












|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
Upright 2nd Molar
Pre-implant exam shows that the tooth #31 has mobility I (Fig.1). Treatment plan changes to extraction of #32, scaling & root planing (SRP) of #31, and banding of #29 and 31 and bracketing from #22 to #28 (Fig.2,3). Why do we not place a bracket for #29?
After SRP at #29 and 31 and extraction of #32 (Fig.5,6), PA is taken; it appears that more SRP should be done at #31 mesial, #29 mesial and 28 distal (Fig.7). Since the tooth #29 has been prepared, a #22 copper band (Fig.8 *) has to be placed before placement of the smallest orthodontic band. To have better anchorage, brackets are placed apparently more than necessary (Fig.9). When the tooth #29 is mesialized by placing an open coil spring between #29 and 31, place figure 8 wire for all of the brackets as a unit to distalize the tooth #31.#29 and 31.
The wire has been changed to 16 niti. Next appointment change to 18 SS and place open coil spring. When the tooth #29 is mesialized, use figure-8 wire between #27-29.
In fact the tooth #29 is not stable (mobility I) and has contact with #28. Figure-8 wire is placed immediately between #26 and 29 (Fig.12). The distal end of 18 SS segmental wire is intentionally left longer than expected (Fig.13 >). The mesiodistal edentulous space is 4 mm. When the tooth #31 is distalized >2 mm (Fig.14), an implant can be placed. The figure-8 wire prevents the tooth #29 from rotation from white line to red line.
If the tooth #29 turns out again to be rotated and lingualized because of the coil spring, stop using it, place a tomas-pin SD mesial or distal to #29 (Fig.10,11) and a tomas-uprighting spring.
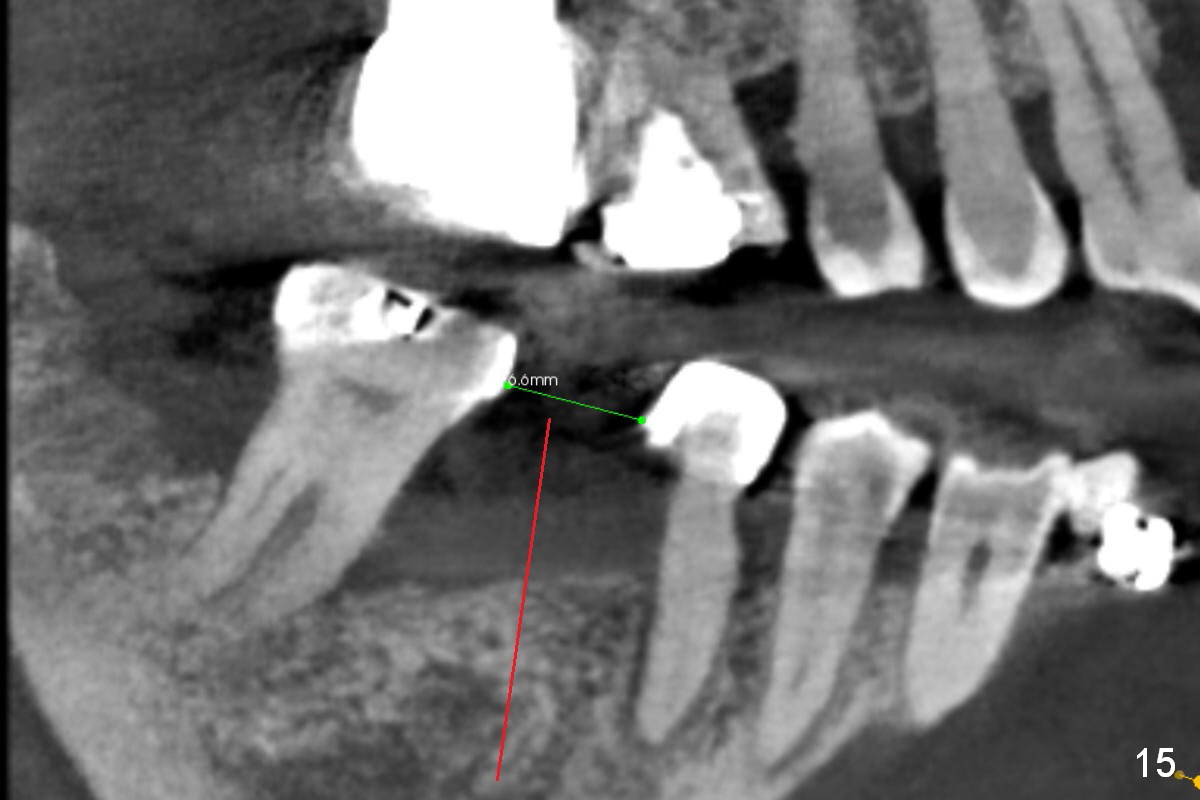
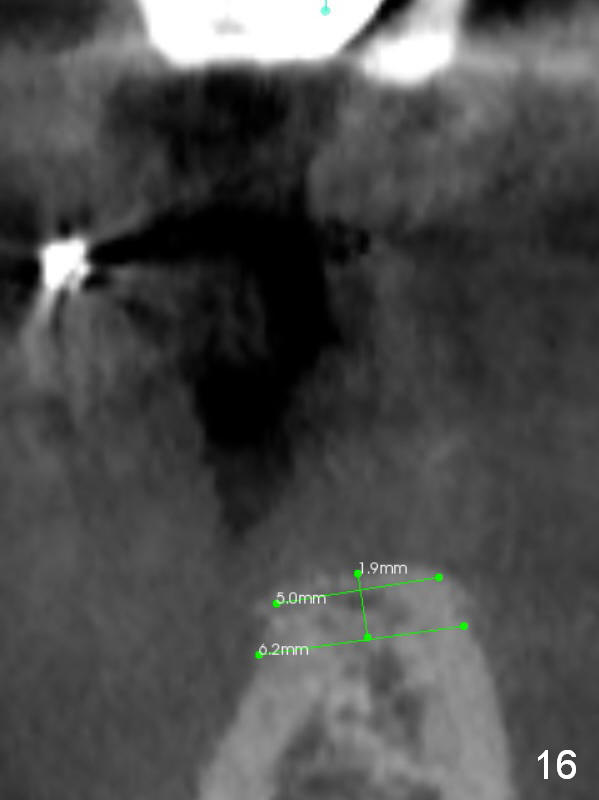
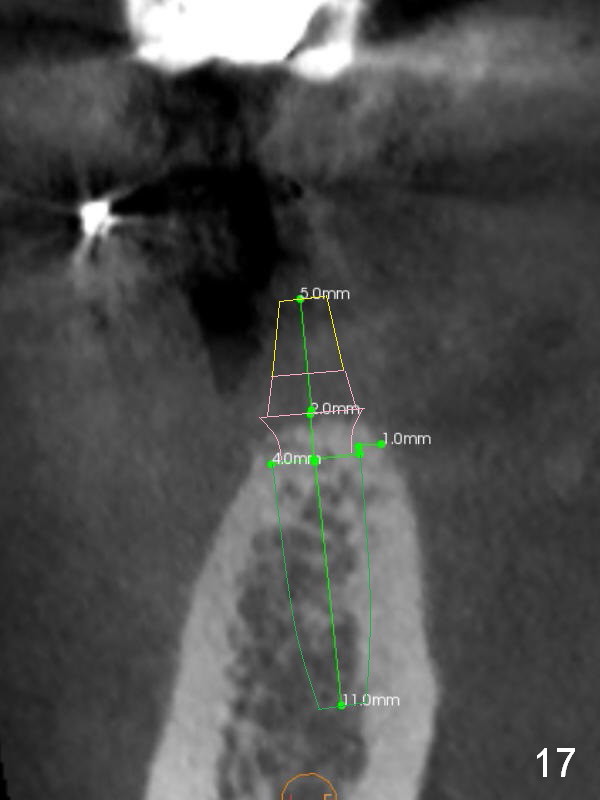
The edentulous space increases to 6.6 mm 5.5 months of orthodontic treatment (Fig.15 CT). The trajectory of osteotomy (red line) is parallel to the long axis of the tooth #29. The buccolingual width of the ridge is 5 mm on the top (Fig.16 coronal section). The ridge will be trimmed down ~ 2 mm so that the width will be 6 mm to accommodate 4 mm implant (Fig.17). The trimming is oblique (lower buccal, higher lingual, parallel to the occlusal plane of the opposing tooth).
The drawback of the narrow implant (4 mm) in the molar region is potential fracture of the thin coronal wall of the implant and/or abutment screw. IBS implant is made of Titanium V, which is stronger than Titanium IV. Furthermore Magicore is a type of 1-piece implant (Fig.17 green (implant portion) and pink (abutment portion)). There is no issue of breakdown of implant wall or screw. A solid abutment is used to facilitate restoration (yellow). In fact Magicore is not used because of run out inventory.
Return to
Lower
Molar Immediate Implant,
Implant & Ortho,
#2
Xin Wei, DDS, PhD, MS 1st edition 10/26/2016, last revision 08/15/2018