

|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Considerations for Upper 2nd Molar Immediate Implant
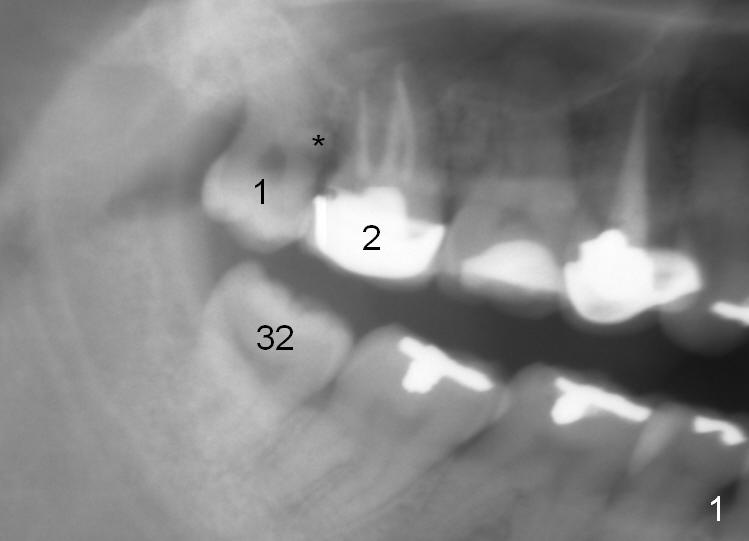
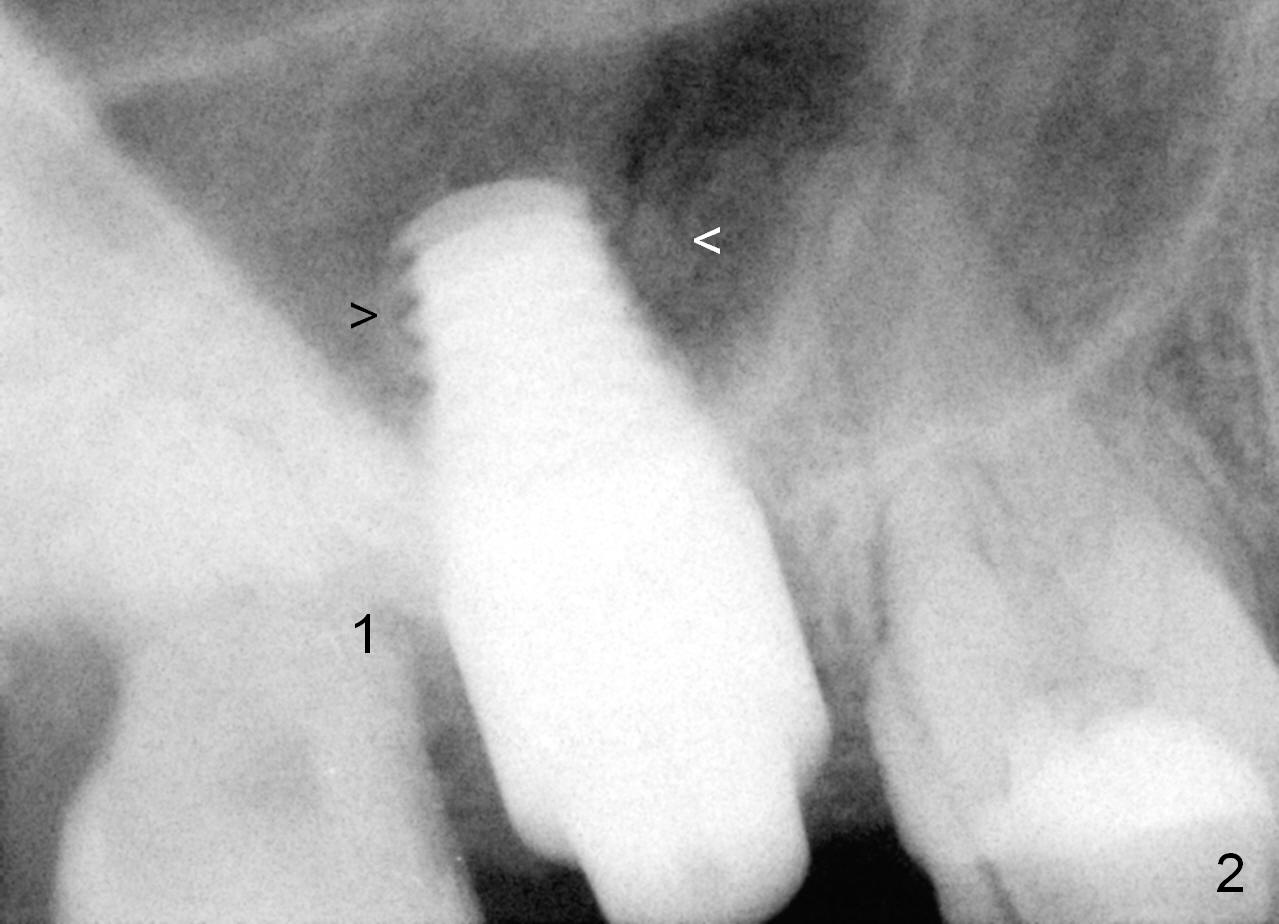
The first consideration: Should the third molar be extracted (Fig.1 (trimmed panoramic X-ray taken prior to #2 fracture): #1). In this case, no, because there is an opposing tooth (#32). More important with the 3rd molar present, the immediate provisional at the site of #2 is more stable. The prominent pathology associated with the tooth #1 is the enamel pearl in the mesial root surface (*), which is removed after #2 extraction (Fig.2: #1).
As planned, a 7x14 mm tissue-level implant is placed in the middle of the socket (mesiodistally (Fig.2) and buccopalatally (not shown) with insertion torque >60 Ncm. What is not ideal is that the implant is placed too deep into the sinus, although the apical portion of the implant is covered by the apparently lifted sinus floor (arrowheads; no graft used for sinus lift). Lack of the control in the depth is mainly due to failure to take intraop PA using #2 sensor. The latter appears to be too clumsy. The smaller, i.e., #1 sensor may be more appropriate. Fig.2 image is trimmed from the original one. From now on, #1 sensor will be routinely used for upper molar immediate implant. This is the 2nd consideration for upper molar immediate implant.
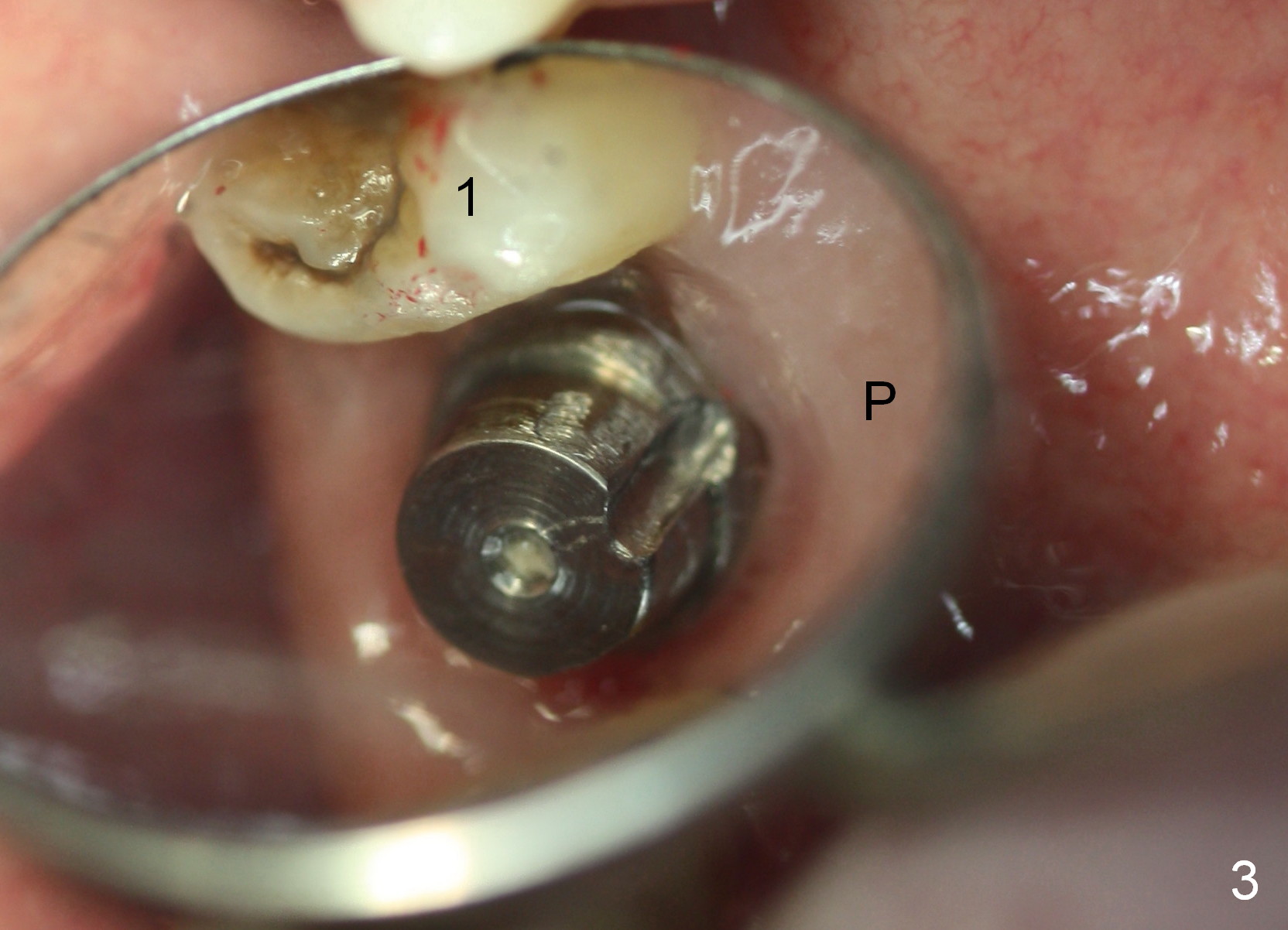
The patient returns asymptomatic 2 weeks postop (Fig.3). The gingiva has approached the implant.
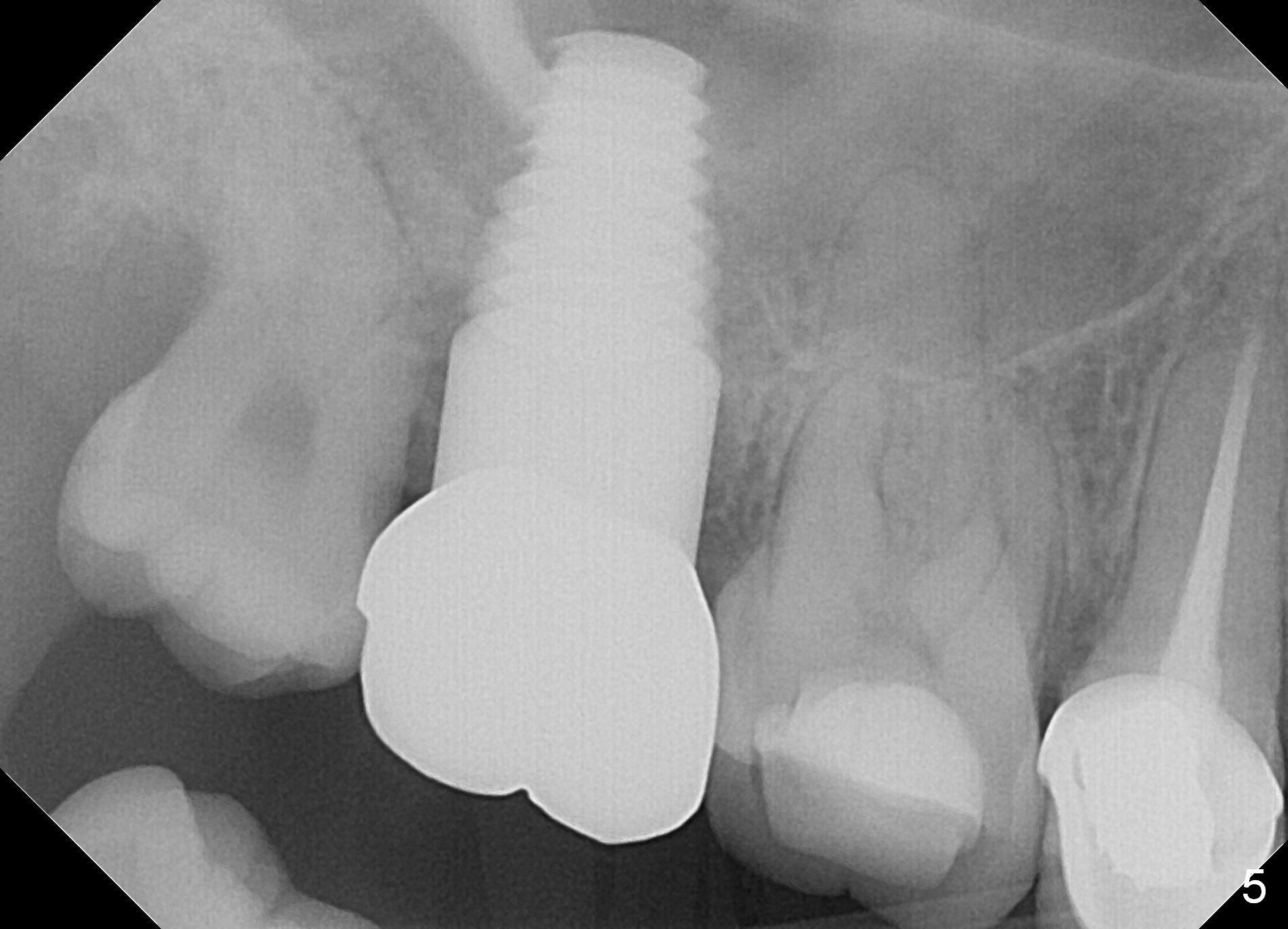
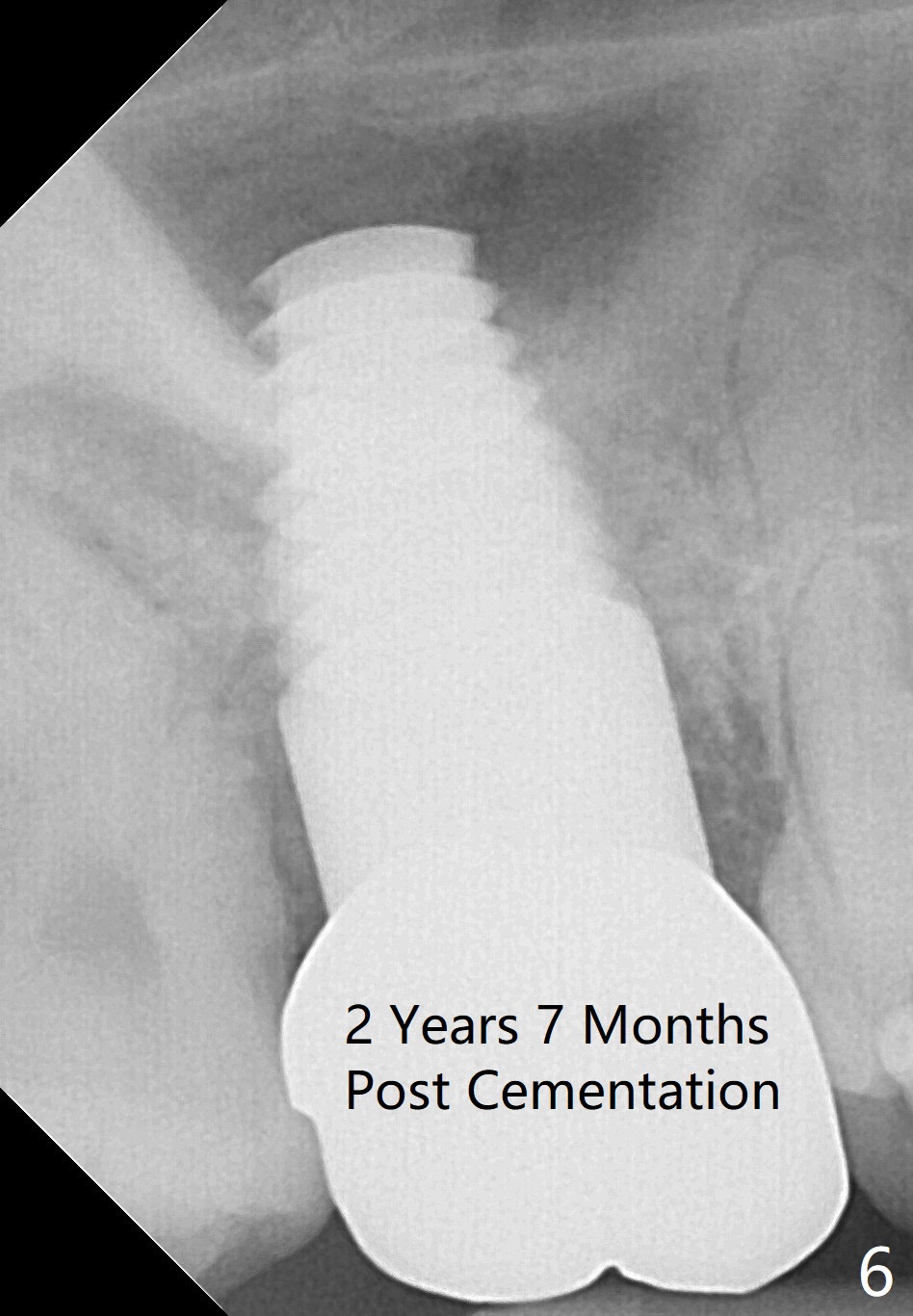
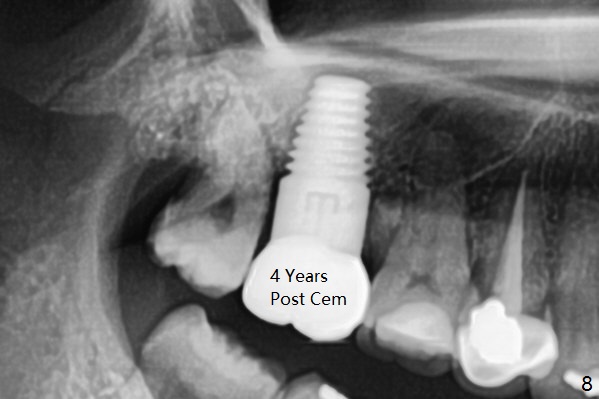
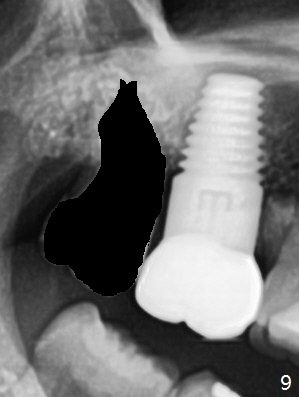
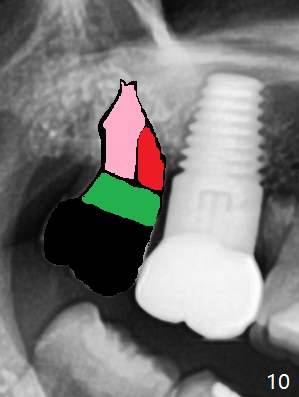
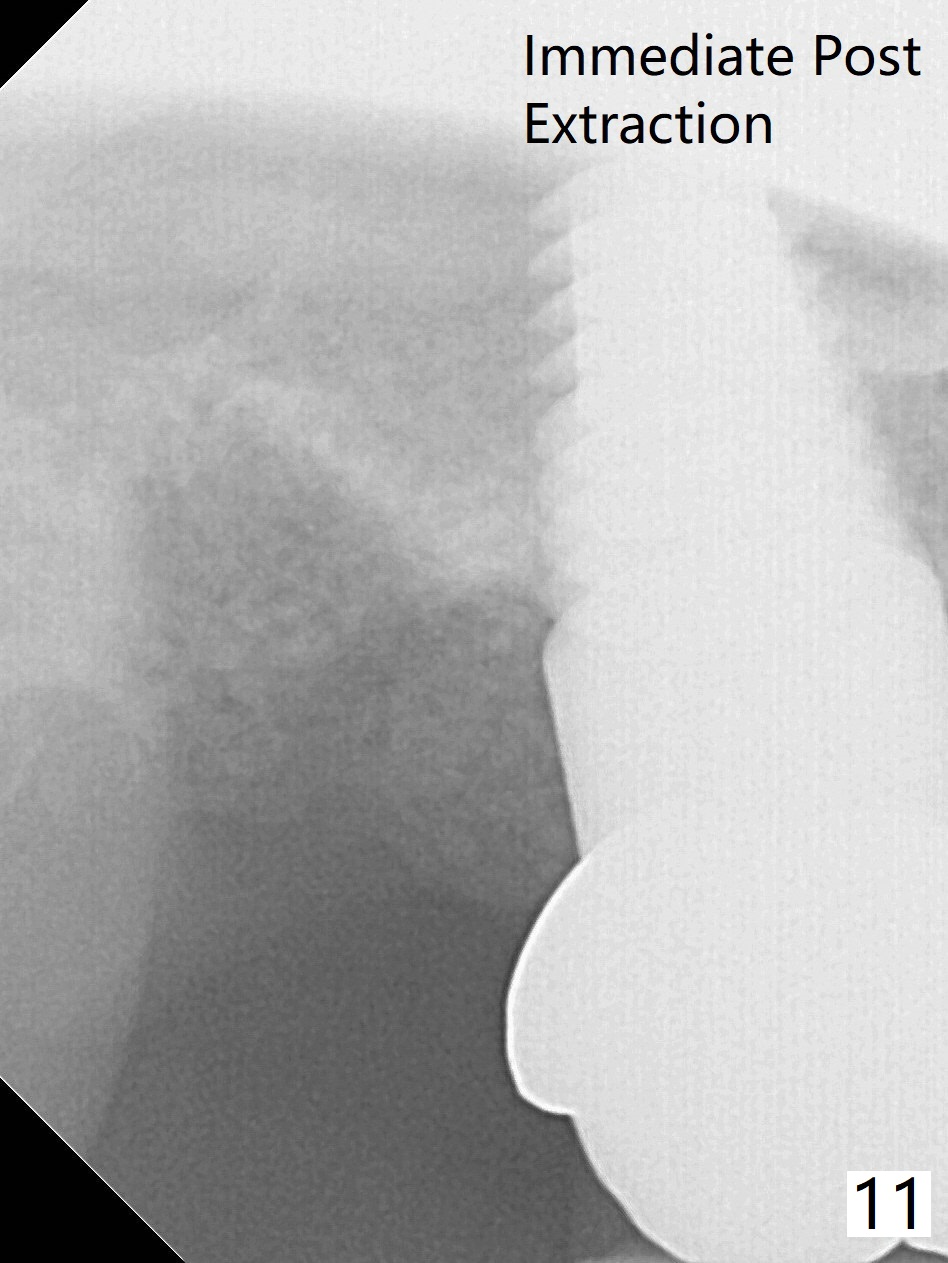
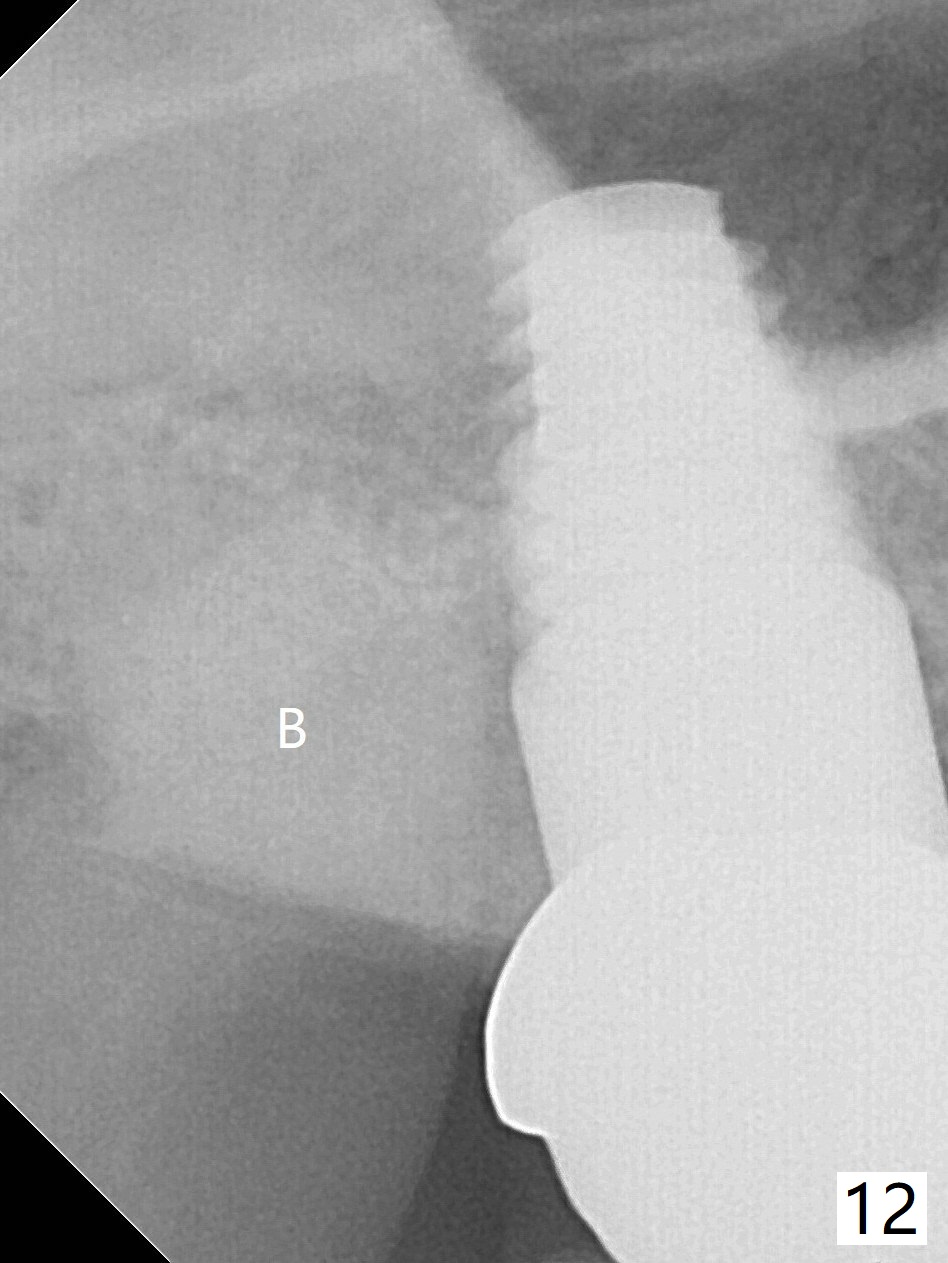
There is no bone loss 3 months postop (Fig.4) or 16 months post cementation (Fig.5). The bone around the implant apparently remains stable between 2 and 4 years post cementation (Fig.6-8). The patient requests extraction of the tooth #1 because of food impaction (Fig.9 black area). To reduce post-extraction bone loss as related to the implant at #2, 3-D Bond (Fig.10 pink (hemostasis)), allograft (red (osteoinduction)) and Osteogen or Collagen Plug + Amnion-Chorion (green) will be used. In fact the extraction socket (Fig.11) is able to hold .5 cc 3-D Bond (Fig.12), leaving no space for allograft. Amnion-Chorion membrane and 6-month membrane are sutured in place with 4-0 PGA, followed by periodontal dressing. Amoxicillin is prescribed. Periodontal dressing dislodges 4 days postop. The distal socket closes, while the mesial portion has opening with sutures in place. The 6-month membrane is invisible. In brief, Amnion-Chorion membrane helps wound heal.
Return to
Upper Molar Immediate Implant
Plug
Trajectory II
Augma
Xin Wei, DDS, PhD, MS 1st edition 05/01/2015, last revision 04/14/2020