


,%20graft.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
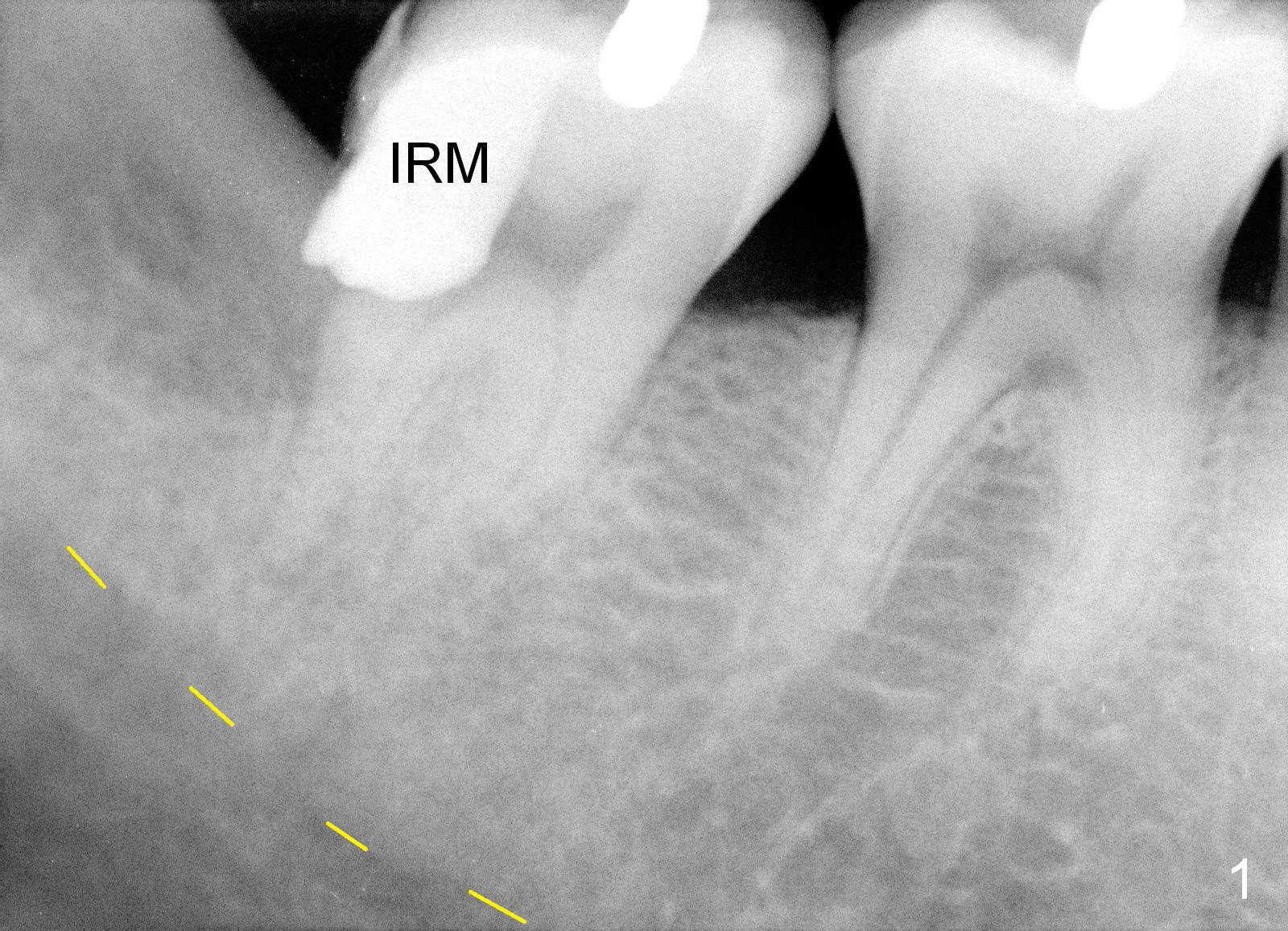
Septum Fractures While the Fused Lower 2nd Molar is Being Extracted
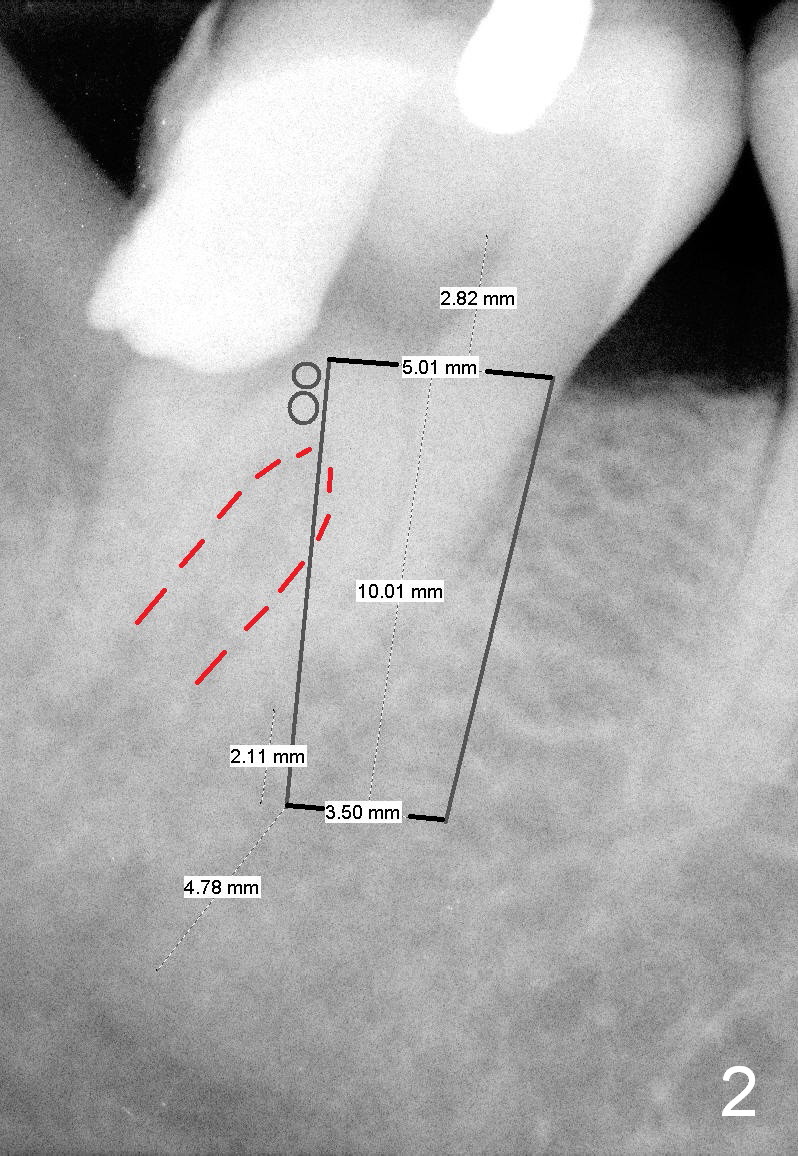
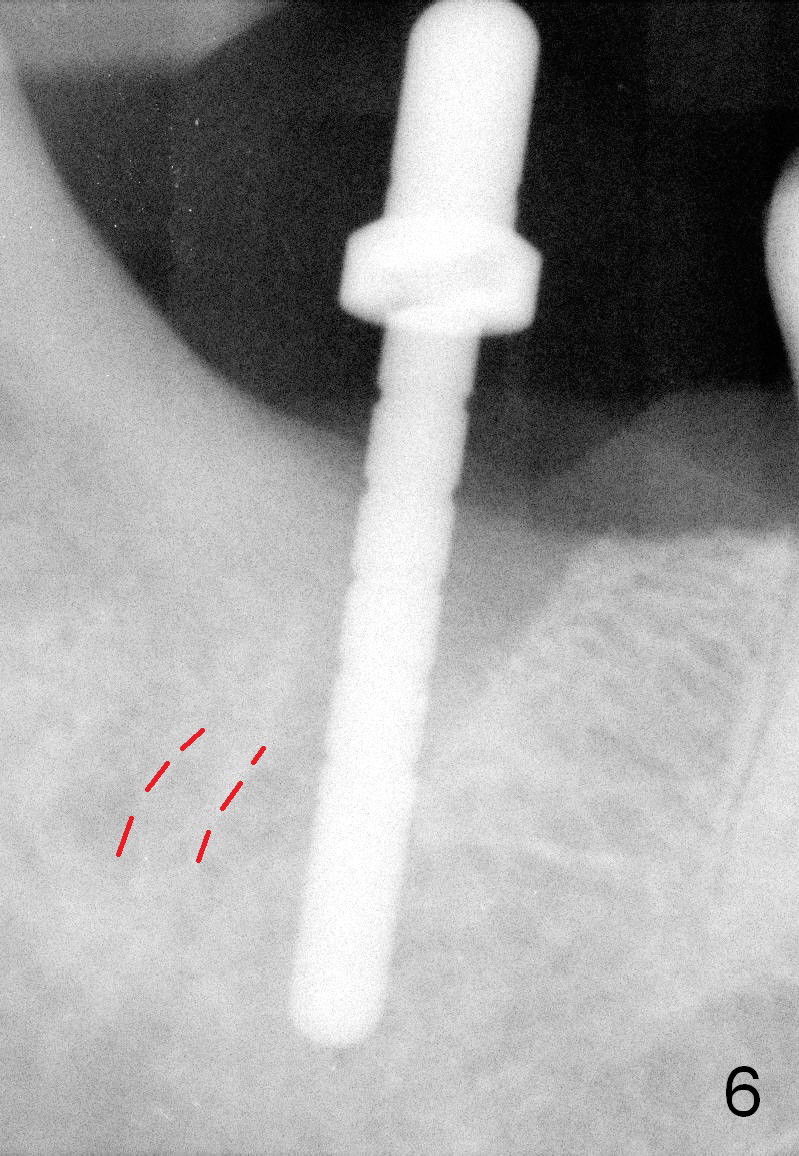
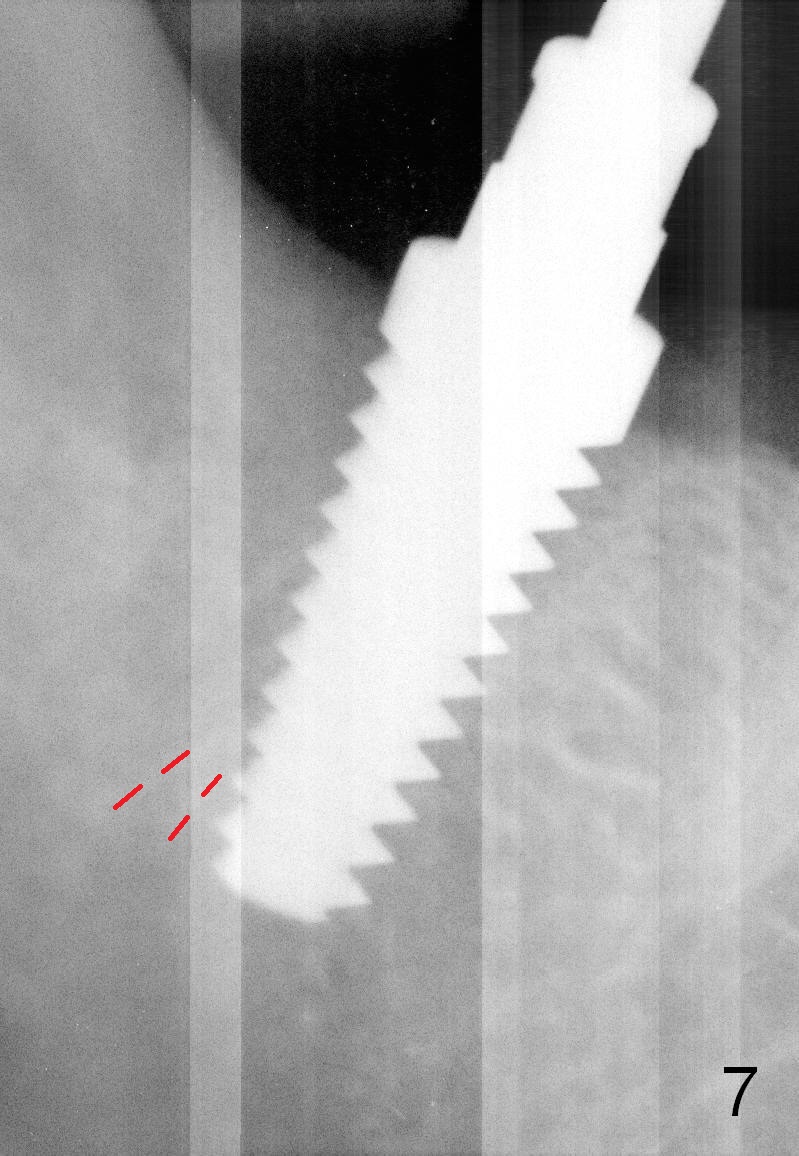
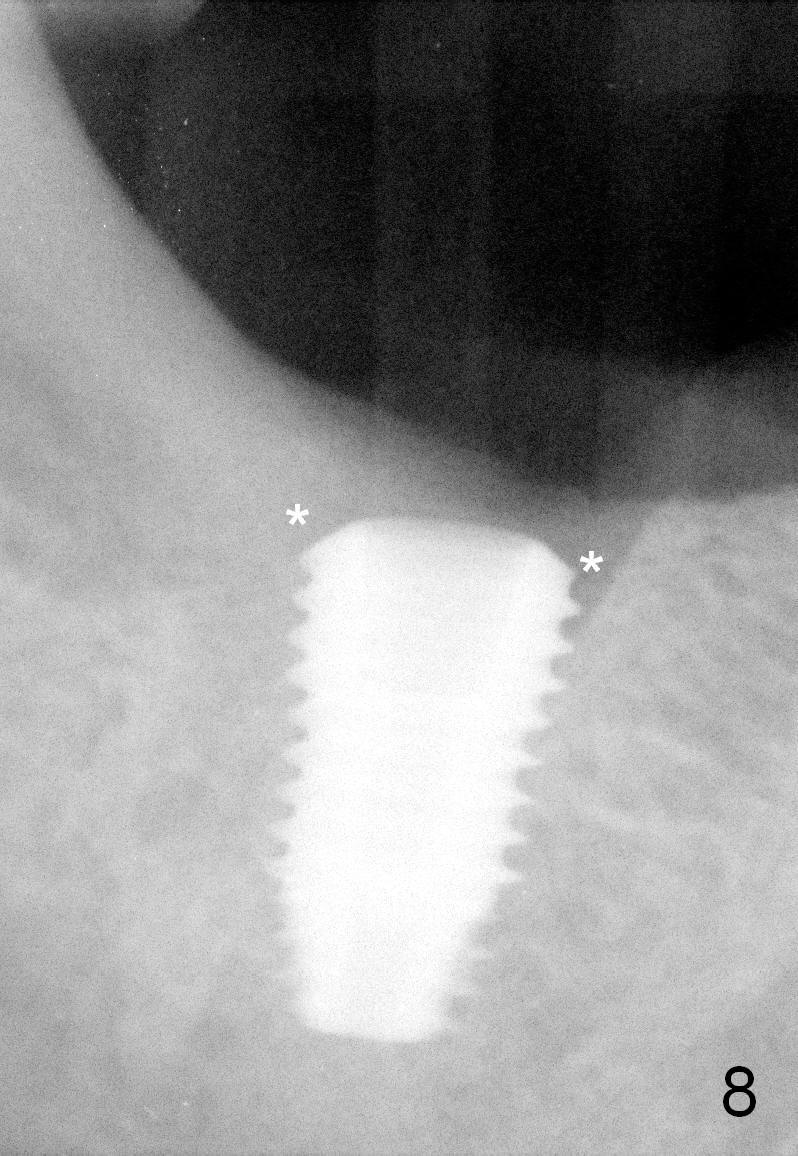
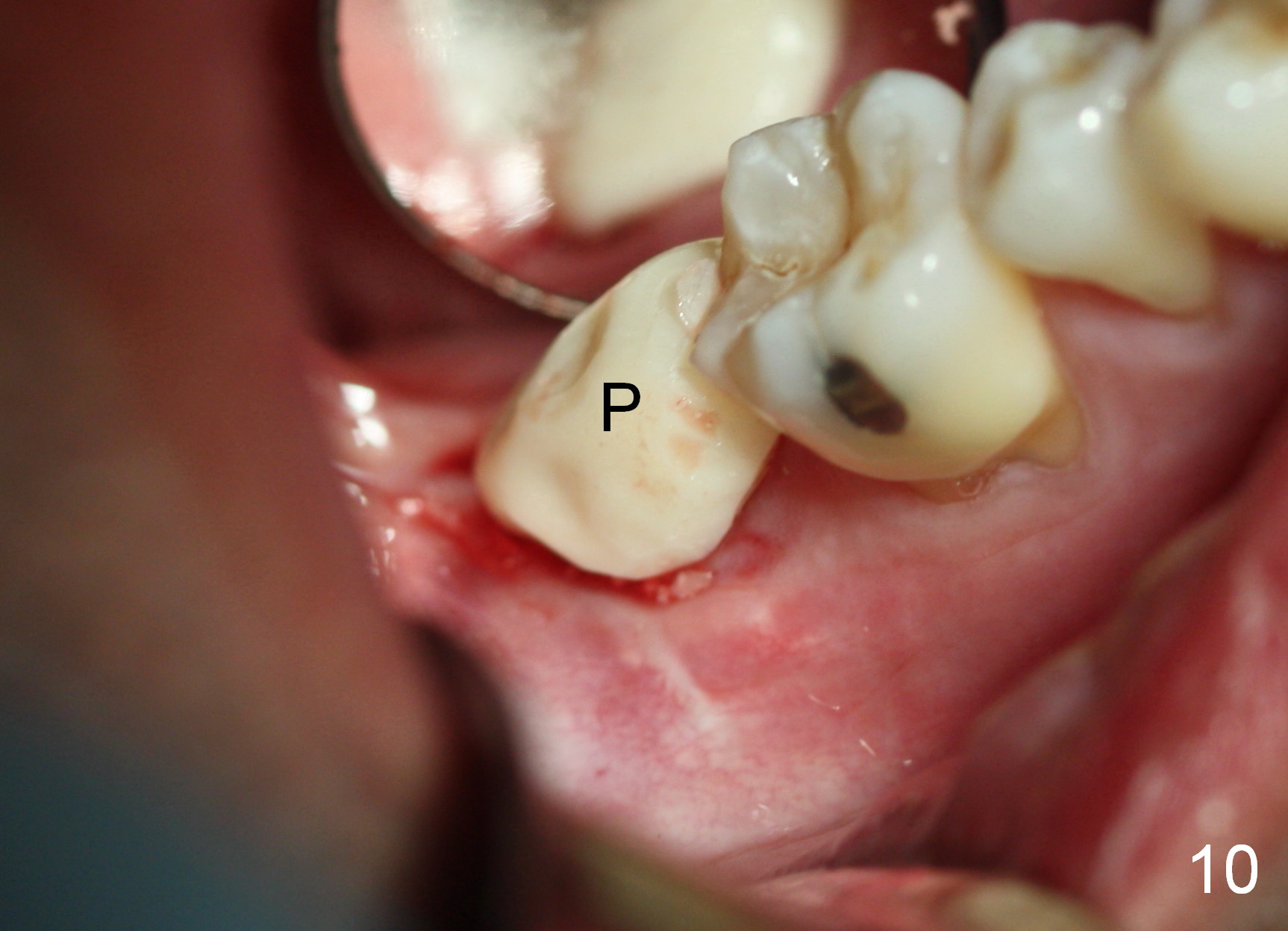
When the patient returns for treatment, he insists on saving the tooth #31, which is post pulpotomy (Fig.1 IRM). IRM is dislodged while accessing the distal orifice. Sodium Hypochlorite leaks. It is difficult to proceed with root canal therapy. After discussion, the patient consents to extraction and immediate implant. As planned, the septum (Fig.2 red dashed line) provides implant (black outline) with stability, but it is fractured while the tooth is extracted (Fig.3-5). Osteotomy is still initiated mesial to the remaining septum (Fig.6 red dashed line; i.e., in the mesial slope of the socket). The opening of the socket is 6x9 mm. When a 6x17 mm tapered tap is inserted at the depth of 14 mm (gingival level), it is stable (Fig.7). A 5.9x10 mm bone-level implant is placed with insertion torque ~ 55 Ncm (Fig.8). The coronal gaps (Fig.8 *) are filled with allograft and Osteogen (Fig.9 *); a 6.8x4 (3) mm abutment (Fig.9 A) is placed for an immediate provisional (Fig.10 P).
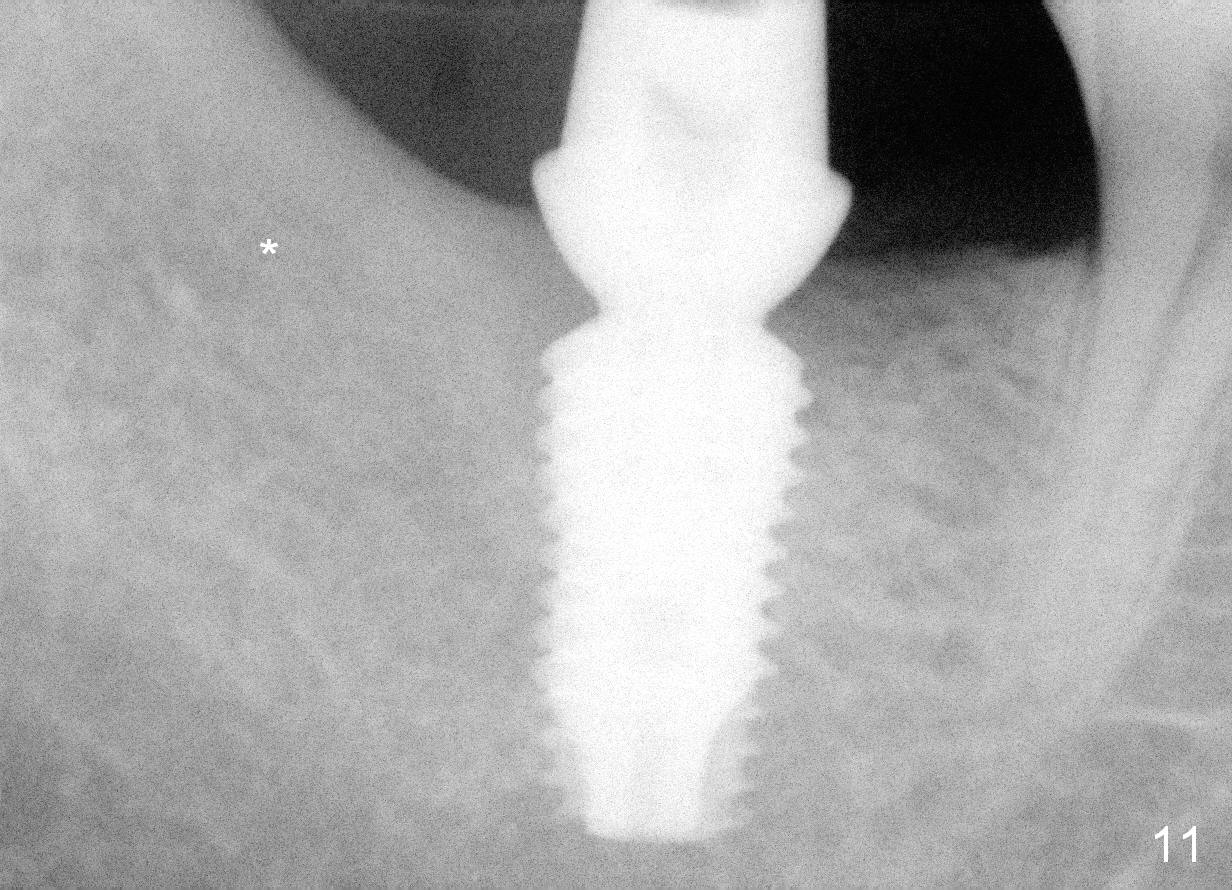
Six months later, the provisional perforates on the top of the abutment. It suggests that the patient has chewed with the provisional. When the provisional is removed, the occlusal clearance appears to have been reduced, suggesting that the opposing tooth has supraerupted. However, osteointegration and bone regeneration at crest have not been disrupted (Fig.11). The 3rd molar socket has also healed (*, compared to Fig.1). It appears that the tooth #18 should receive the same treatment.
Return to Lower Molar Immediate Implant,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 06/24/2015, last revision 04/11/2017