


|
|
|
|
|
||
|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|||||
Size of Immediate Implant in One Socket of Upper Molar
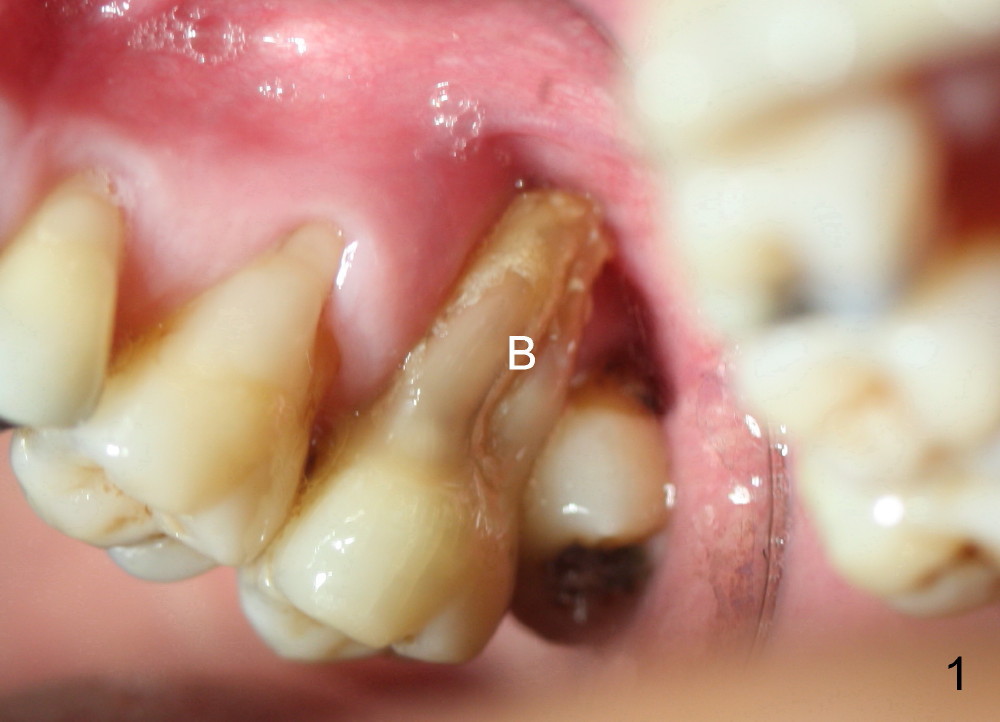
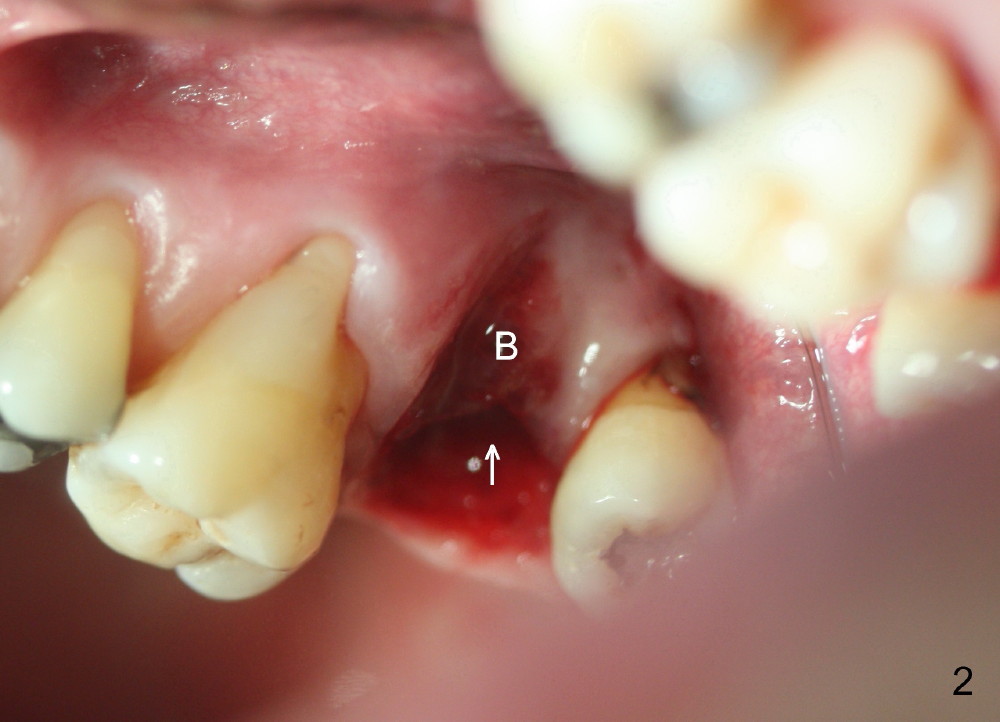
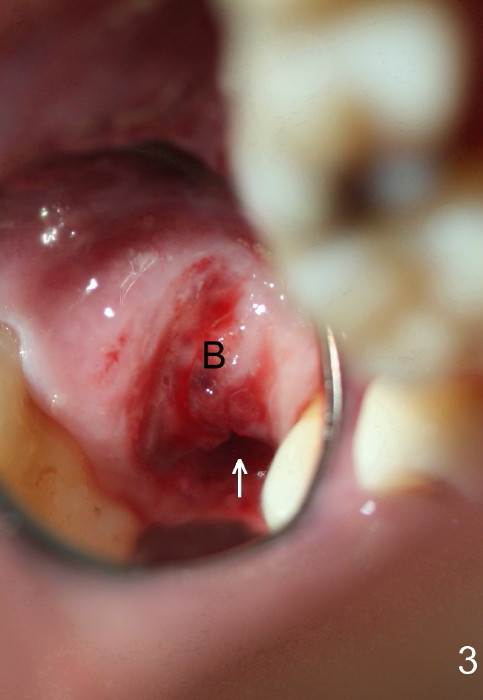
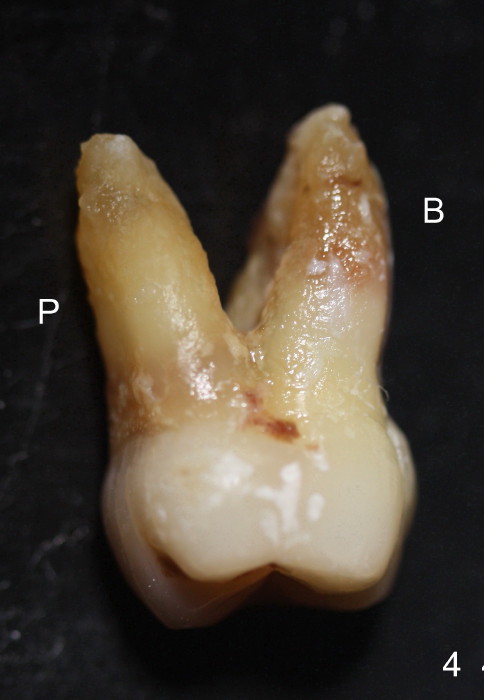
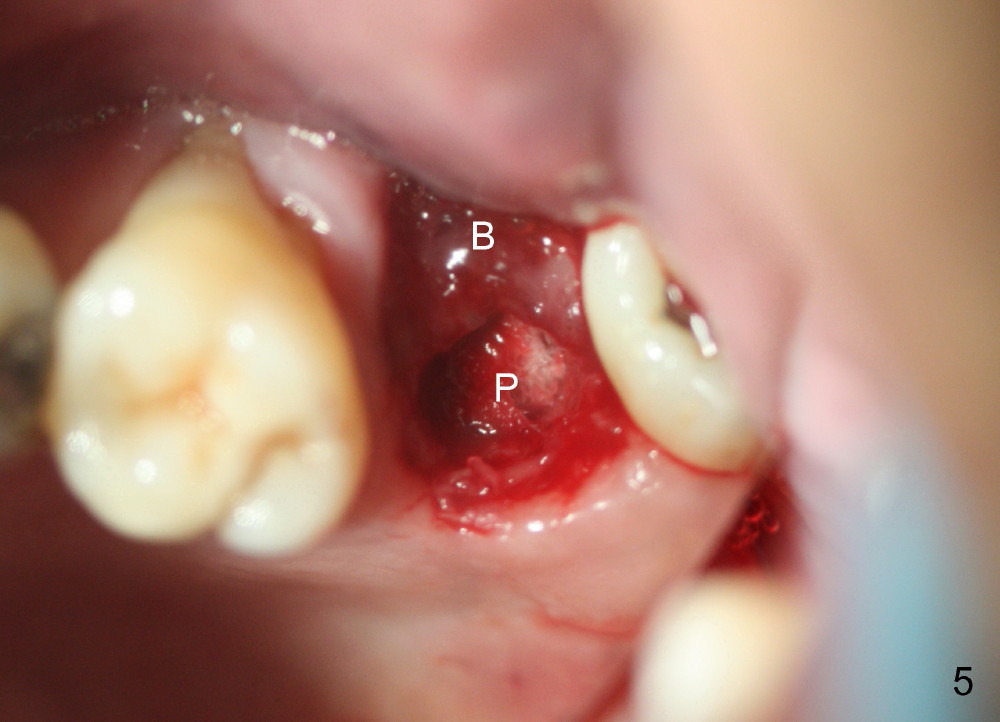
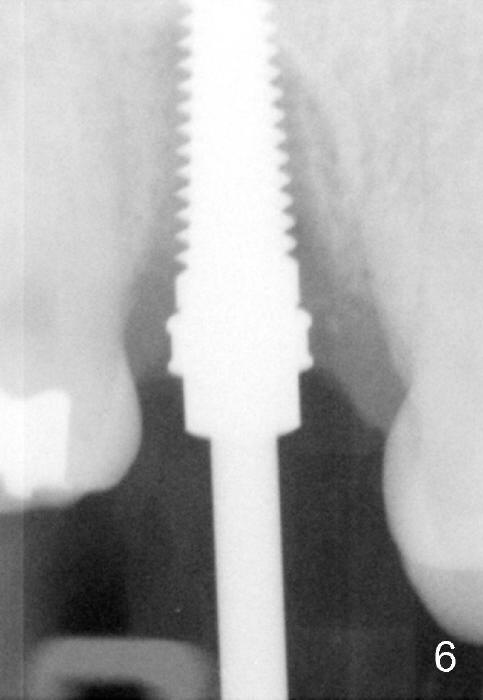
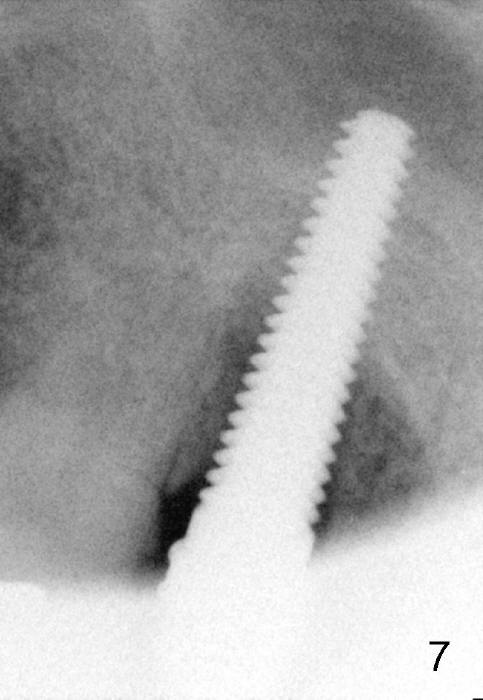
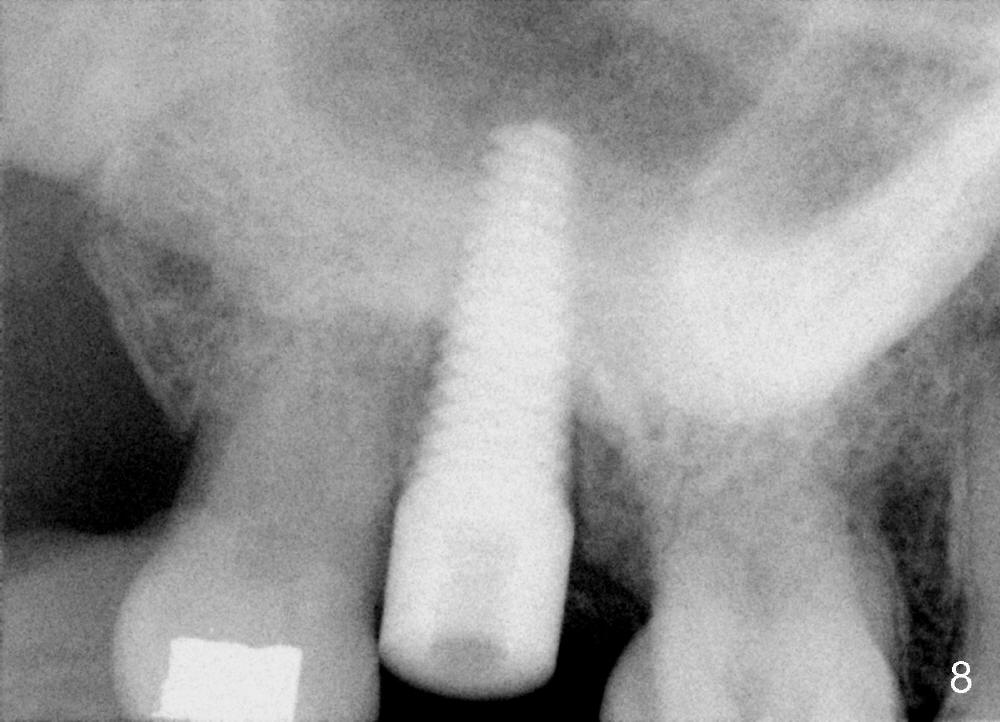
The buccal roots of the 2nd upper molar are basically entirely exposed (Fig.1 (mirror view) B). When the tooth is extracted, there is no bony buccal (B) socket (Fig.2,3,5). Although the furca of the extracted tooth is fairly large (Fig.4), the septum is mainly of soft tissue. Therefore the palatal (Fig.2,3 arrow, Fig.5 P) socket can be the implant site. The palatal socket is long and narrow. Intraop plan is to place a long, relatively narrow implant. Pointed end osteotomes are being used to form initial osteotomy in the apical palatal wall of the palatal socket 17 mm deep (from gingival margin; Fig.16,17). There is no sinus membrane perforation. The bone density is high. The osteotomy is deepened to 20 mm and enlarged by drilling and reaming. A 4.5x20 mm tap achieves initial stability (Fig.6,7): although the apex of the tap looks as if it is the sinus, clinically the base of osteotomy is solid. The osteotomy is further enlarged by larger taps with increasing stability. By the time a 6x20 mm implant is placed, the insertion torque is 60 Ncm (Fig.8). The peri-implant gap is limited; small amount of allograft and Osteogen is inserted. An abutment is placed, followed by an immediate provisional. The purpose of the latter is to cover the wound and to prevent shifting and supraerupting of the neighboring and opposing teeth during osteointegration.
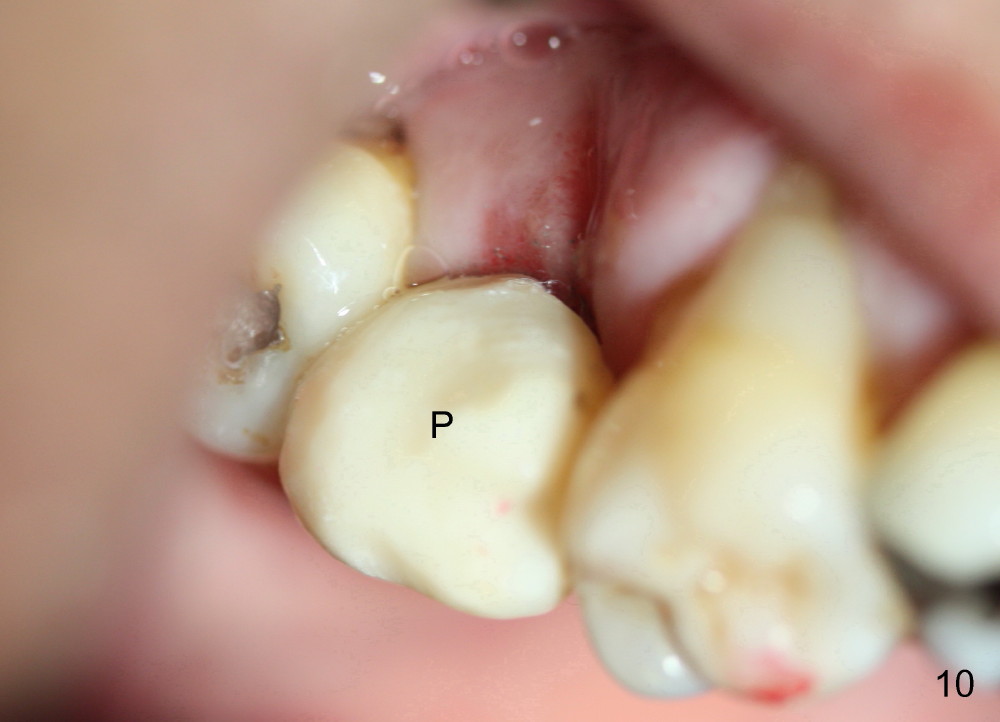
The provisional dislodges 4 days postop (Fig.9). After re-prepping the implant (I) and abutment (A in Fig.9) for increased retention, the provisional (P in Fig.10) is relined and recemented with tight contact with the neighboring teeth so that the latter are not going to shift in 2-4 months of osteointegration of the implant.
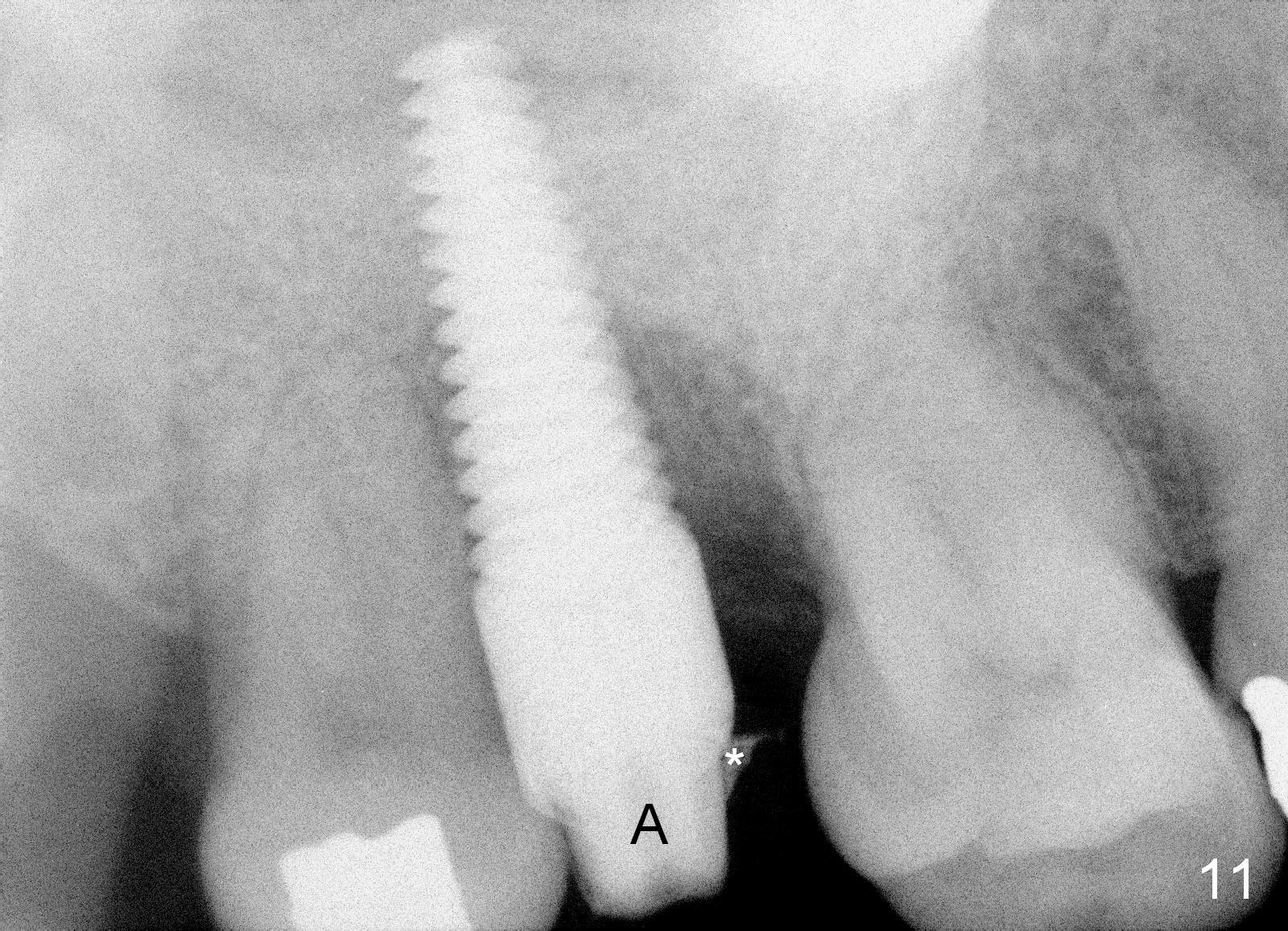
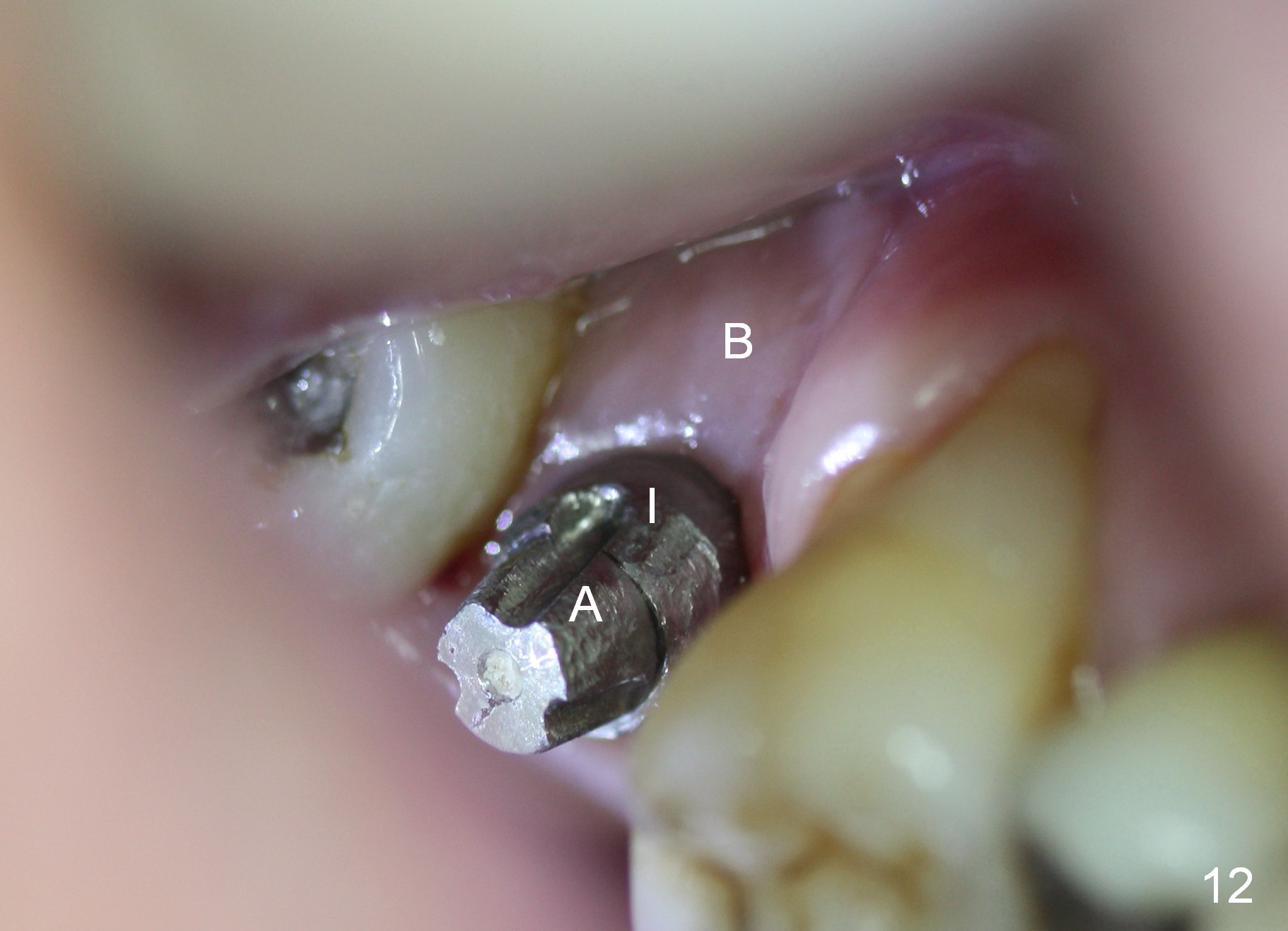
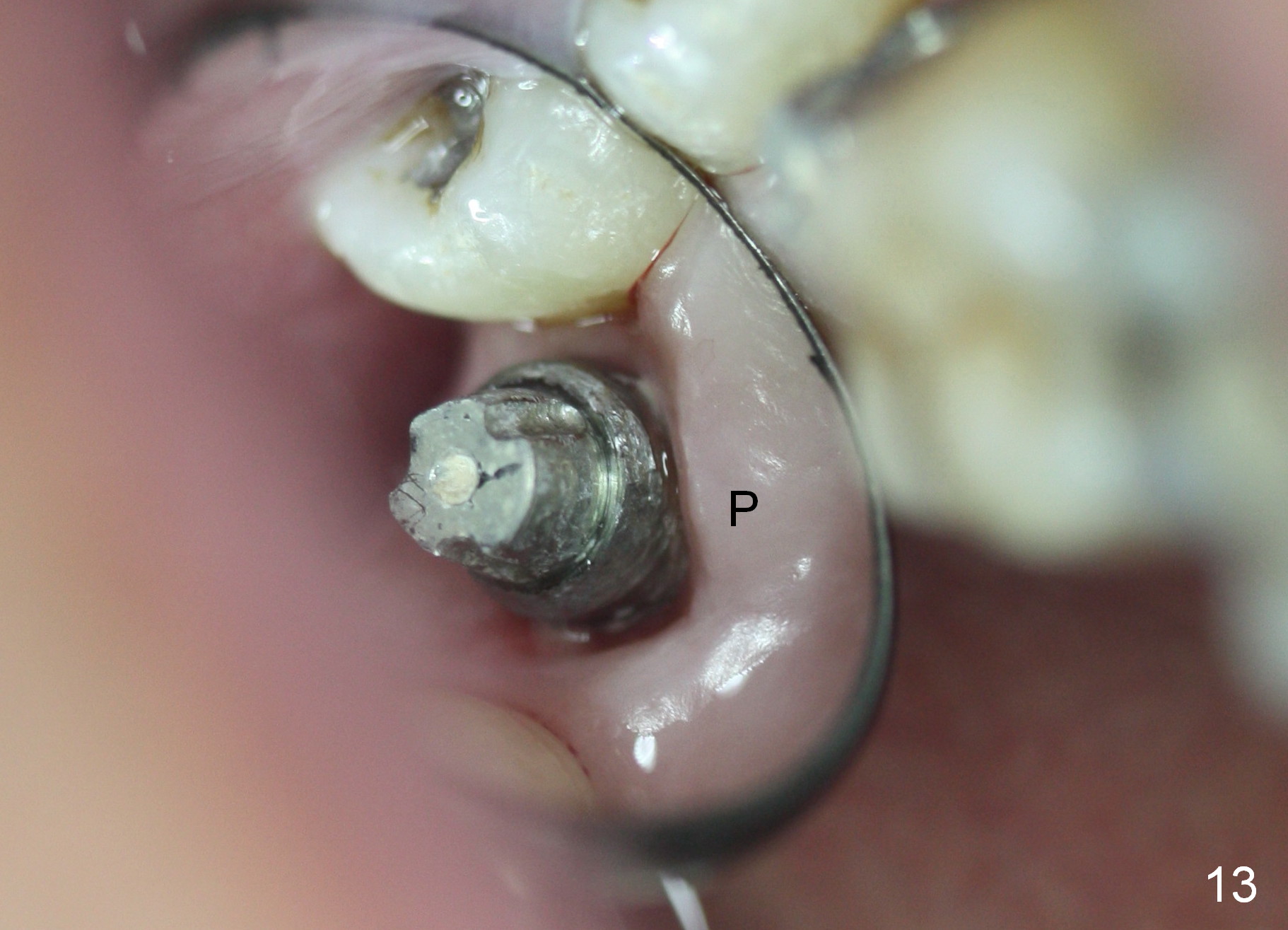
The patient returns 3.5 months postop (Fig.11-13), requesting final restoration, because of loose provisional. The implant is stable with healthy buccal (B) and palatal (P) gingiva.
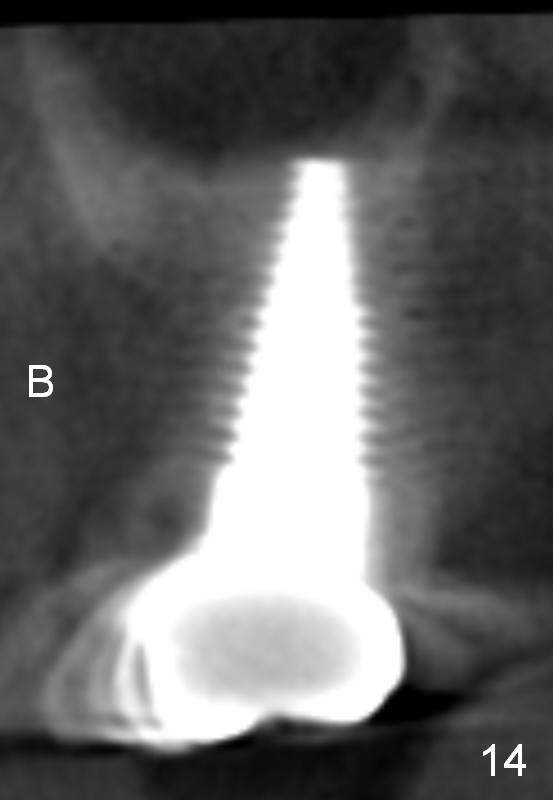
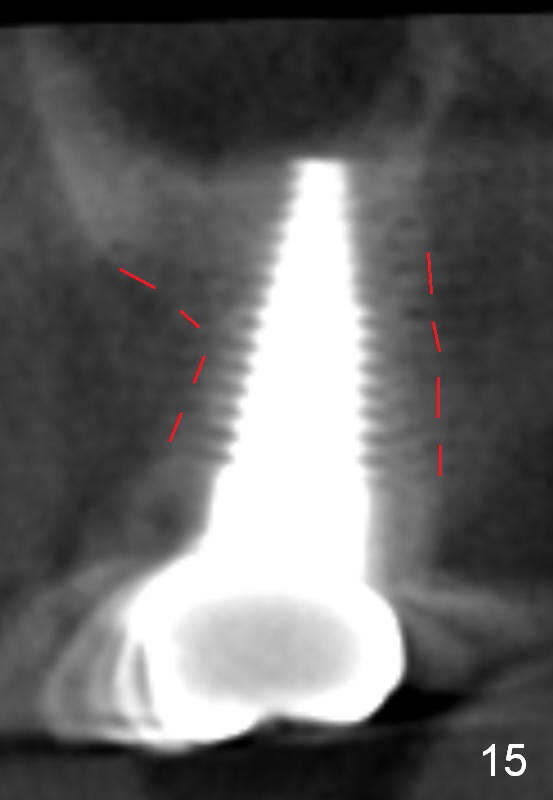
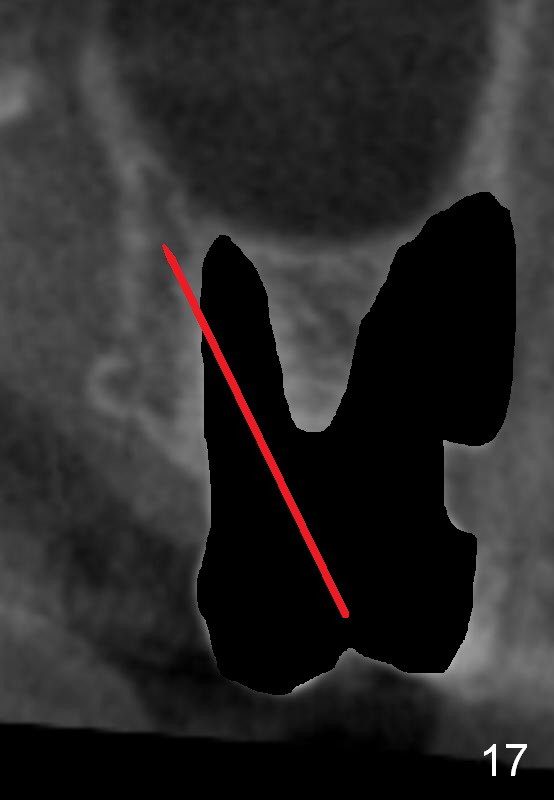
To place an implant in the anterior atrophic ridge, CBCT is taken (4 months post cementation of the crown at the site of #2). The implant is found inside the alveolar ridge (Fig.14,15). Fig.16 shows the cross section of the tooth #15 (*: buccal plate). Fig.17 demonstrates the socket after extraction with loss of the buccal plate. To place an implant, osteotomy is initiated in the apical palatal wall of the palatal socket (red line, as mentioned above).
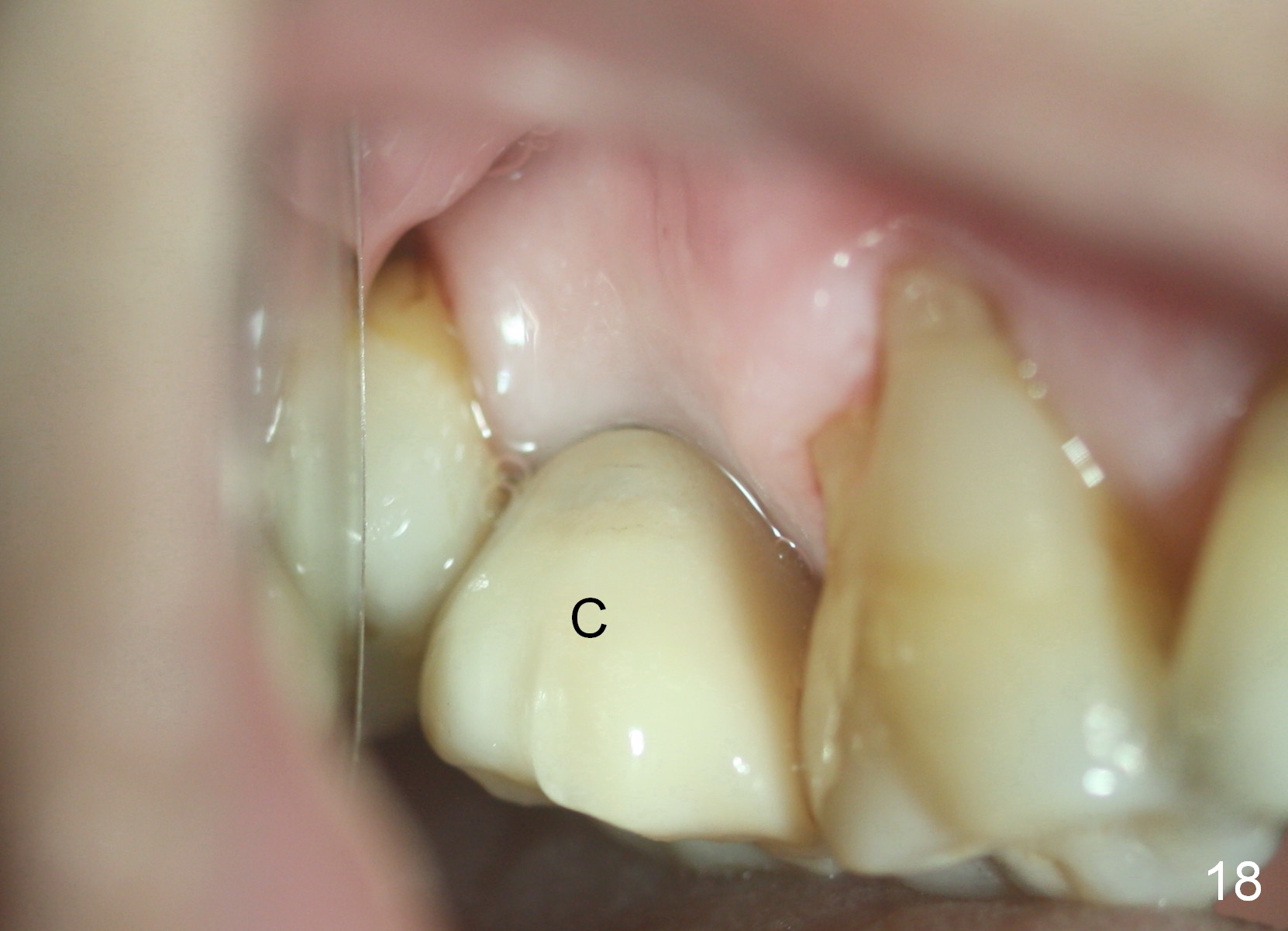
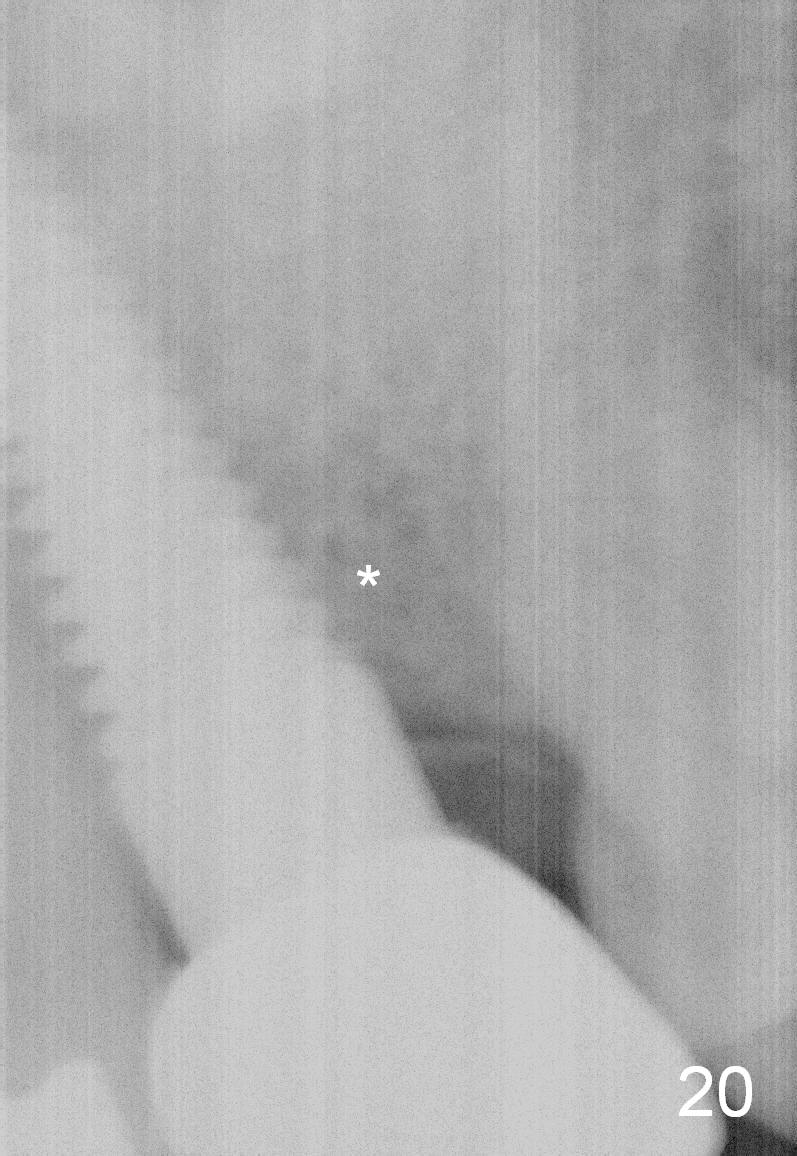
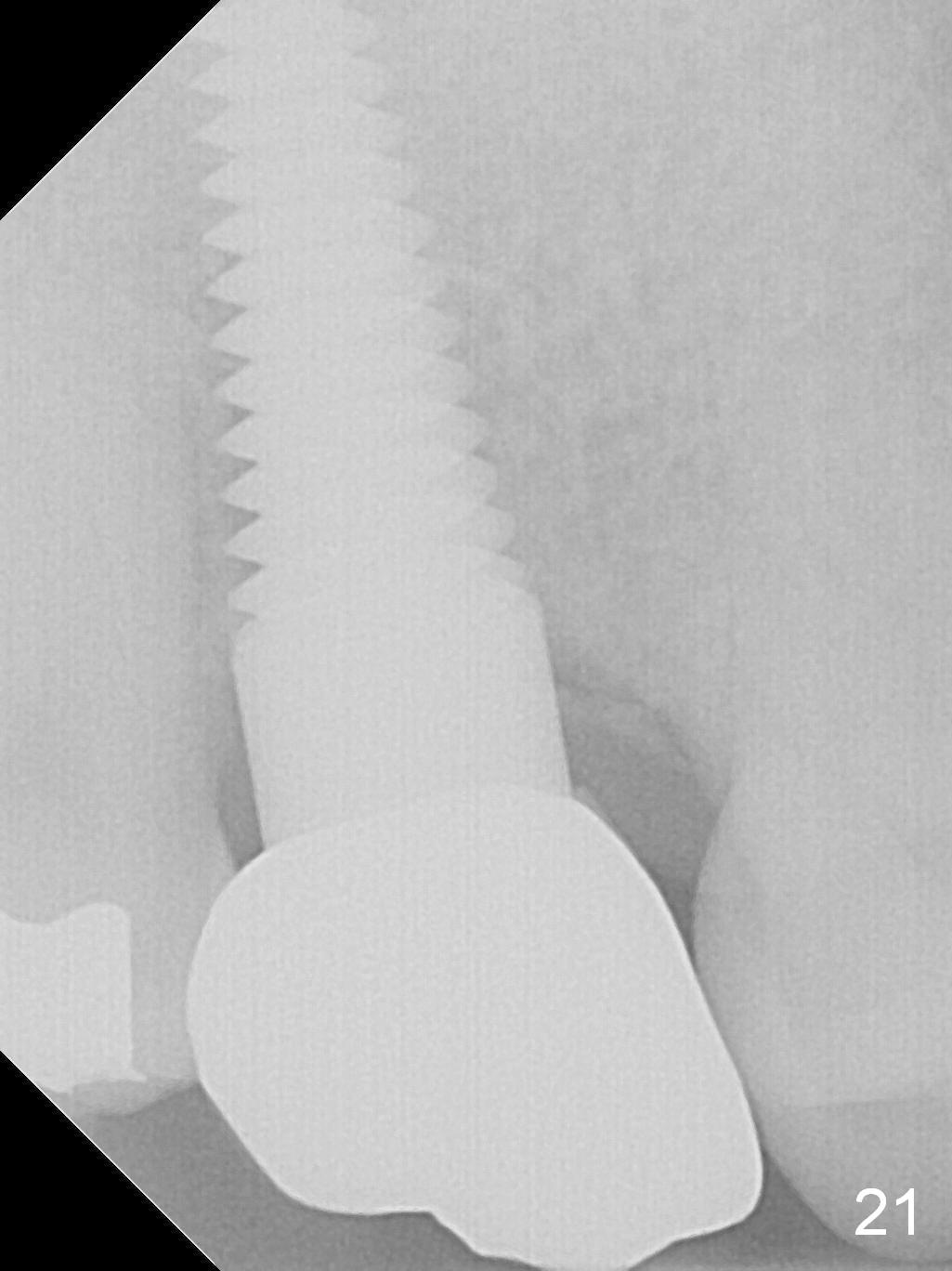
The gingiva remains healthy around the implant crown (Fig.18 C) and there is no mesial defect 14 months (Fig.19,20 *, as compared to Fig.8,11) or 32 months (Fig.21) post cementation.
Return to
Upper Molar Immediate Implant,
Posterior Immediate Provisional
Buccal Root Exposure
9
Webinars
上
下
第二磨牙即种
Xin Wei, DDS, PhD, MS 1st edition 12/31/2014, last revision 04/18/2021