,%20bone%20graft.jpg)



%20from%204.5x5.7(3).jpg)

|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
Narrow Ridge With Thick Cortical Plates
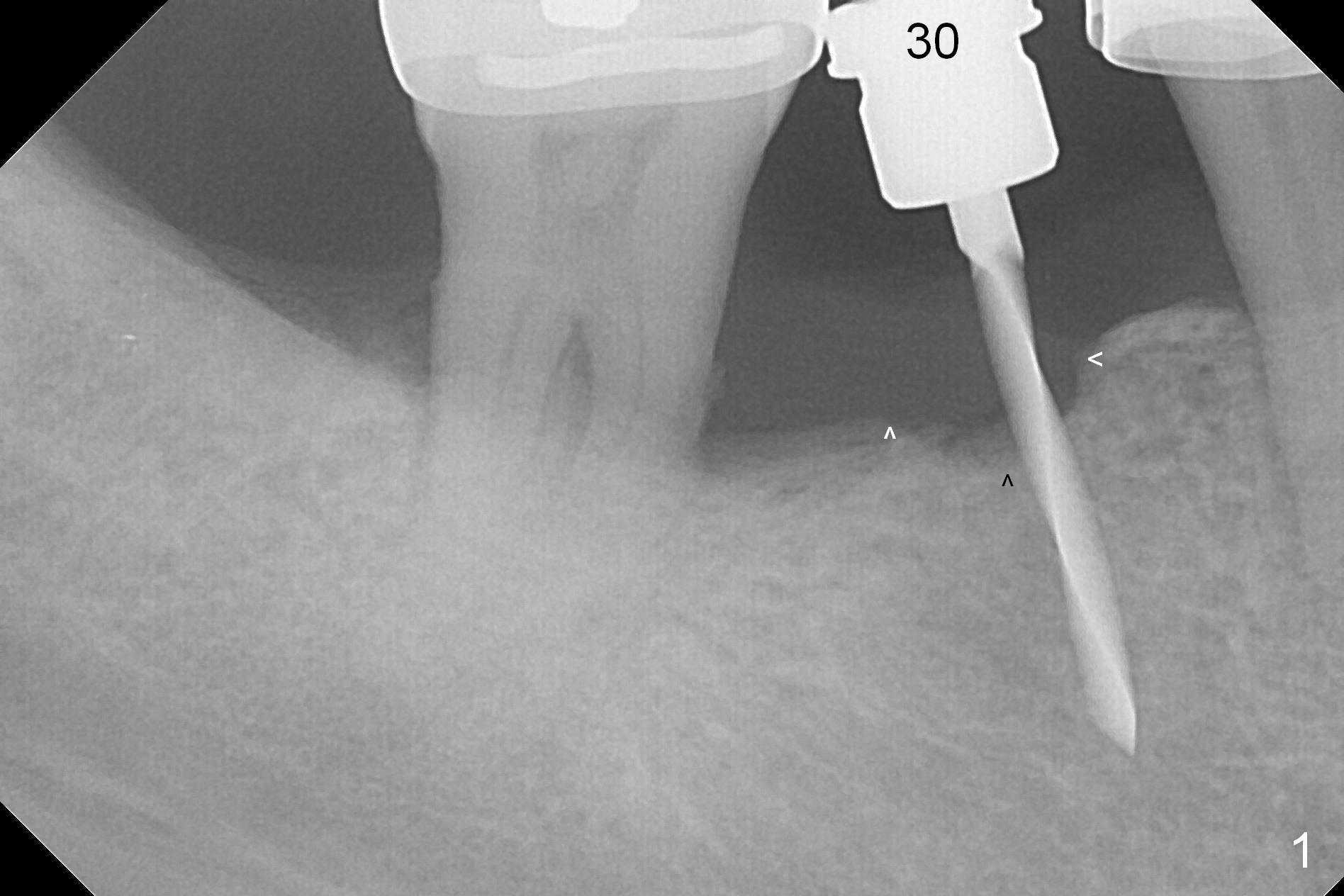
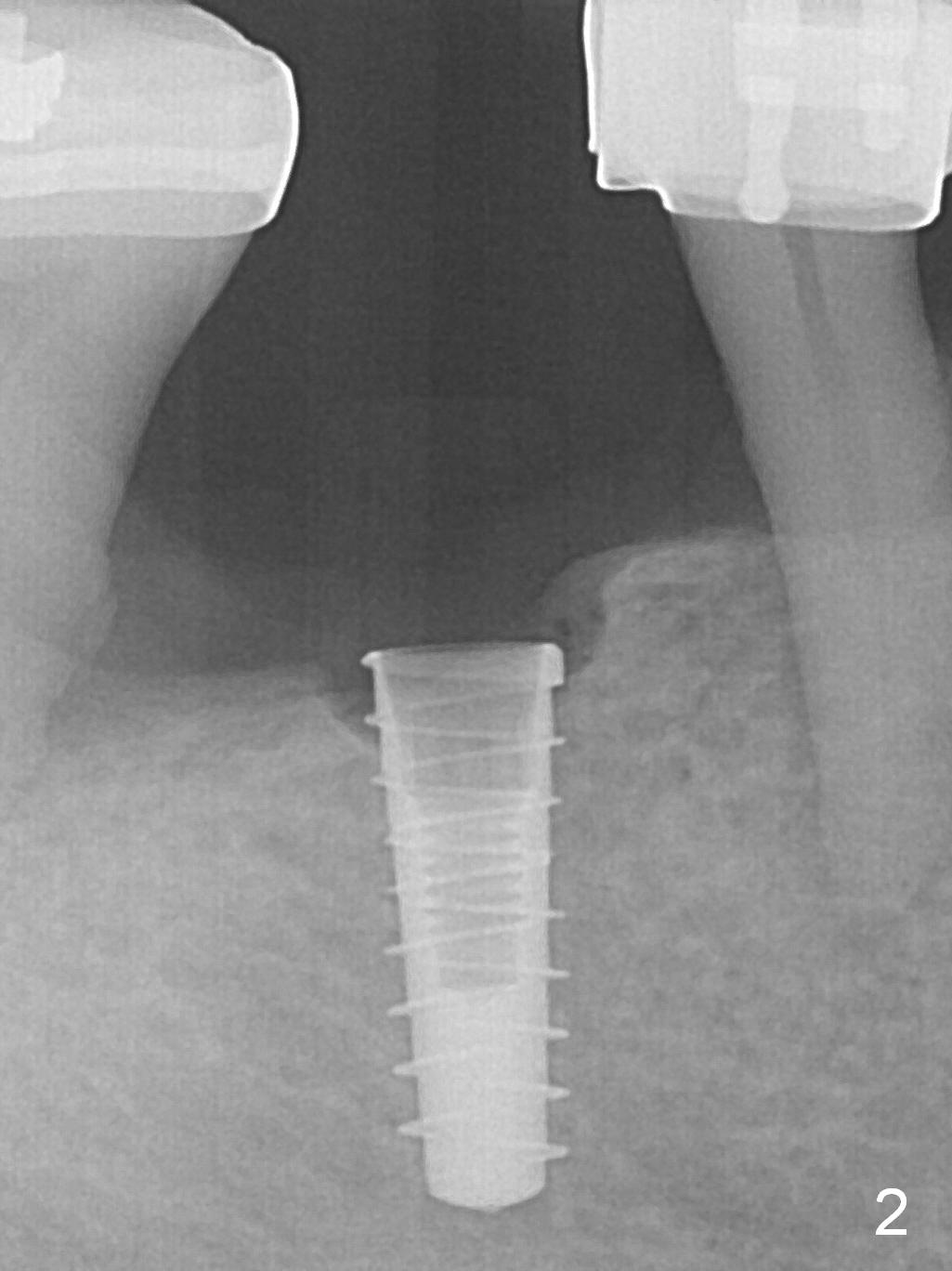
To place an implant in the narrow ridge at the site of #30, the first step is to flatten the ridge as shown by arrowheads in Fig.1. The initial osteotomy by 1.6 mm pilot drill for 9 mm seems to be positioned too mesial and tilts distal. The osteotomy is then moved distal using Lindaman bur. After reusing the 1.6 mm drill for 11 mm, Magic Drill 3.3 mm and final drill are utilized to finish osteotomy. A 4x11 mm IBS implant is placed with better trajectory and insertion torque > 50 Ncm (Fig.2). After further apical placement of the implant (Fig.3 arrow, 6 turns of torque wrench), a 4.5x5.7(3) mm abutment (A) and bone graft (*) are placed (red dashed line: Mental Foramen and Inferior Alveolar Canal).
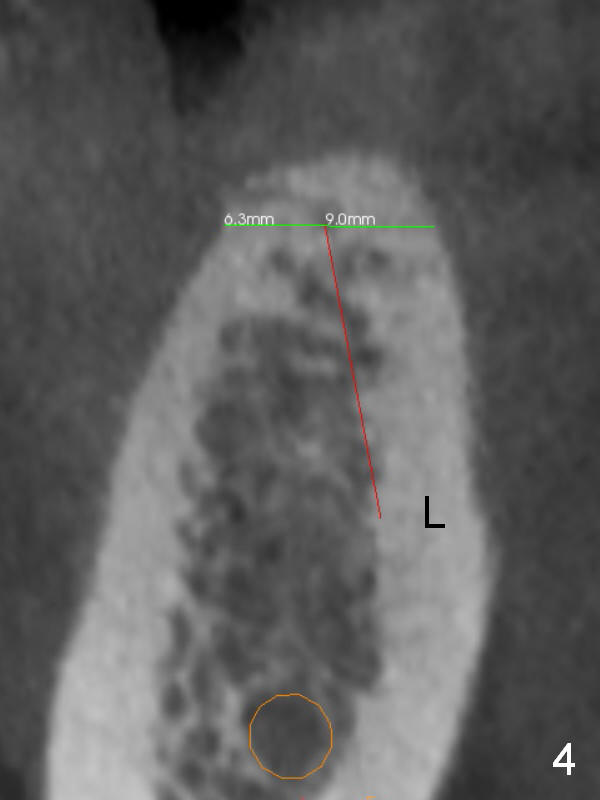
How can the narrow implant achieve such high torque value? After ridge top trimming (Fig.4 green line), it is difficult to extend the 1.6 mm pilot drill (Fig.4 red line) for the last few mm. The drill must encounter the lingual cortex (L). When the 4x11 implant (Fig.5 green box) is placed, it must contact both the crestal (C) and lingual cortices.
Periodontal dressing is removed 2 weeks postop. A nonfunctional provisional is fabricated 3 weeks postop because of the narrowing edentulous space. A .018 ss wire is placed 6 weeks postop.
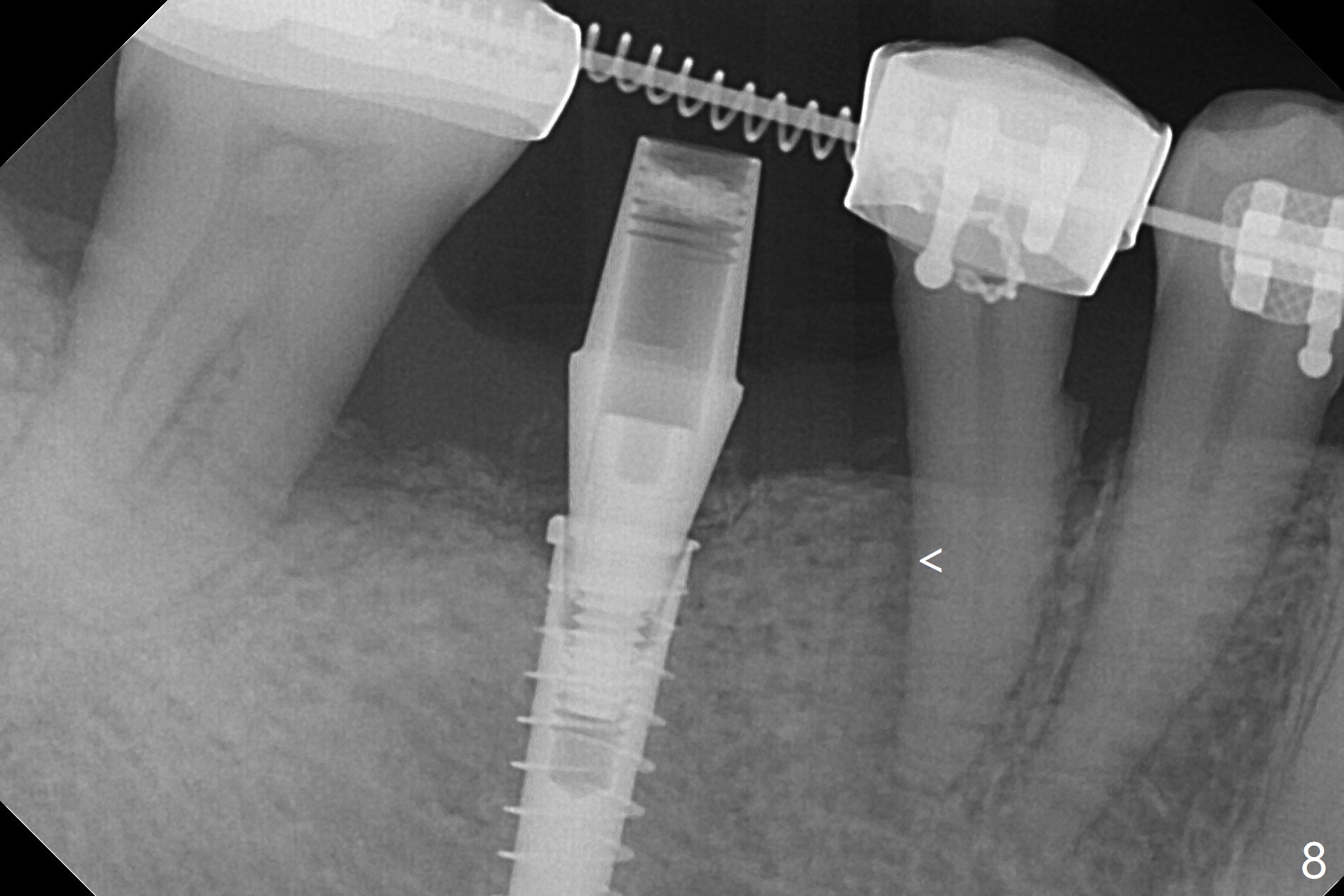
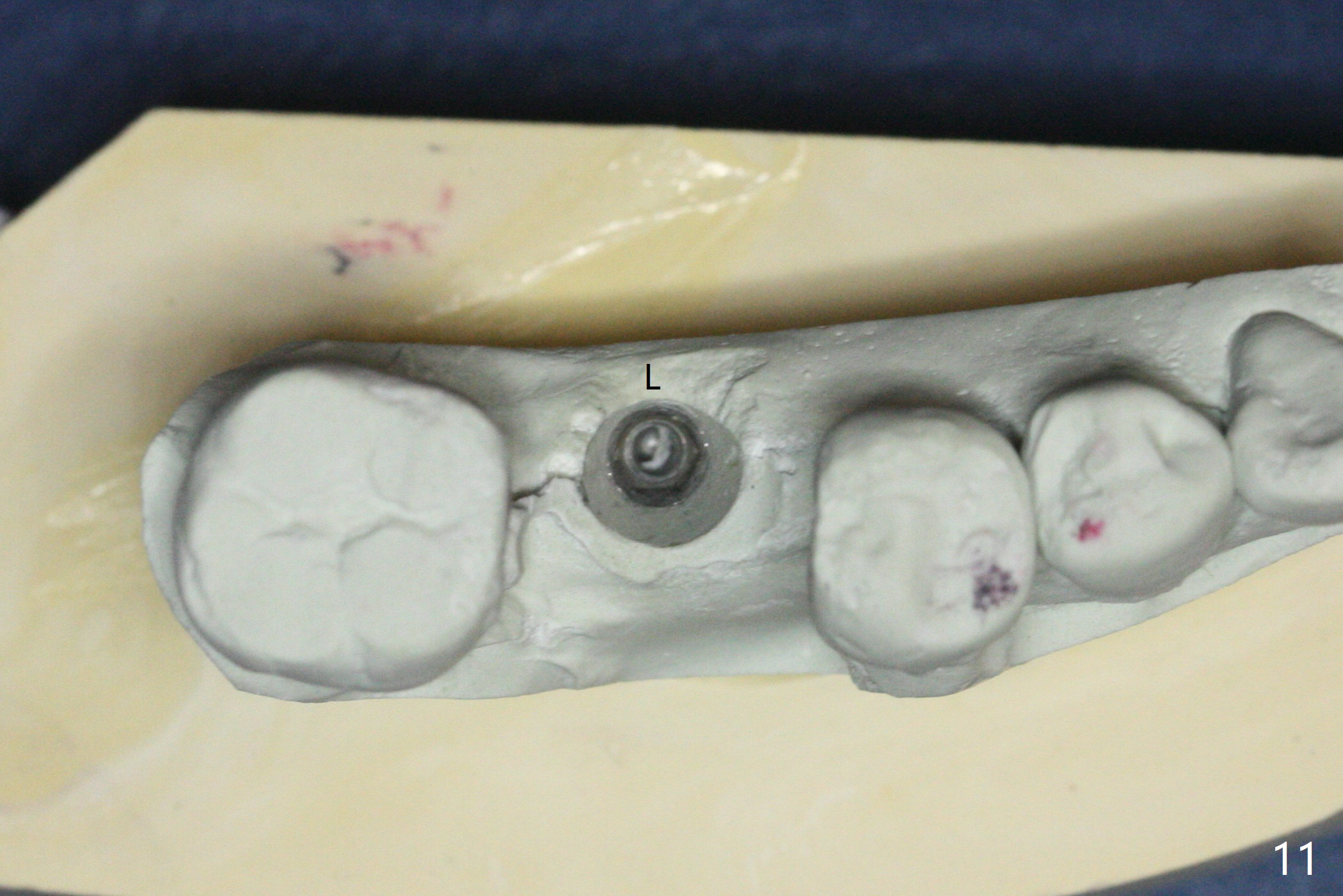
The tooth #29 is distalized (relapse)10 weeks postop (Fig.6, after removal of 18 ss wire). The coronal bone loss is minimal (Fig.7); later an open coil spring is placed between #29 and 31. Eight weeks later, the tooth #29 is mesialized with wide distal pdl (Fig.8 <). In fact, the implant at #30 is not used as an anchorage. The lamina dura reforms 3 months post cementation (Fig.9 <). The occlusal contact is limited between upper and lower molars (Fig.10). The implant was placed lingual (Fig.11 model for occlusal porcelain addition at #30)).
Return to
Lower
Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 02/16/2017, last revision 05/30/2019