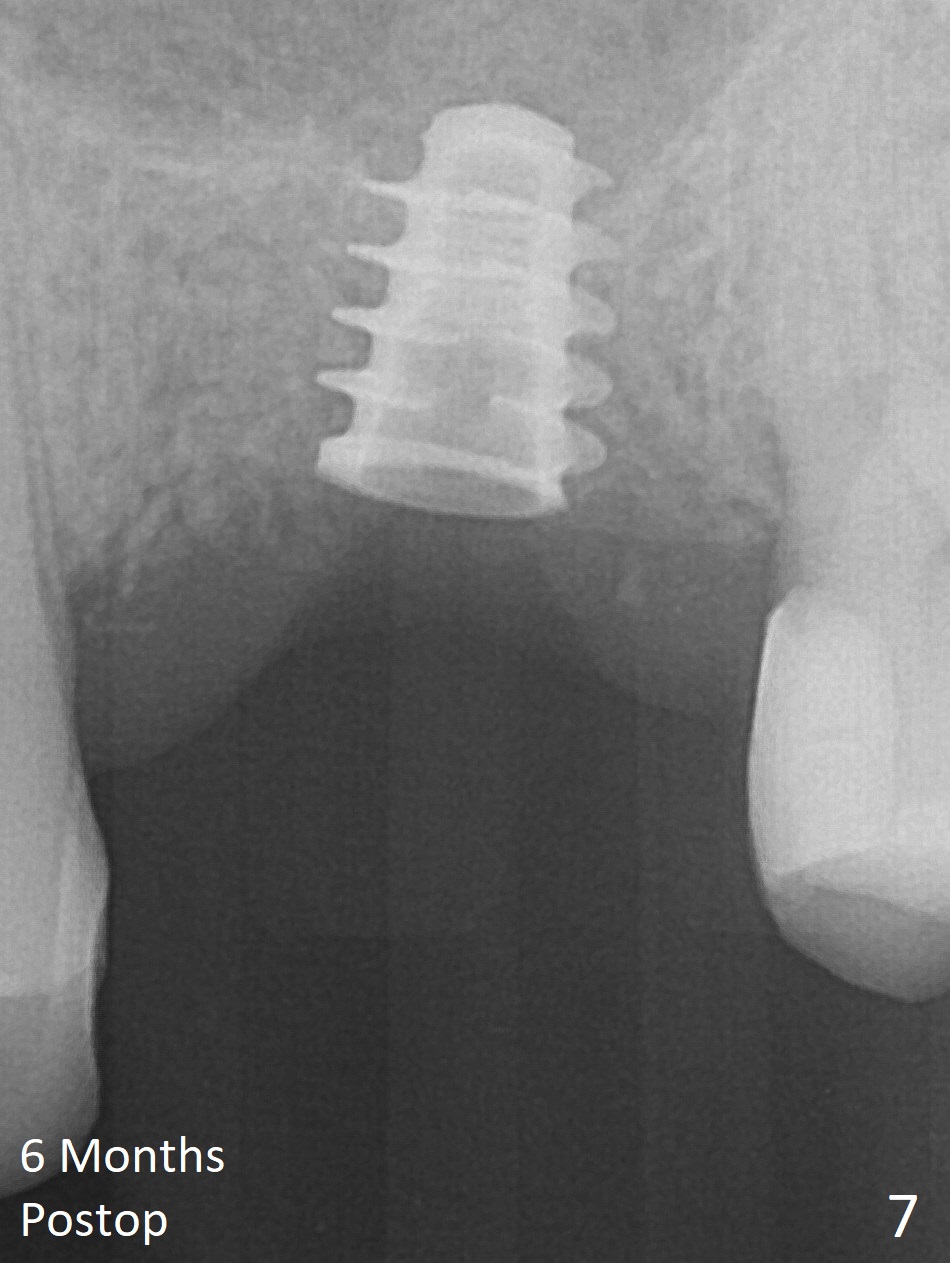
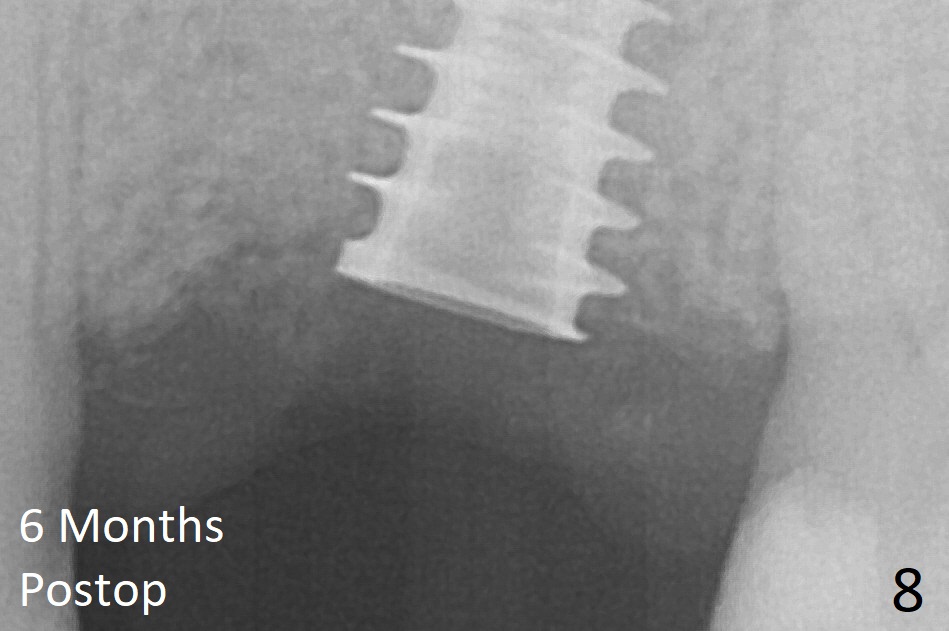
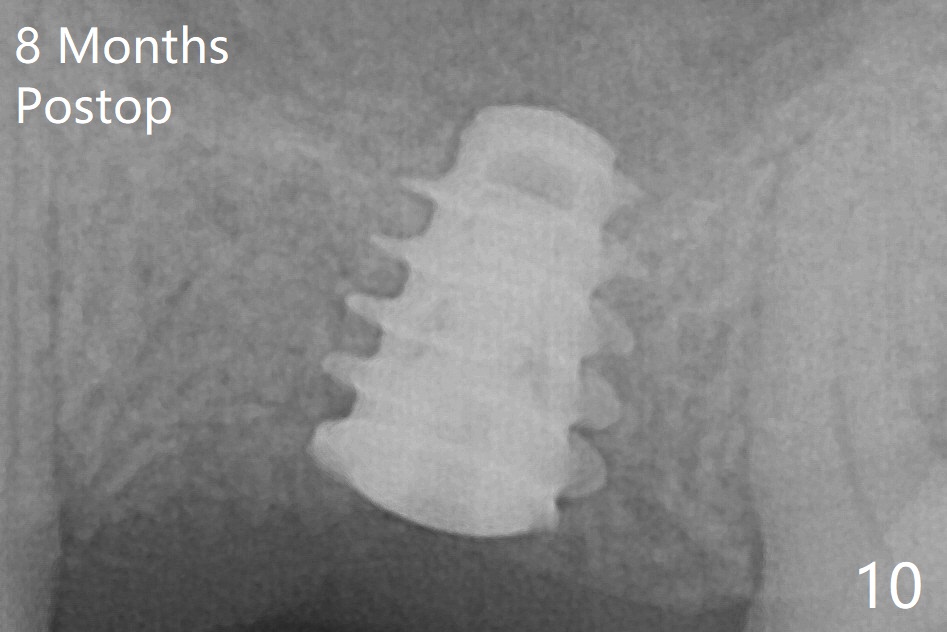
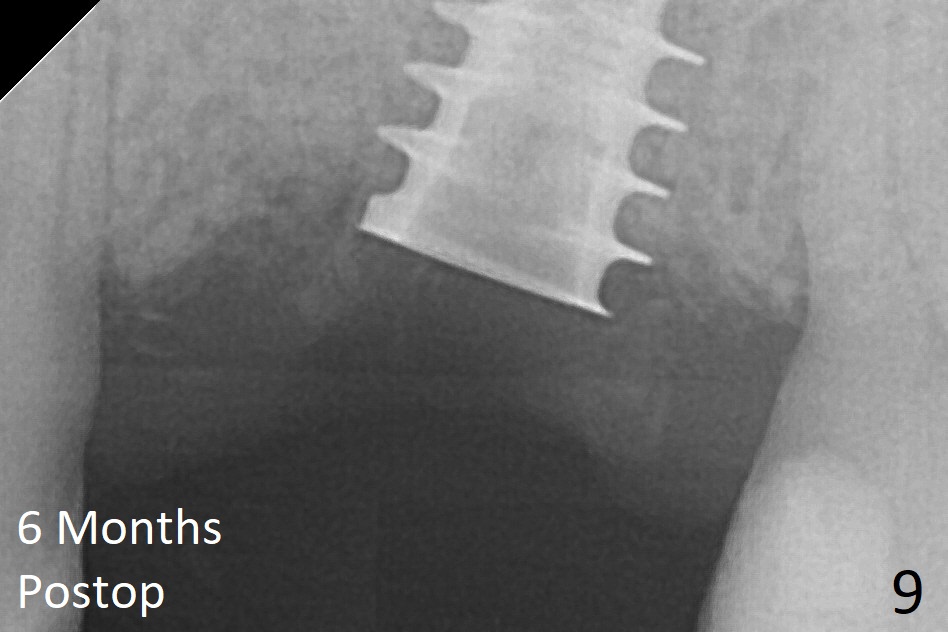
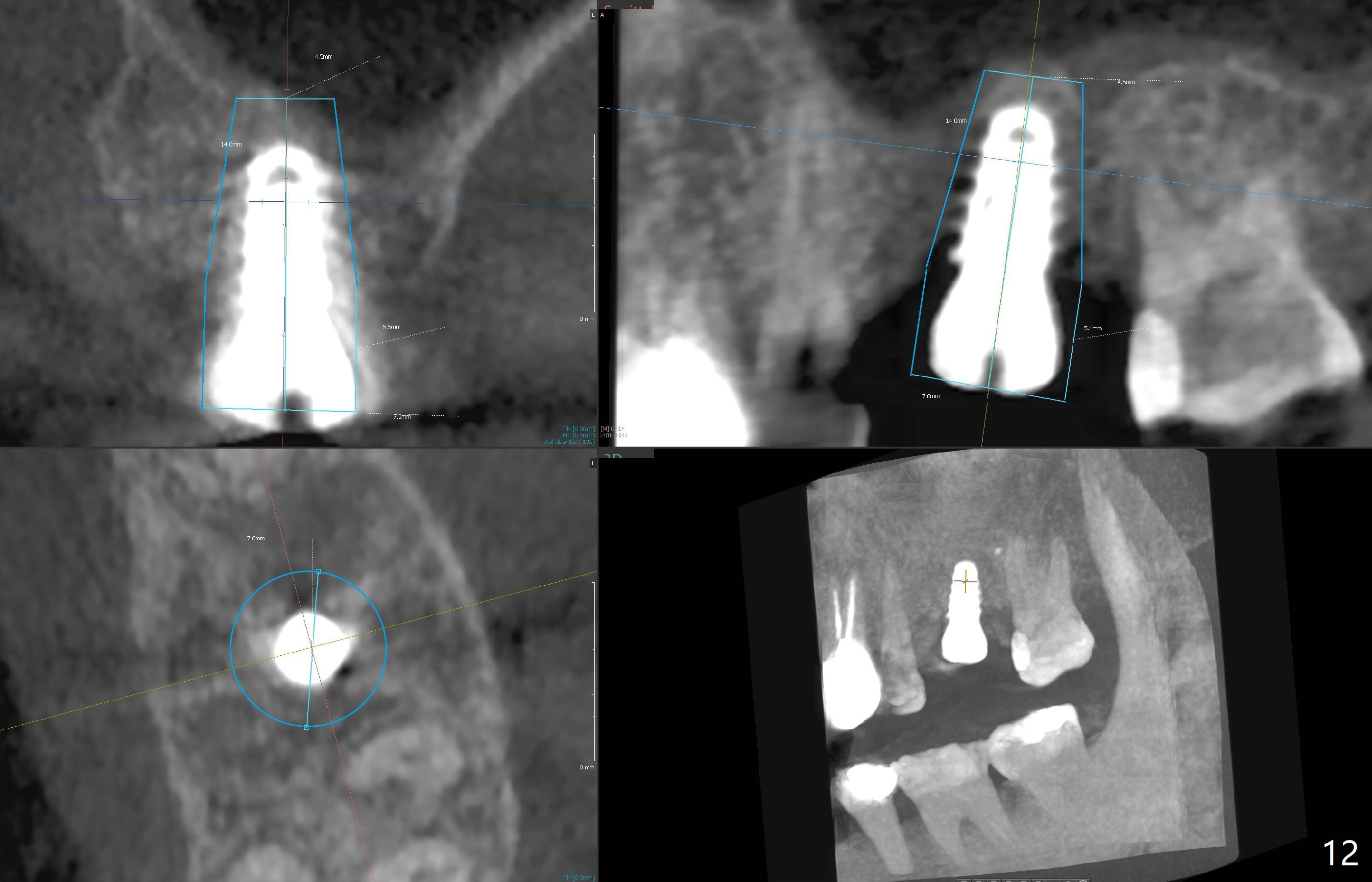
The implant is mobile 4 months postop (Fig.6). A 6x2 mm healing abutment is placed next. Although the implant remains mobile 6 months postop, the bone seems to have become denser around the implant (Fig.7-9). A healing screw is placed. When the bone height is limited (<7 mm), place a larger implant (>5.5 mm). The implant seems to have osteointegrated 8 months postop (Fig.10). Impression is taken following placing a 6.5x4(3) mm abutment. The patient reports pain after cementation, which is less when the abutment screw is loose (9.5 months postop, 2 weeks post cementation). CBCT taken after placement of a healing screw apparently shows loose bone mesial and distal to the implant (Fig.11 *). The implant trajectory is less favorable. It seems necessary to change to a large implant with more sold threads (Fig.12).
In fact, the patient insists upon removing the loose implant. Ten months postop, the healing abutment seems unstable. When it is removed, the tissue looks healthy and the implant is apparently stable. After discussion, a healing screw is placed. He will return for follow up in 2 months.
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), Course
1
2
Xin Wei, DDS, PhD, MS 1st edition 06/13/2017, last revision 04/18/2018