
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Anatomic Basis for Upper 2nd Molar Immediate Implant
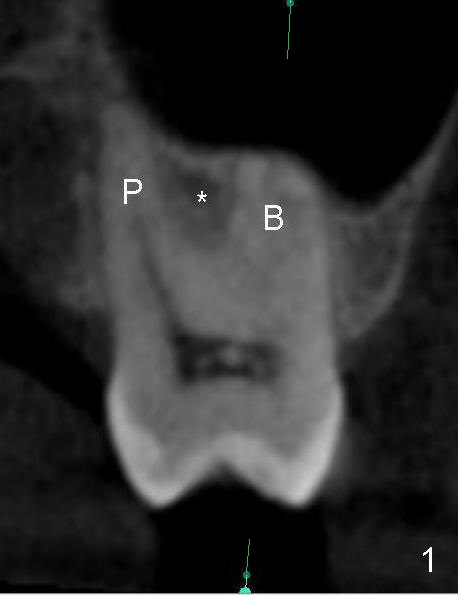
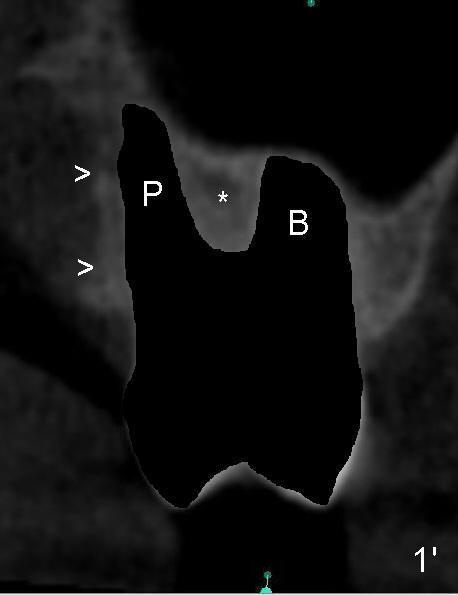
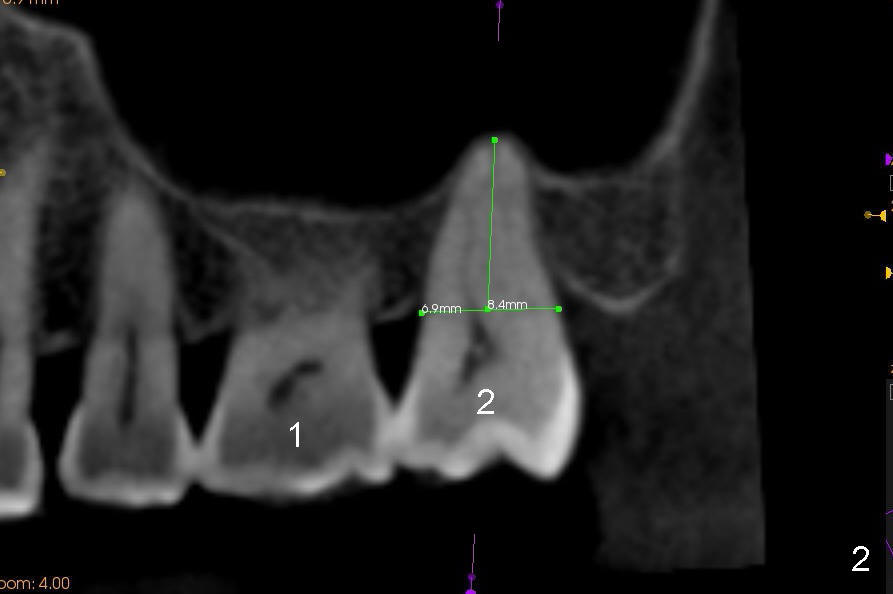
The upper 2nd molar have 3 roots with limited furcation. The buccal ones may be fused (Fig.1 (CT coronal section),2 (sagittal)). After extraction, there are 2 sockets (Fig.1'). When 3 roots are fused, there is a single large socket.
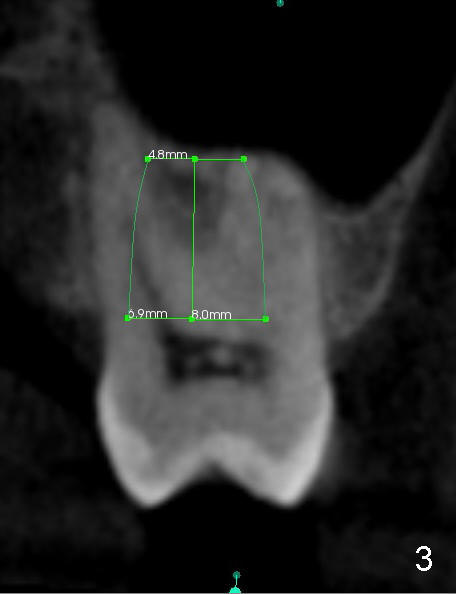
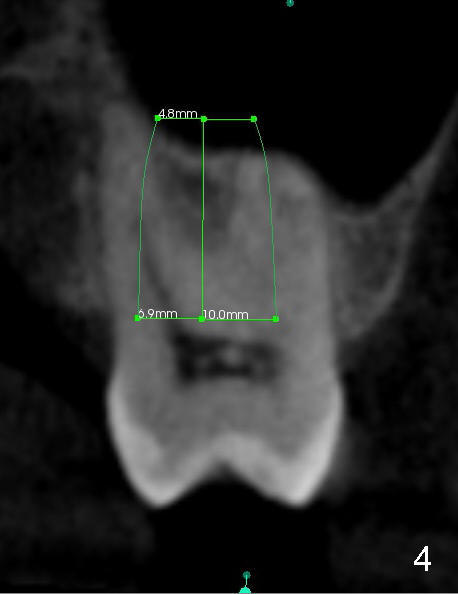
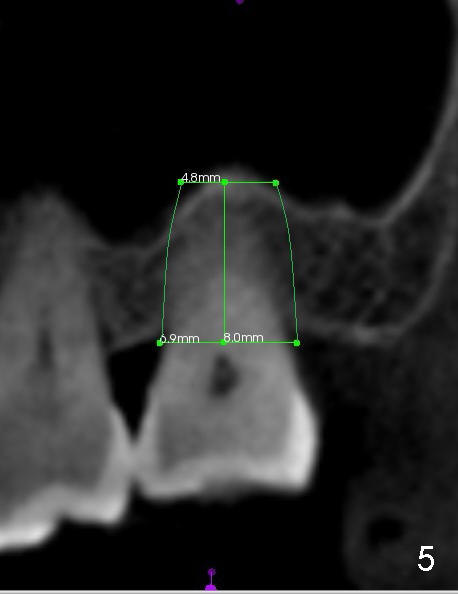
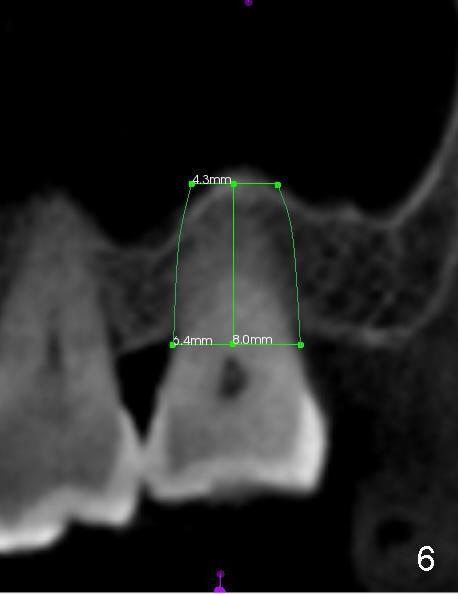
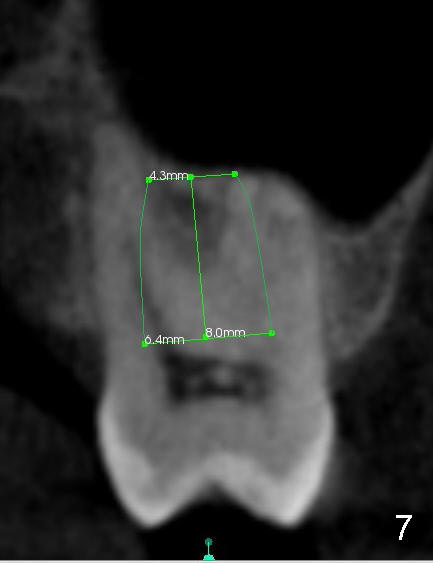
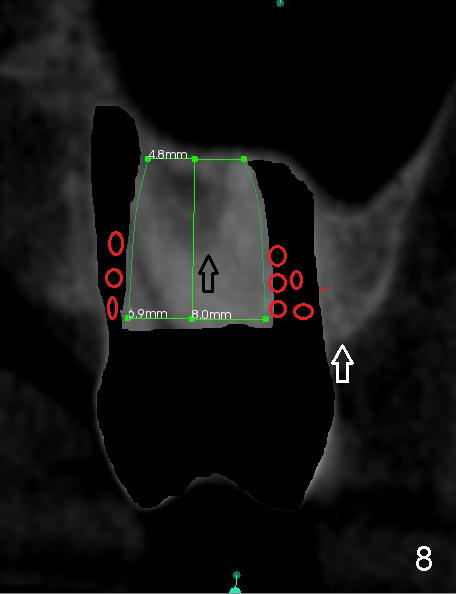
When the buccal roots are fused, there are 3 potential sites for immediate implant (Fig.1'): septum (*), buccal (B) and palatal (P) sockets. Septal placement (6.9x8 mm bone level implant) is the most ideal for restoration (Fig.3). The length of the implant can be increased (10 mm) with sinus lift so that the base of the implant between the buccal and palatal apices in height (Fig.4). Primary stability is derived mainly from the implant body engagement into the septum (Fig.5 coronal section through the septum). If bone density in the septum is high, a small implant may be appropriate (Fig.6,7: 6.4x8 mm). The large implant (6.9 mm) is chosen so that amount of bone graft to be used (Fig.8 red circles) is less.
The 2nd best site for implantation in this case is the buccal socket, which is large with thicker buccal bone (Fig.9). Although the apex of the implant is buccal, the base of it can be leaned palatal using bone manipulation.
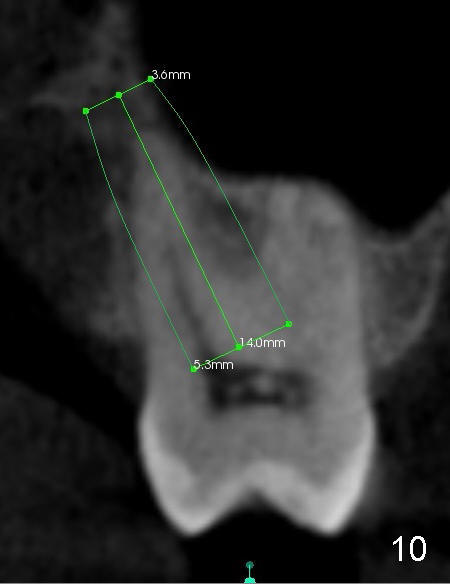
The least ideal implant site is the palatal socket; a longer and smaller implant (Fig.10: 5.3x14), in case of buccal bone defect. The coronal end of the implant should be placed as central as possible.
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/28/2014, last revision 12/28/2014