





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Socket Preservation or Implant Placement?
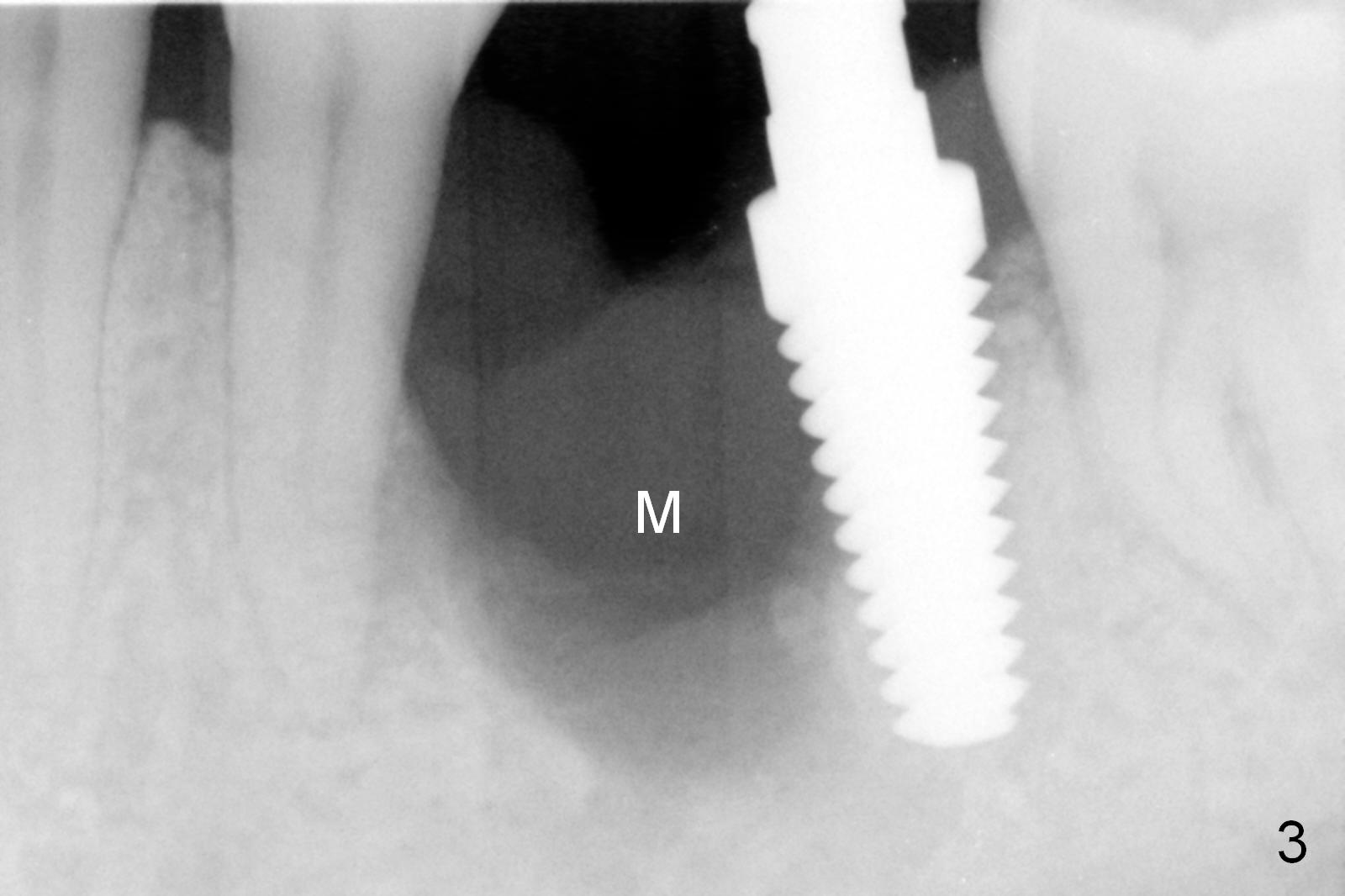
Considering the severe bone loss in the meisal socket, socket preservation is indicated if immediate implant is not feasible. Preop exam shows that the mesiobuccal gingival recession (Fig.1 MB) is not as severe as the mesiolingual one (Fig.2 ML). Because of oozing from the mesial socket, buccal envelop incision is made with flap raising to increase visibility. Probably due to periodontal infection, pain control is difficult. Osteotomy buccal to the Inferior Alveolar Canal proves to be risky. In addition, osteotomy in the mesial socket is more difficult than the distal one (Fig.3). Once the osteotomy depth is determined relative to the superior border of the Inferior Alveolar Canal (4 mm), the osteotomy depth increases by 2 mm. A 5.5x10 mm implant is placed with insertion torque ~ 35 Ncm (Fig.4); a 15 ° angled abutment (5.5 mm in diameter, 4 mm in cuff) is placed mesially. Then the abutment is turned lingually favorable for restoration (Fig.5), the remaining socket is filled with allograft/Osteogen (*) and Collagen Plug.
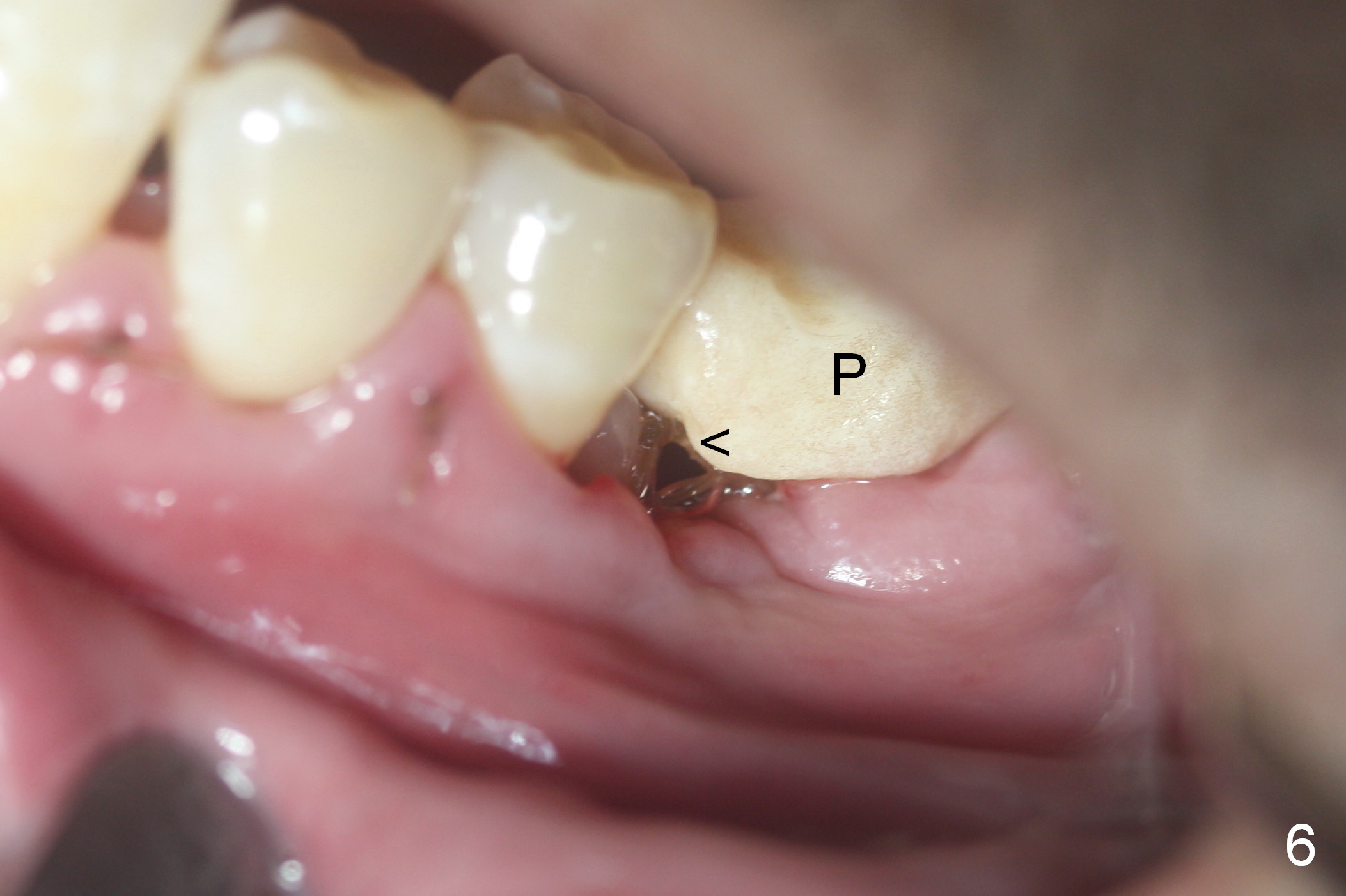
The patient is doing well postop. The mesial socket appears to have collapsed 7 days postop (Fig.6 <). The mesial portion of the immediate provisional (P) should have been overbuilt to compensate for the socket with lost buccal and lingual plates.
The patient reports loss of the provisional and looseness of the "implant" 4 weeks postop, while he is traveling in China. The looseness is most likely derived from detachment of the angled abutment from the implant.
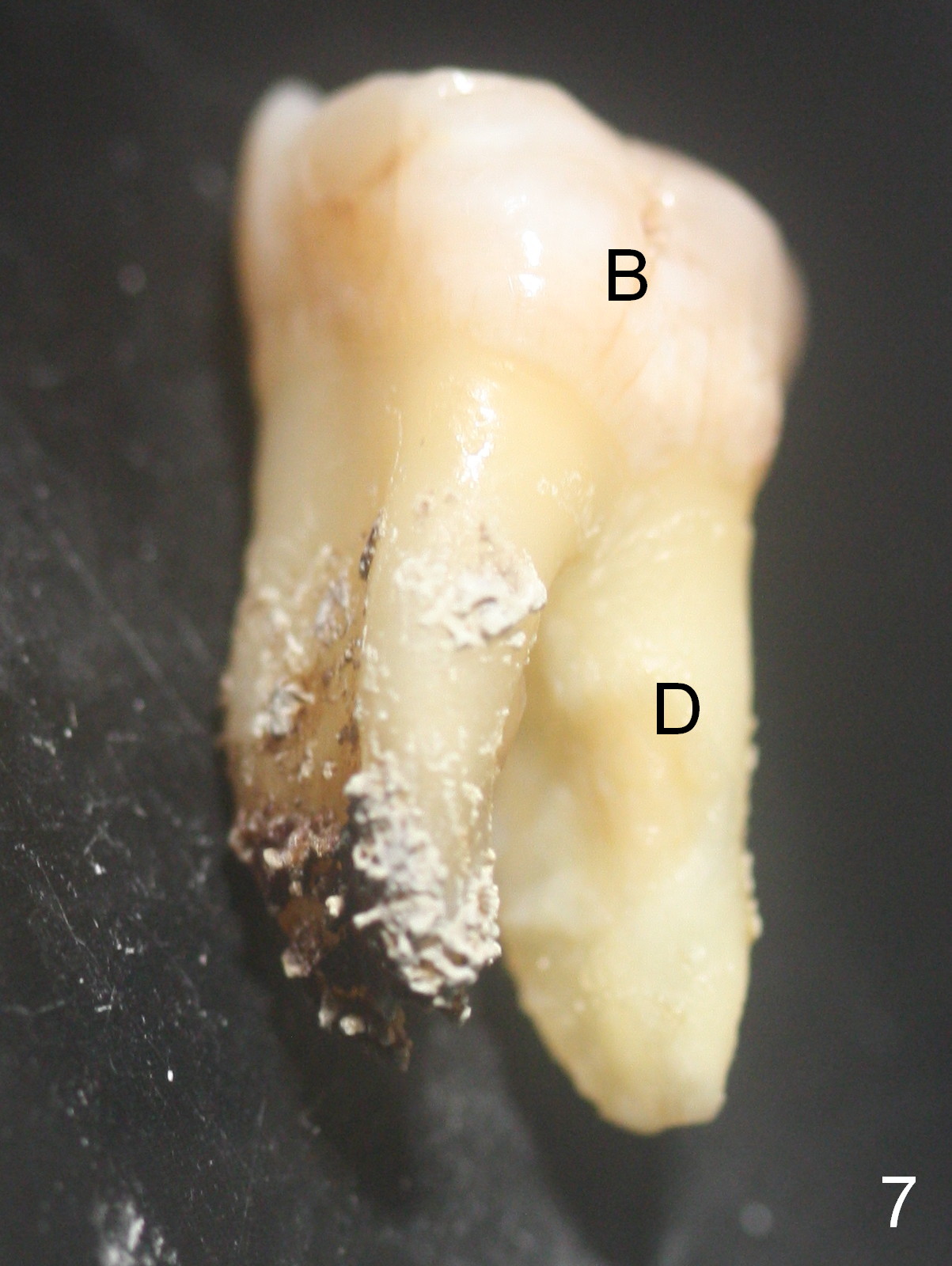
There is calculus over the mesial root of the extracted tooth (Fig.7,8).
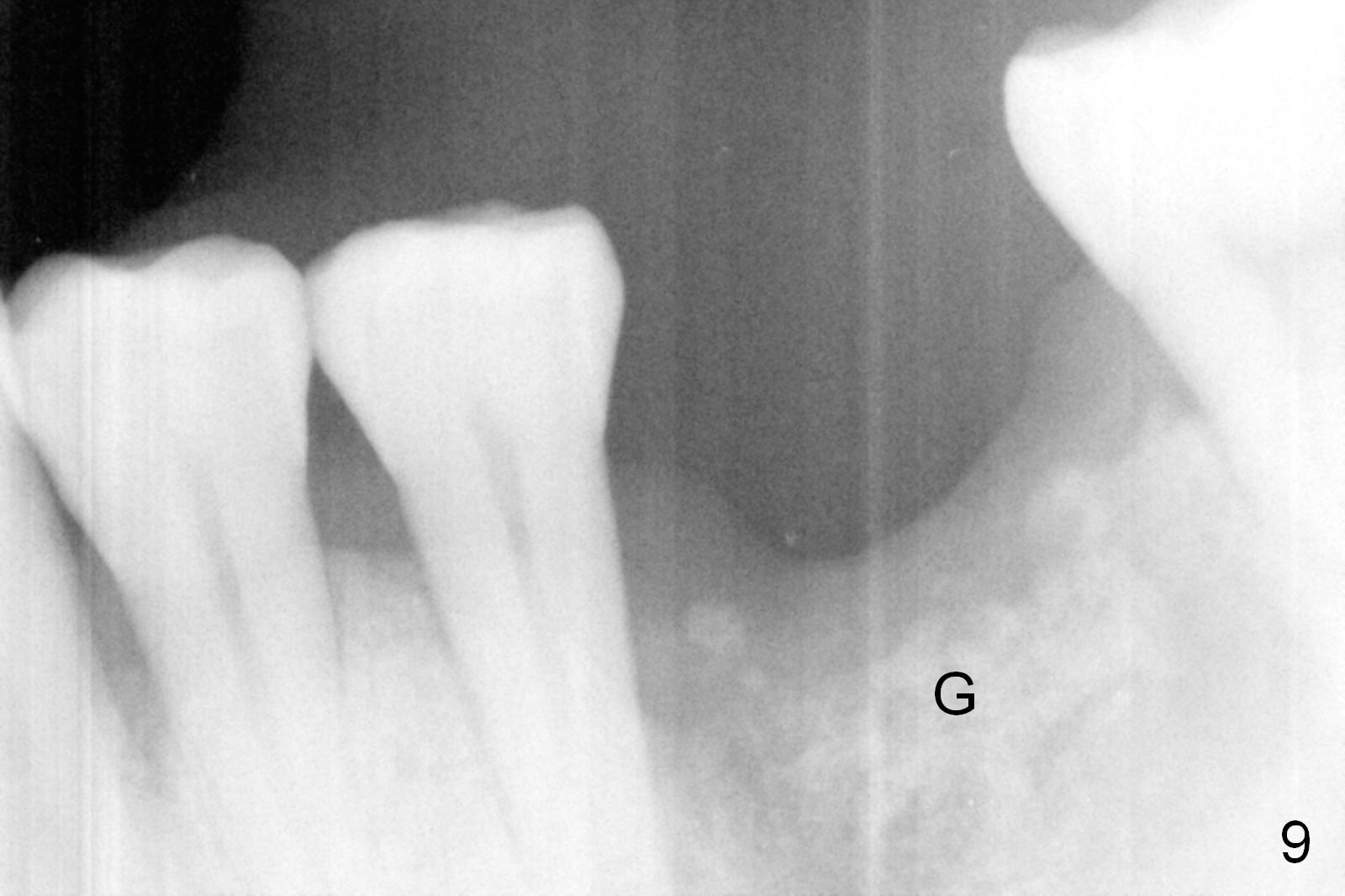
When he returns from abroad 6 weeks postop, the implant is found to be loose most likely due to retention of a piece of gauze in the mesial socket for hemostasis. The distal socket is also low. After debridement, socket preservation is accomplished with allograft and Osteogen, covered with Collagen plug (Fig.9). Early removal of the retained gauze may save the implant. The tooth #3 also has severe periodontitis. What is new strategy?
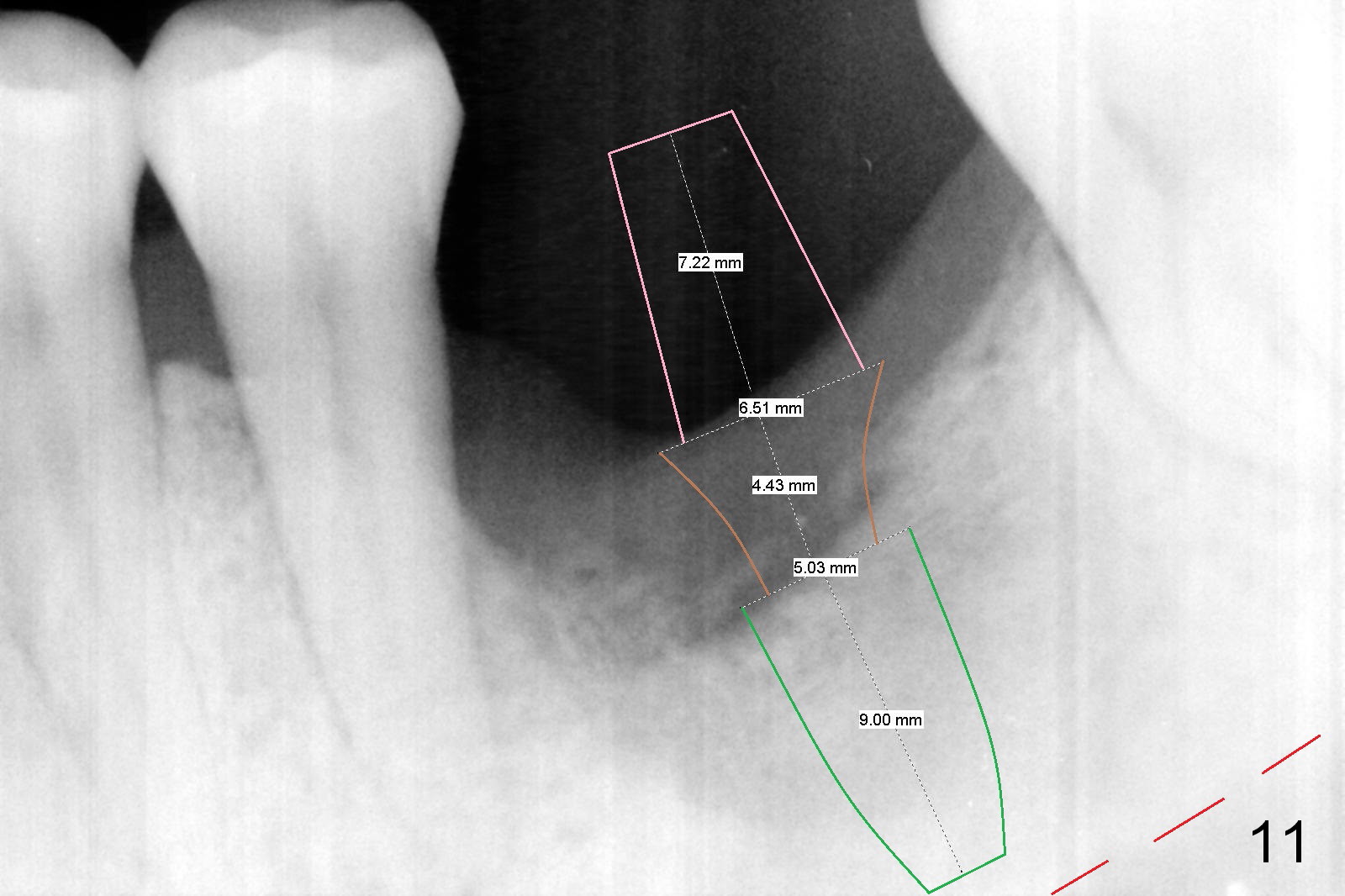
There is bone growth in the mesial socket 5 months post graft (Fig.10). Use Magic Split to get access and test bone density (which must be low or medium in the upper portion). Use drills beyond the socket if necessary. Crown/implant ratio is unfavorable (Fig.11); so progressive loading is essential.
Return to Full Arch,
Lower Molar Immediate Implant,
IBS
3,
9,
23
Xin Wei, DDS, PhD, MS 1st edition 04/25/2016, last revision 04/22/2018