|
|
|
|
|
|
|
|
|
|
Redo Immediate Implant
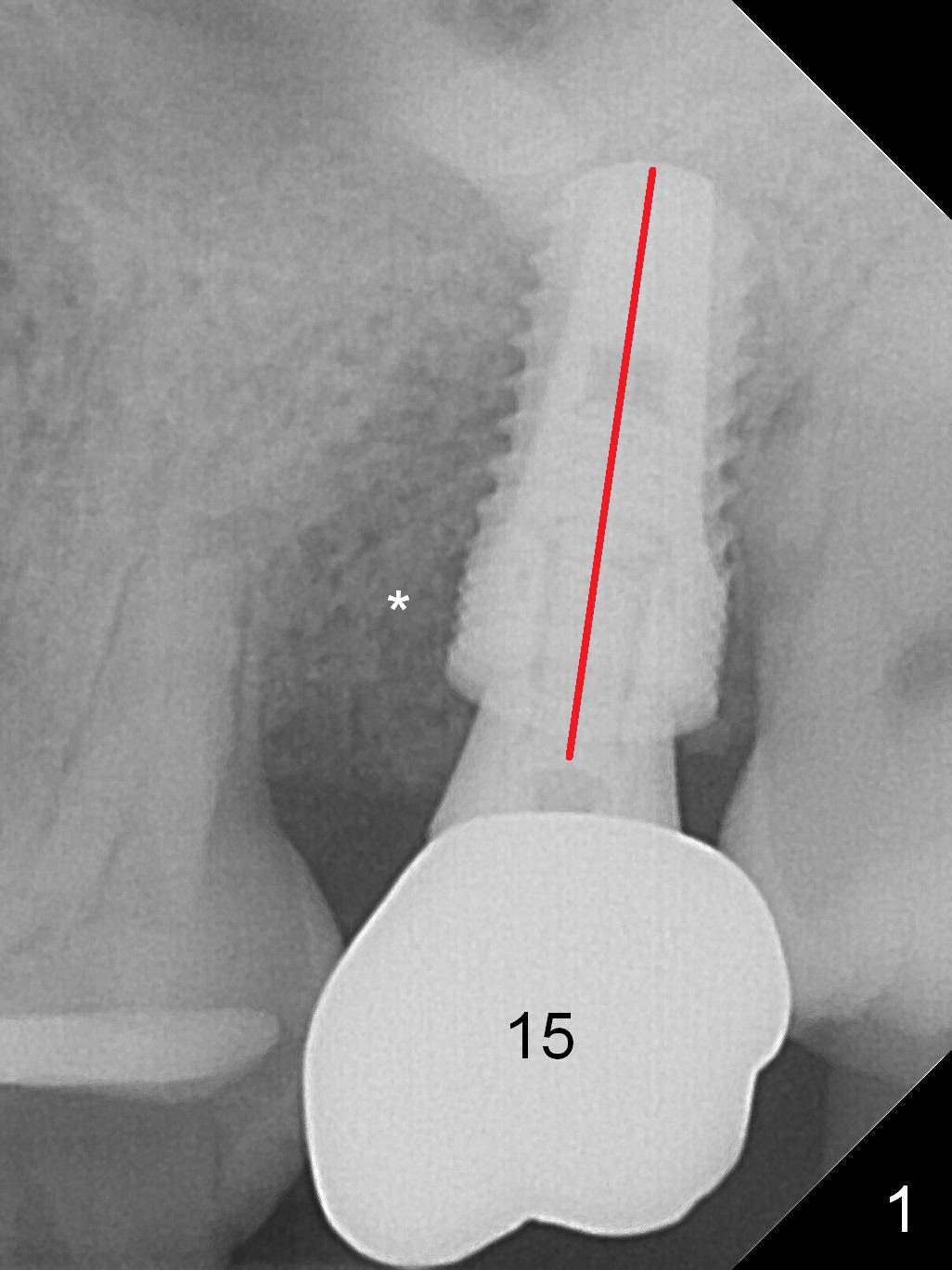
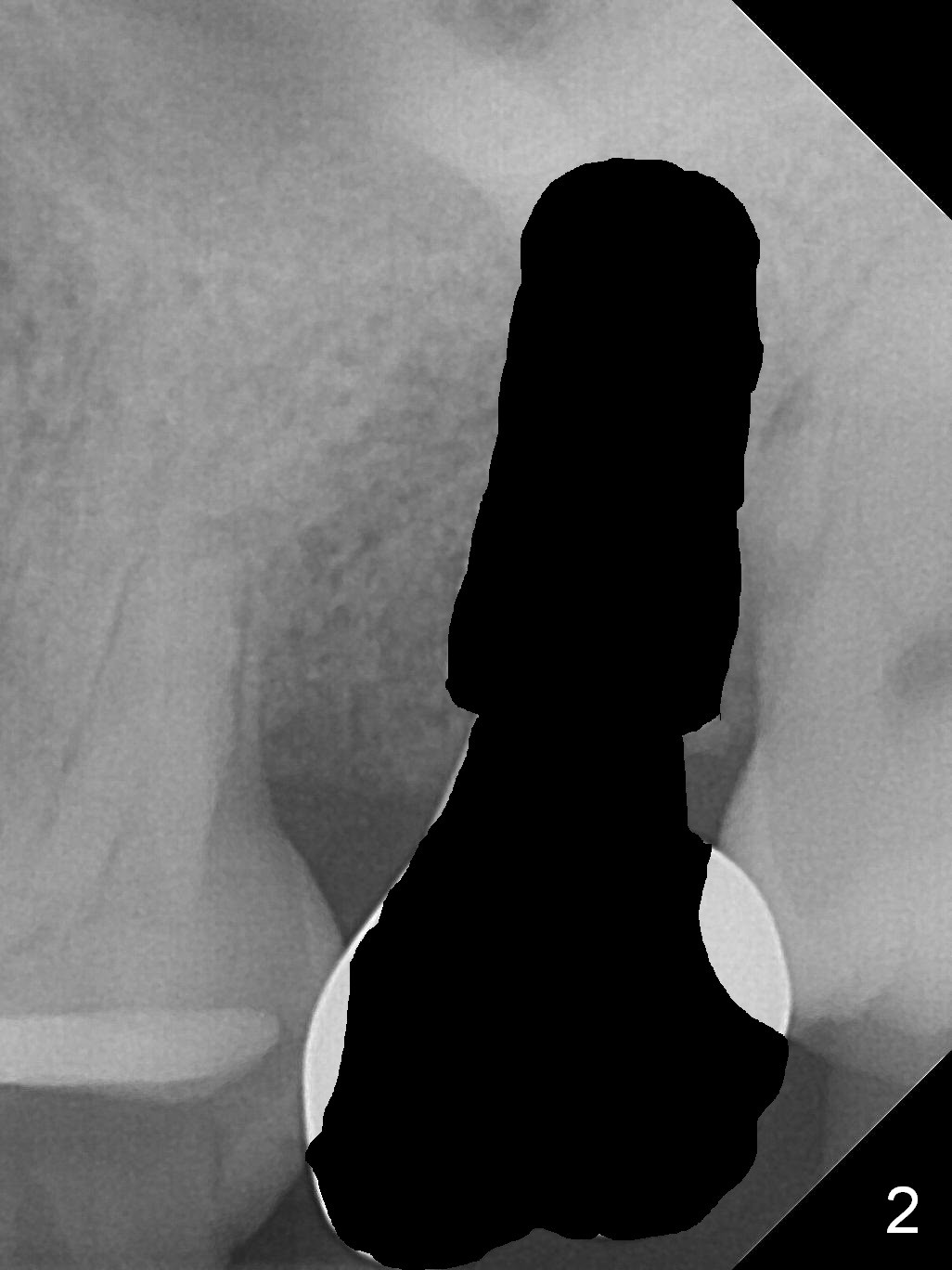
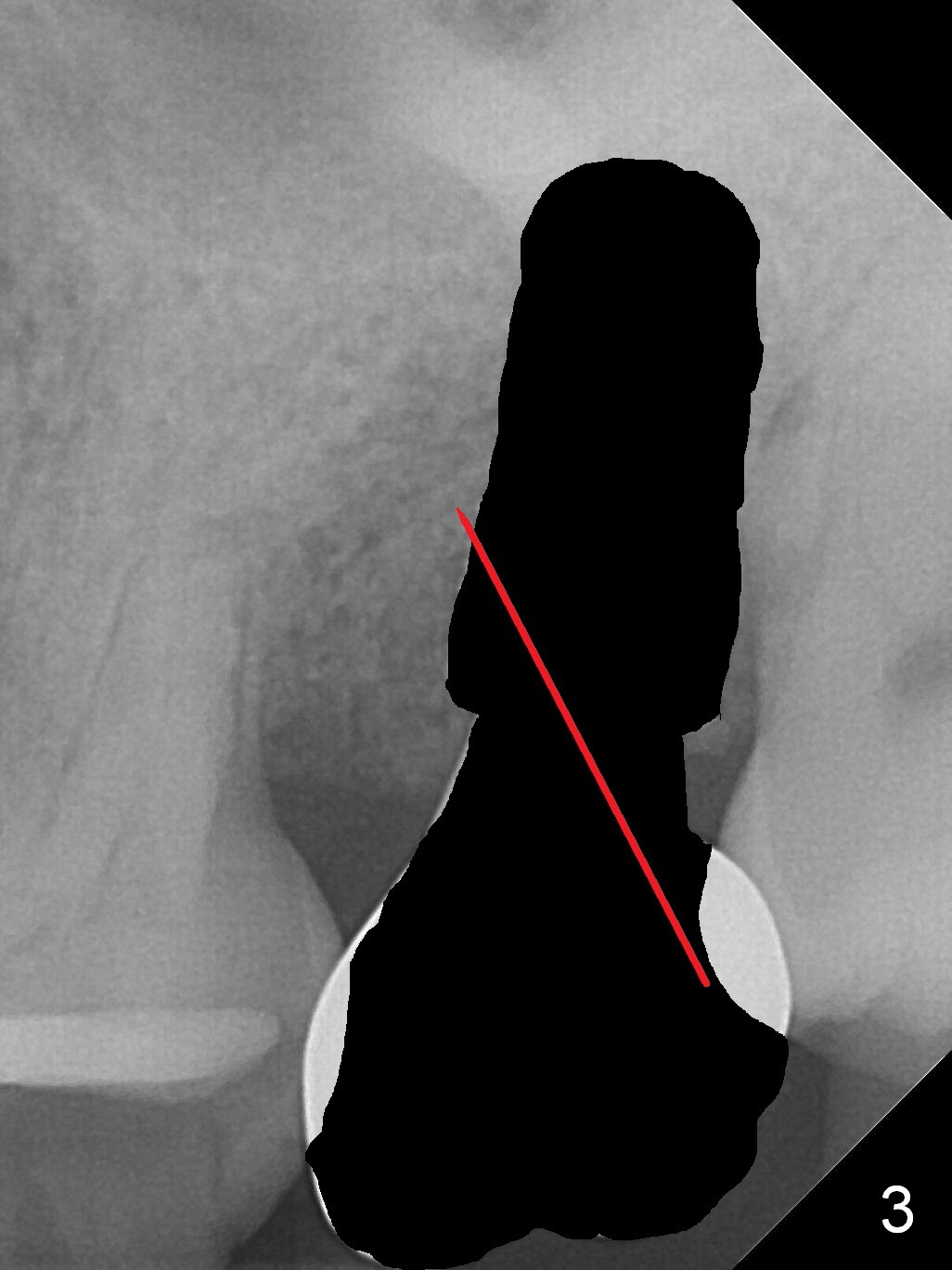
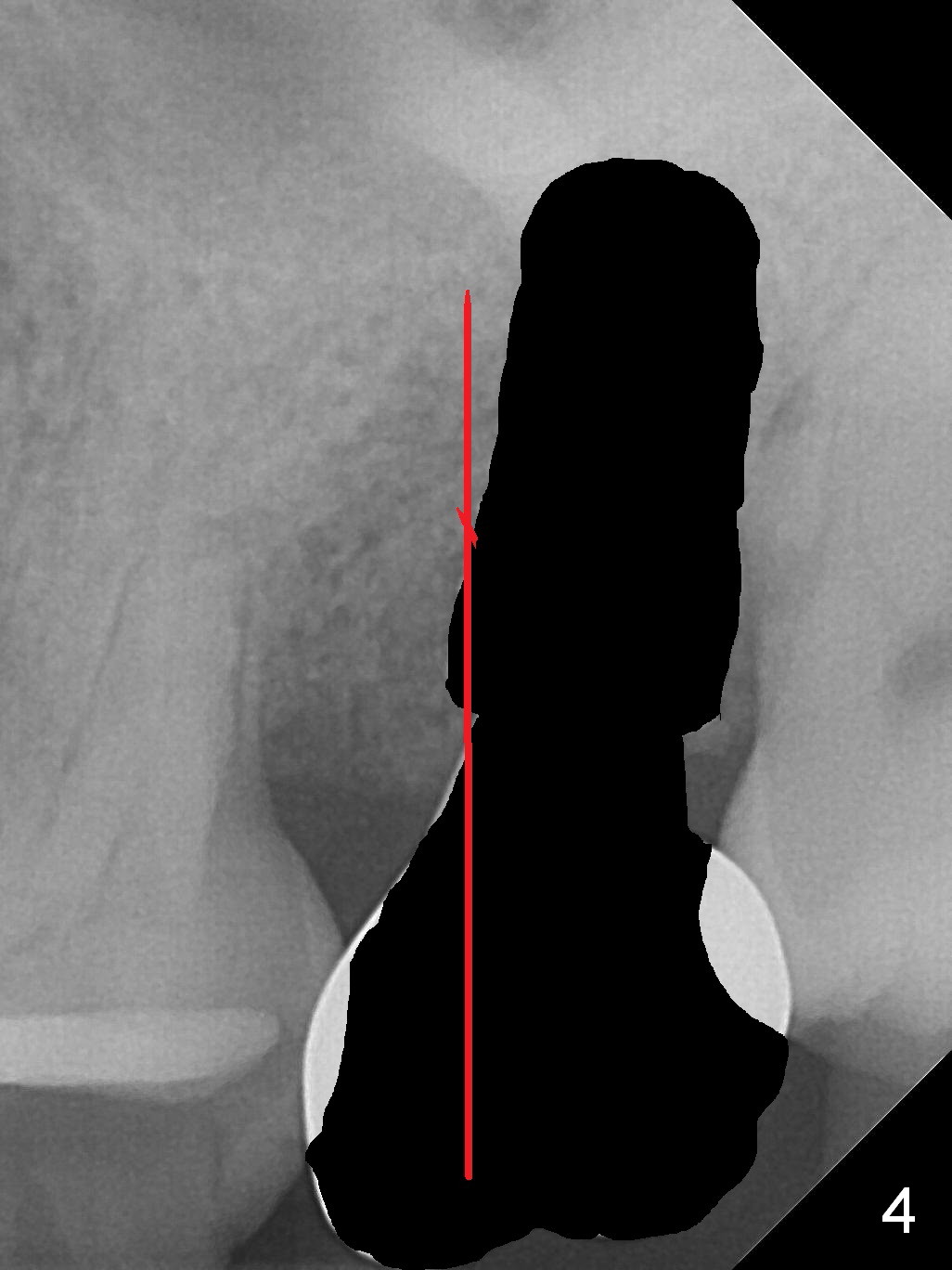
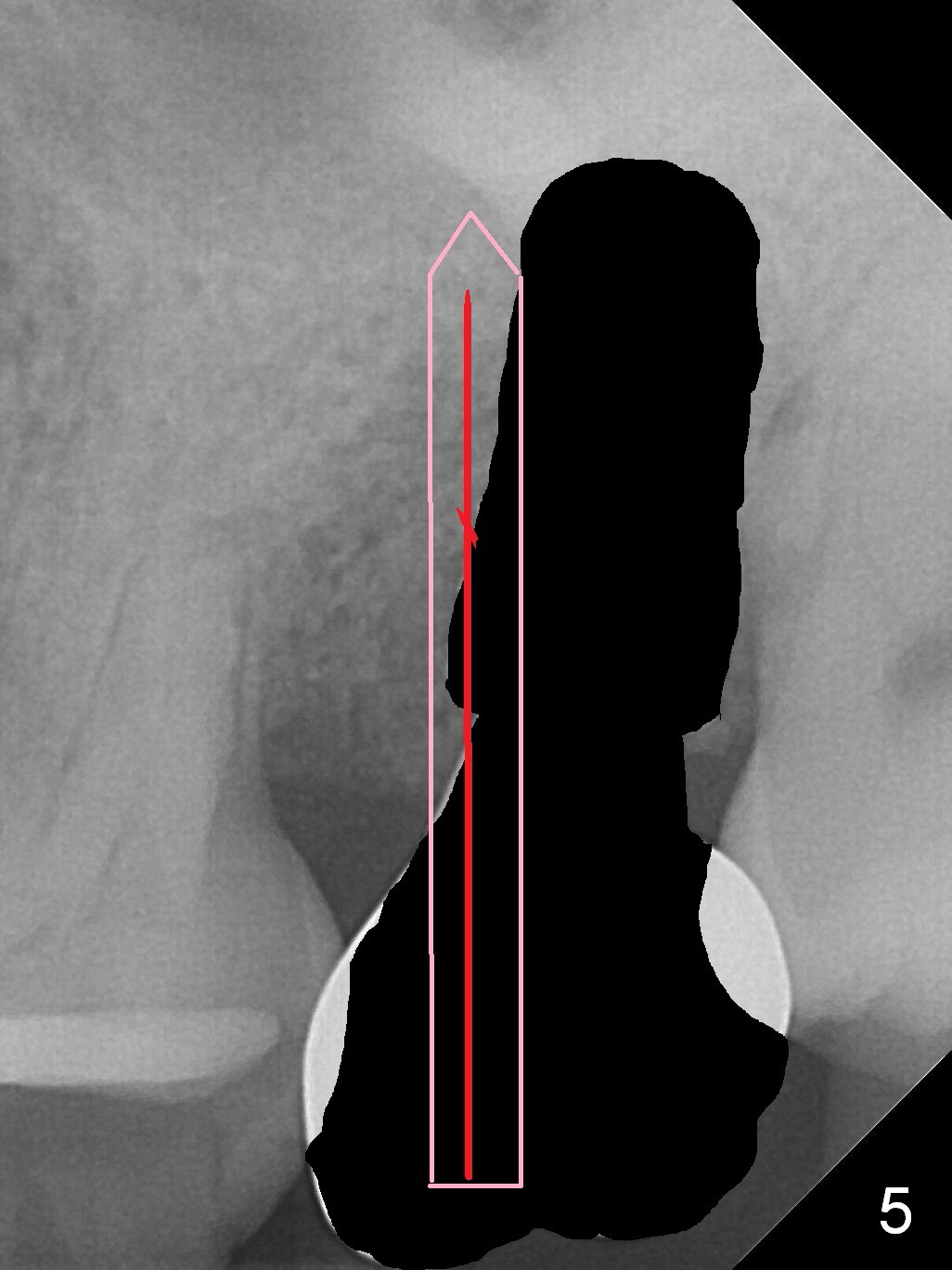
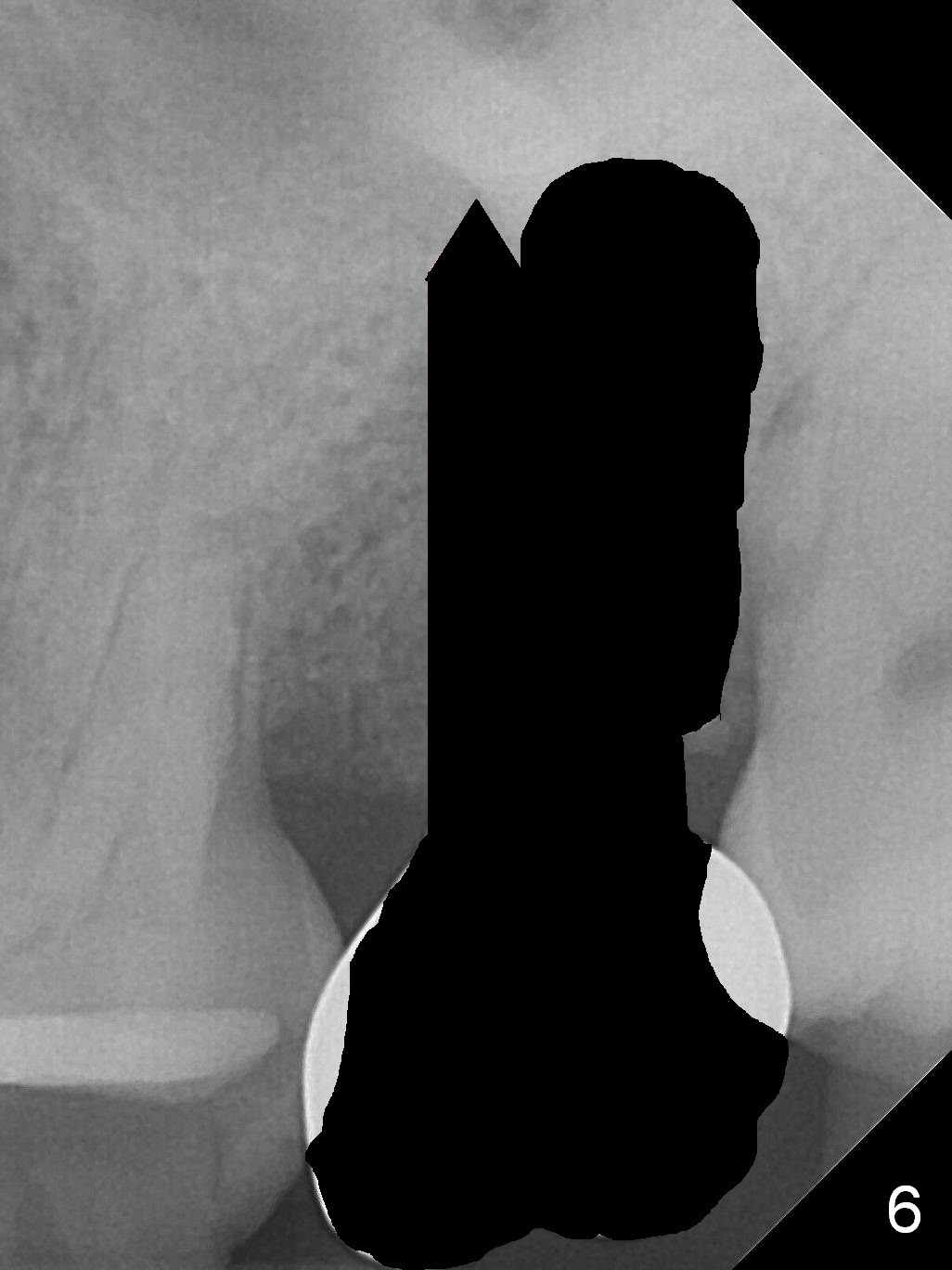
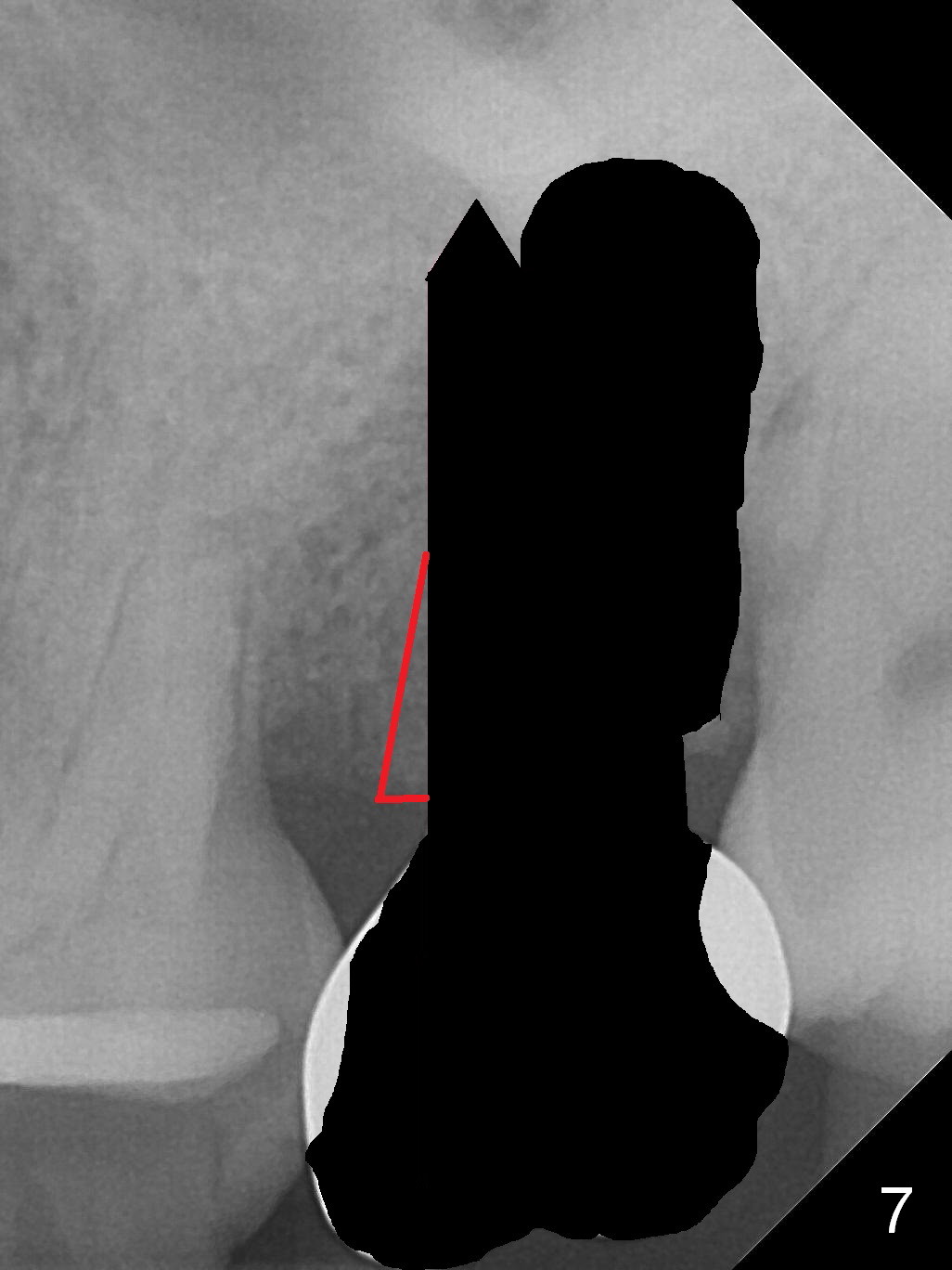
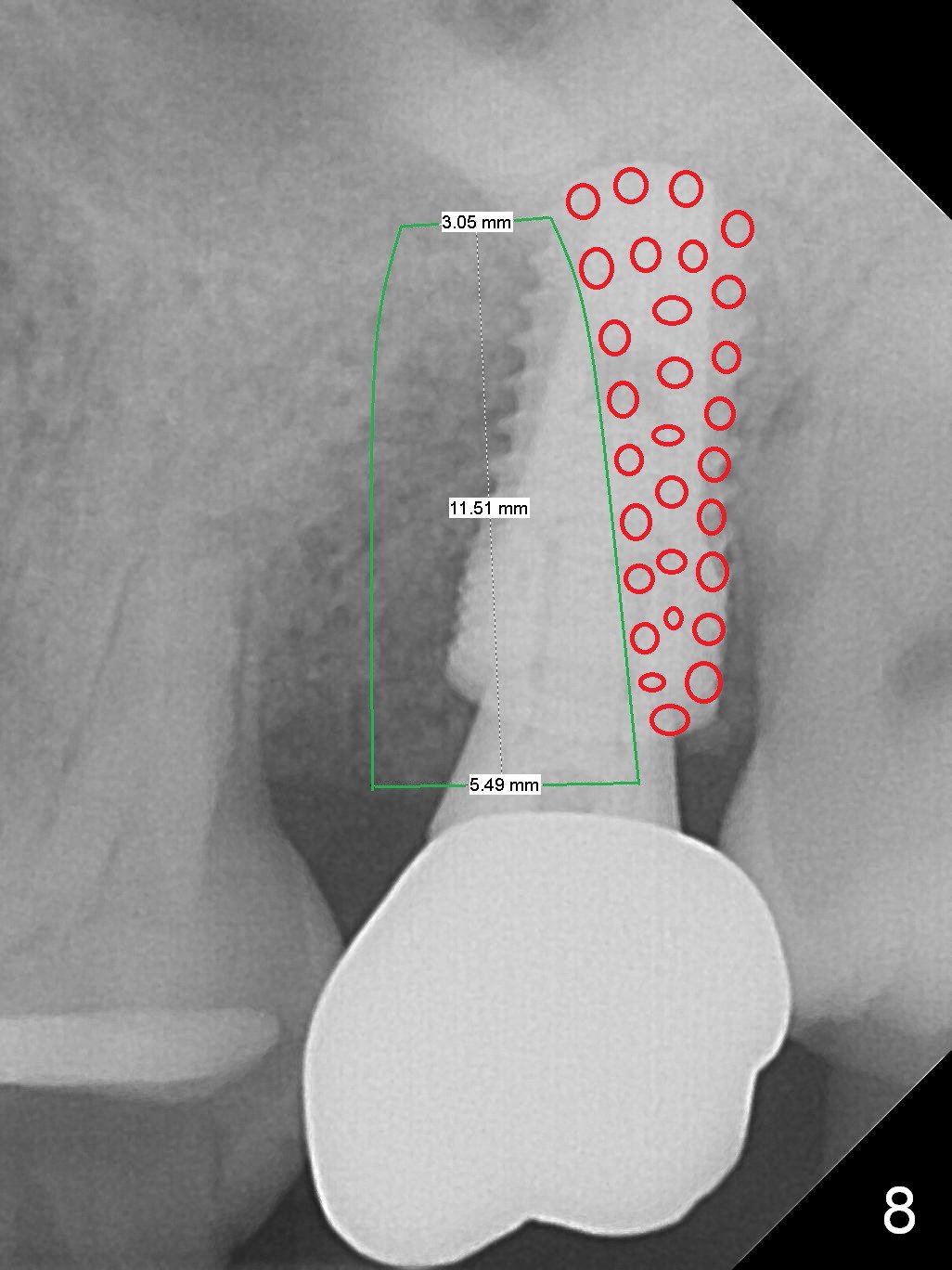
A 43-year-old woman cannot bite hard with the implant at the site of #15. It appears that the bone density around the implant is low (Fig.1 *). The crown seems to be mobile. The crown/abutment/implant appear to be able to be pulled out under local anesthesia. Bone loss is severe preop. In addition, the trajectory of the implant is off (Fig.1 red line). After implant removal (Fig.2), site exploration and Metronidazole soaking, start osteotomy in the mesial wall obliquely (Fig.3 red long arrow). Then change the trajectory (Fig.4). As the osteotomy enlarges, it may shift distally (Fig.5 pink arrow). To prevent excessive distal shifting, withdraw the last drill (Fig.6), remove part of the mesial bone with Lindamann bur (Fig.7 red triangle) and place an implant (Fig.8 green area) with bone graft distally (red circles). The implant may need to penetrate the sinus floor for increased stability. Prepare PRF. Place a healing abutment if insertion torque is low. Otherwise fabricate an immediate provisional to prevent the mesial shift of the 3rd molar.
Return to
Upper
Molar Immediate Implant,
IBS
Xin Wei, DDS, PhD, MS 1st edition 02/04/2017, last revision 12/02/2018