
%20abutment,%202nd%20round%20of%20bone%20graft.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
Complete Fill of Bony Defect
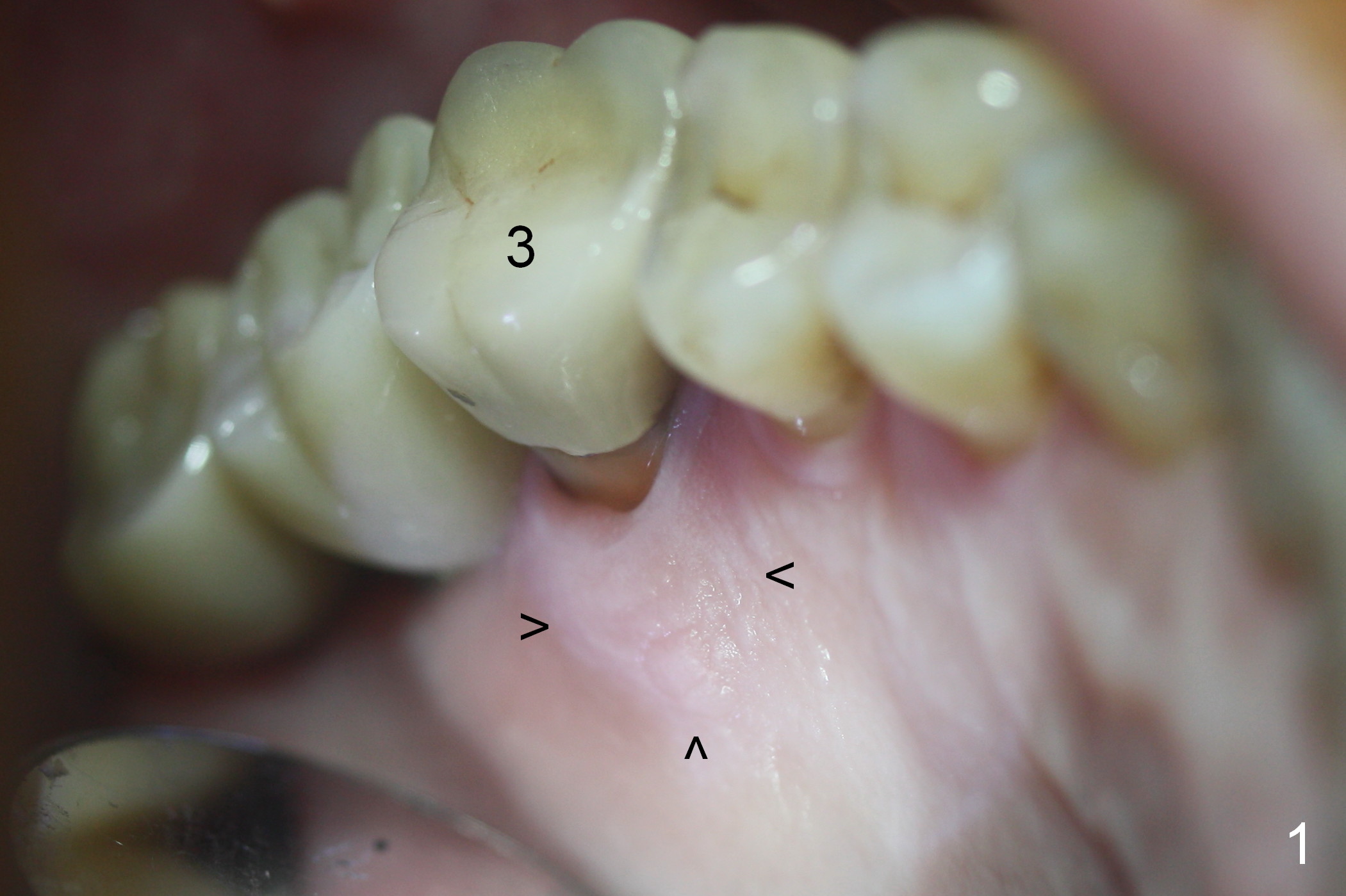
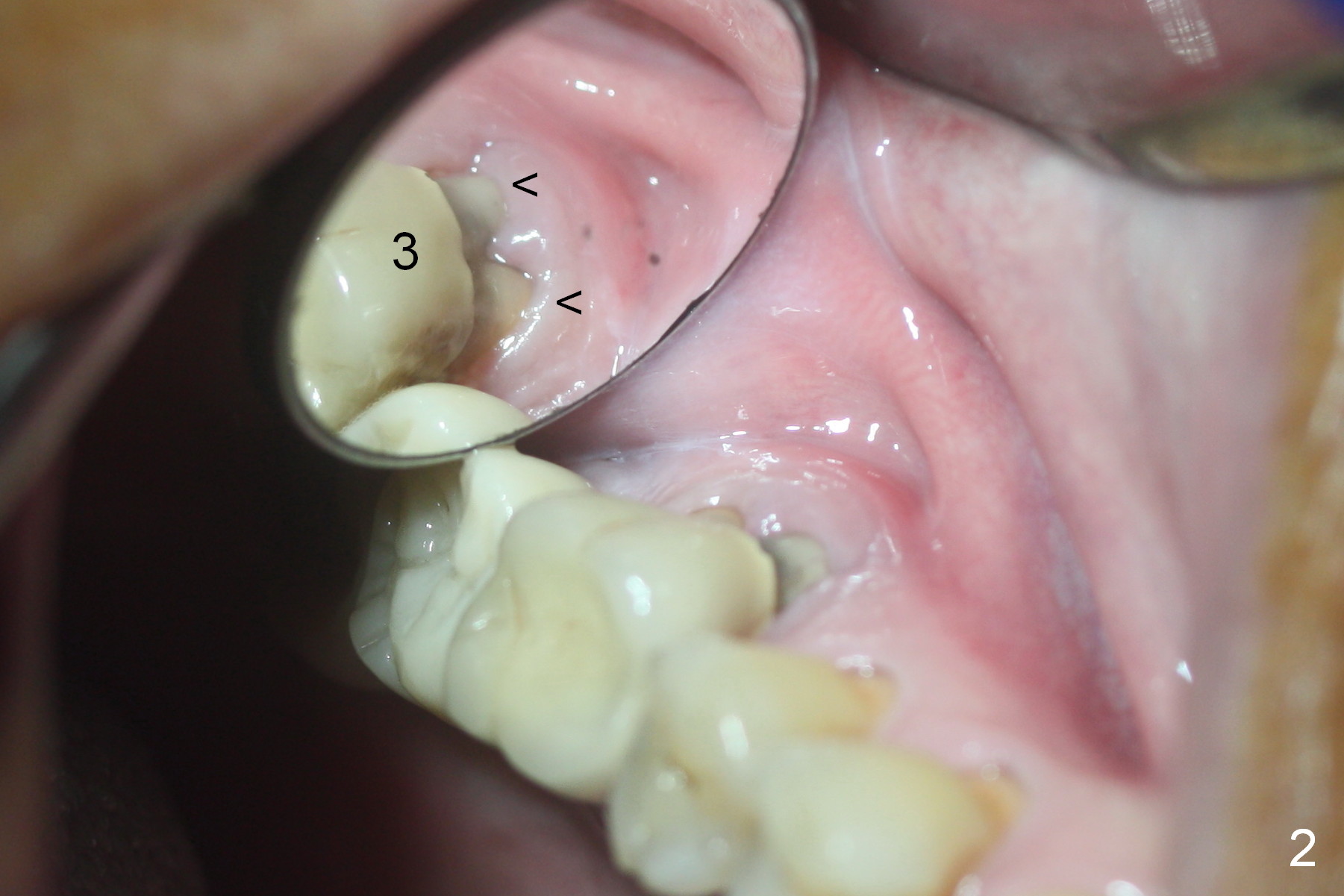
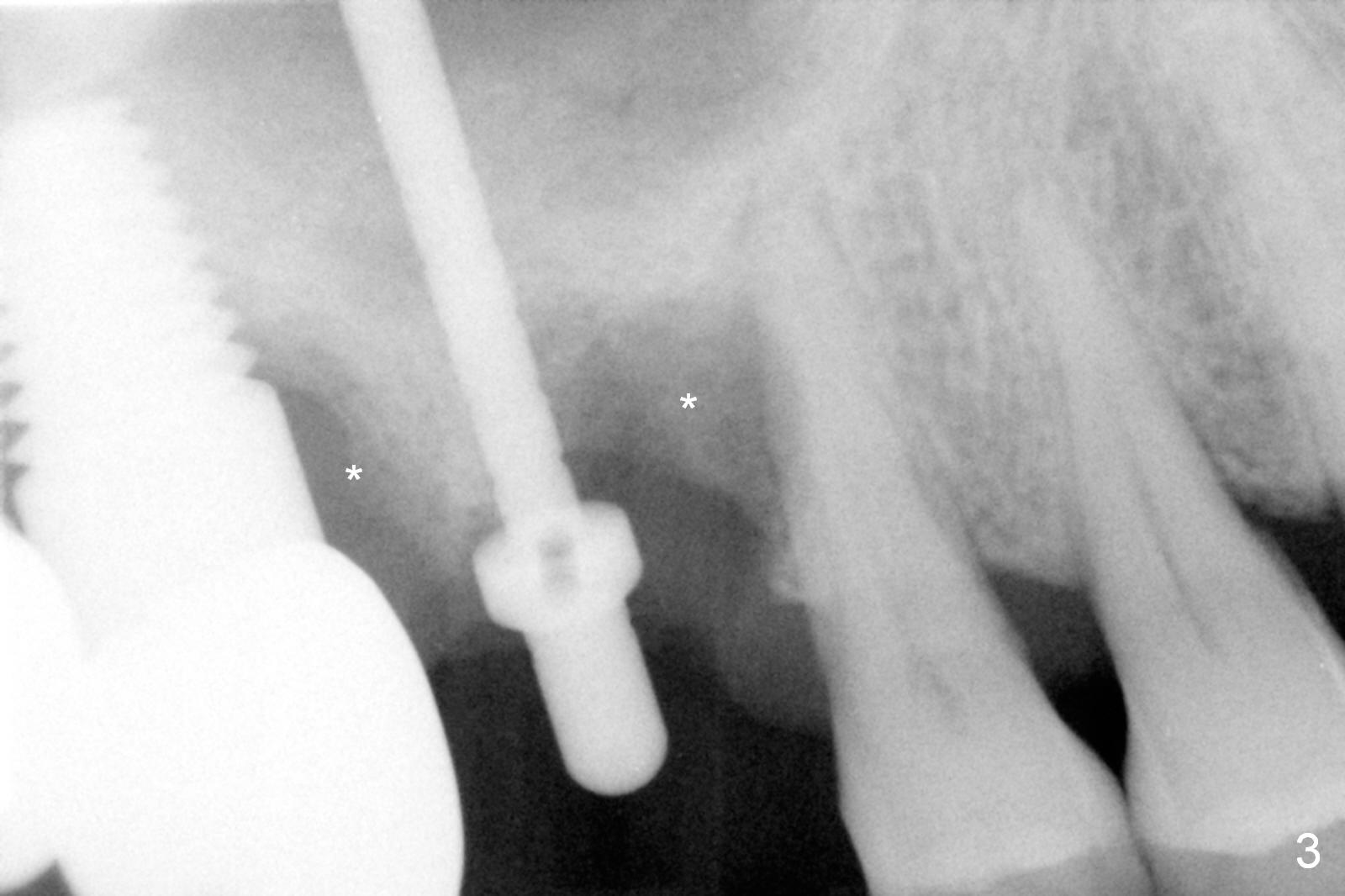
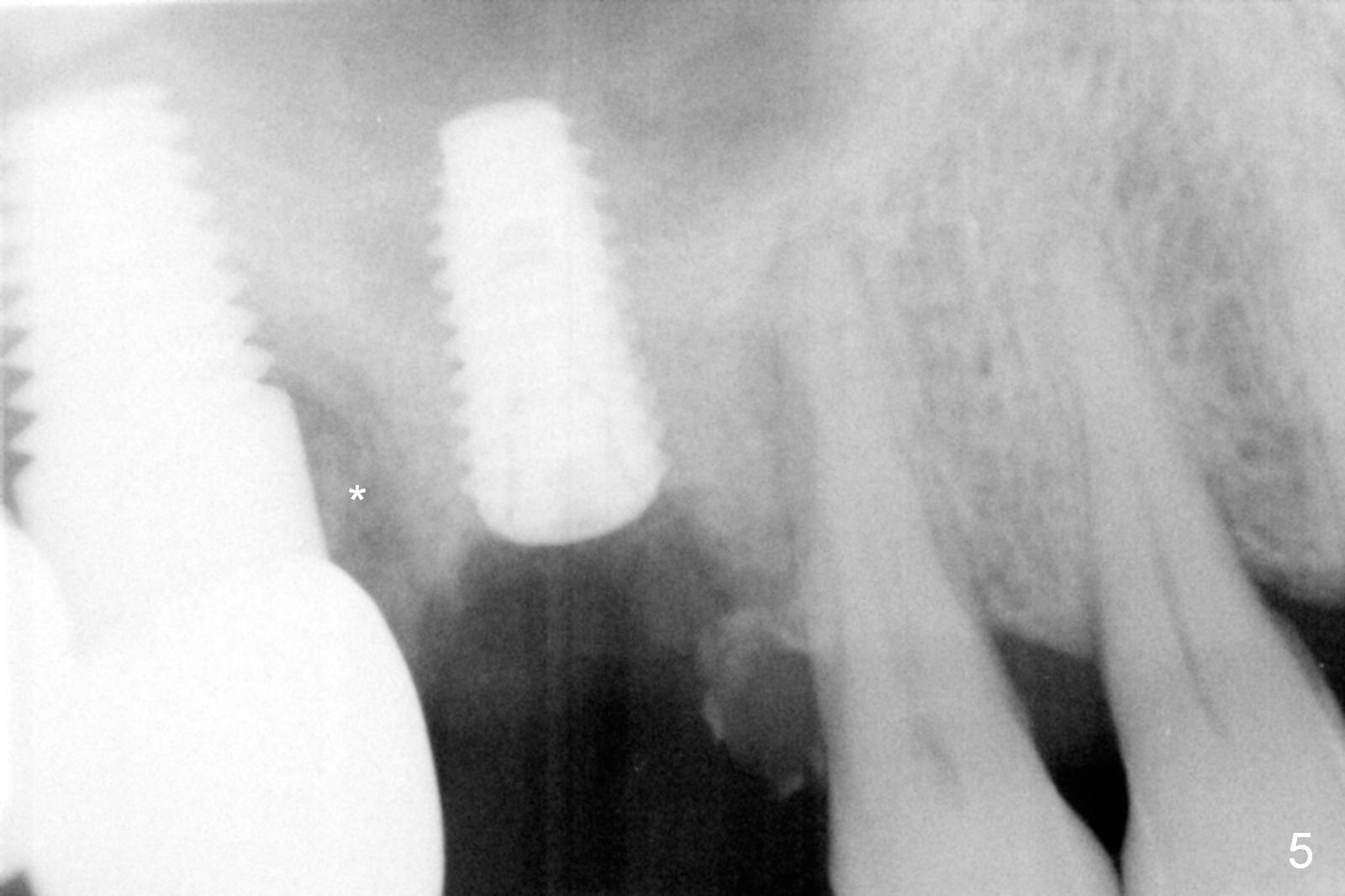
The patient returns for the tooth #3 extraction and immediate implant because of severe pain associated with the palatal swelling (Fig.1 arrowheads). There is moderate buccal gingival recession (Fig.2 <). Therefore the coronal portion of the buccal and palatal plates are defective. The septum is the site of osteotomy; its height is shorter than expected. After a 2 mm pilot drill is used for 10 mm, a parallel pin enters for 14 mm, suggesting sinus floor perforation (Fig.3). Subsequent osteotomy is confined to 8 mm (Fig.4). Note extensive bony defects (Fig.3,4 *). Following insertion of collagen plug and allograft with autogenous bone for sinus lift, a 5x10 mm implant is placed with ~35 Ncm (insertion torque); larger size of allograft and Osteogen is placed in the major part of the bony defect (Fig.5). Further placement of the graft fills up the remaining defect (Fig.6), followed by placement of an abutment (6.5x5(4) mm), graft and collagen plug. An immediate provisional is fabricated to close the socket opening.
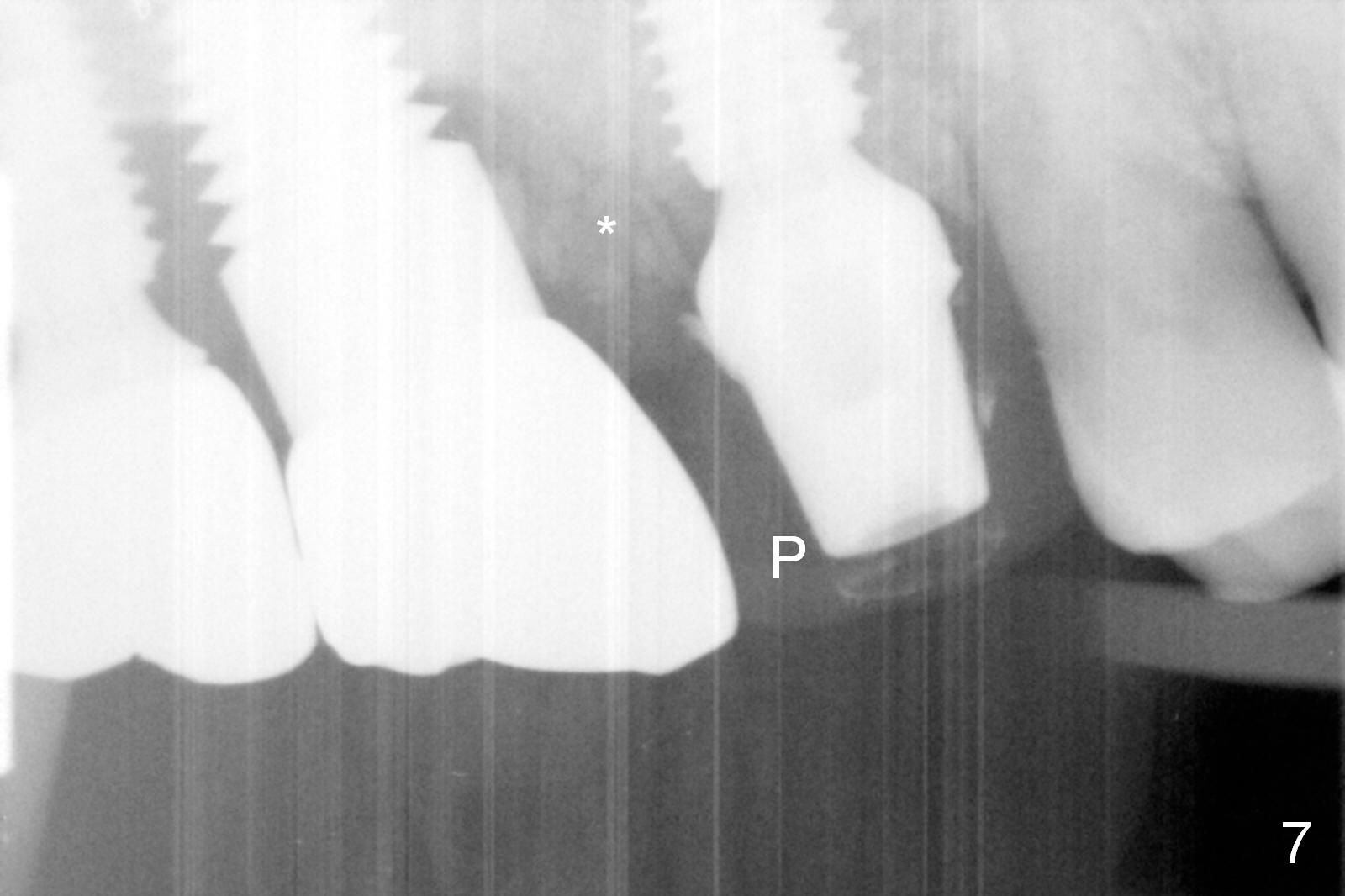
Three months postop, the bone graft remains in place (Fig.7 *), almost completely covered by the healthy gingiva (Fig.8) when the provisional (Fig.7 P) is removed. It appears that long term use of the provisional prevents perfect oral hygiene. It is not recemented. The patient wants to wait for another 4 months for definitive restoration, since insurance benefit runs out for the year.
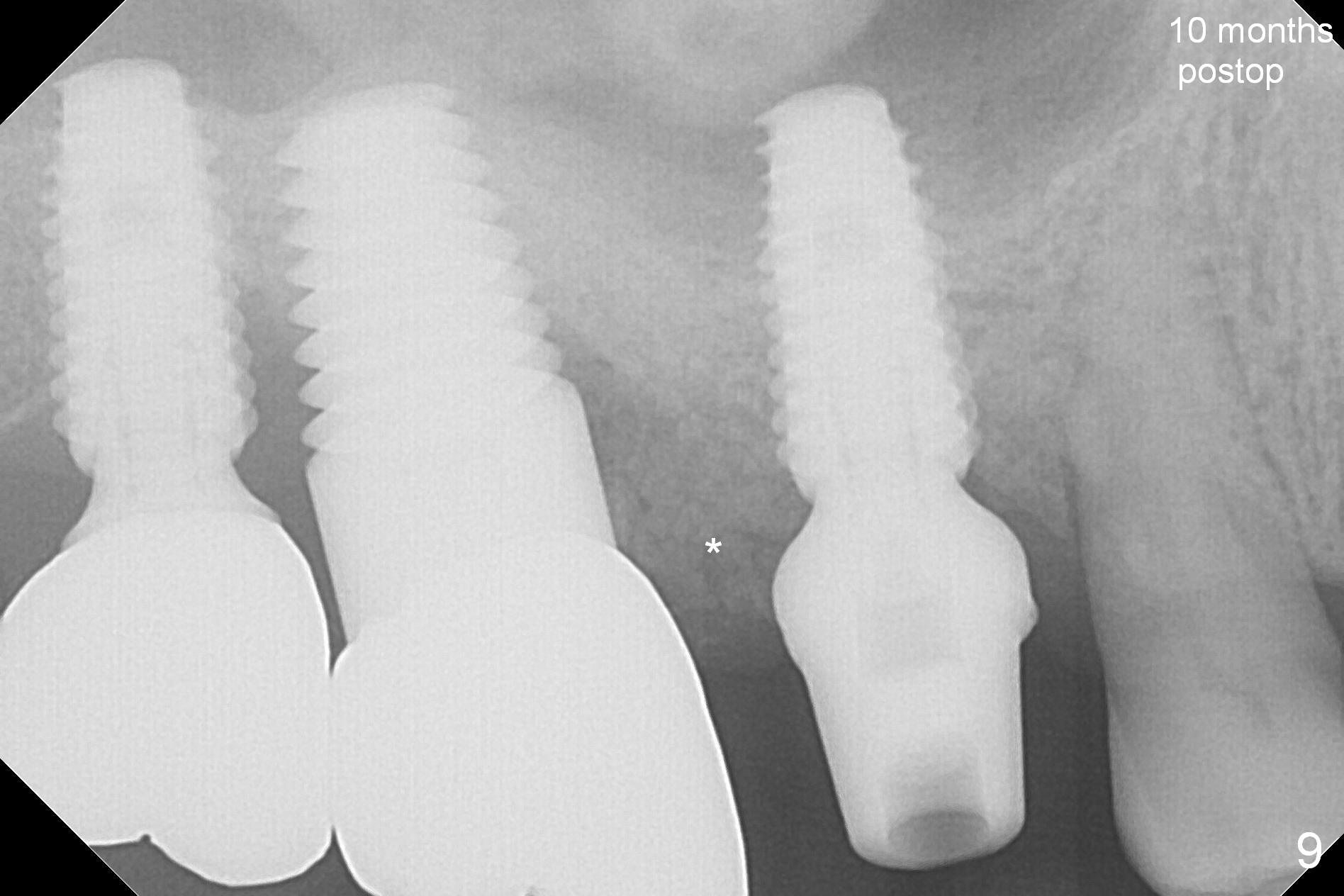
When the patient returns for impression 10 months posotp, the bone between the implants of #2 and 3 is more consolidated (Fig.9 *).
Return to Upper Molar Immediate Implant 14 Xin Wei, DDS, PhD, MS 1st edition 05/20/2016, last revision 12/09/2018