|
|
|
|
|
|
|
|
|
|
|
|
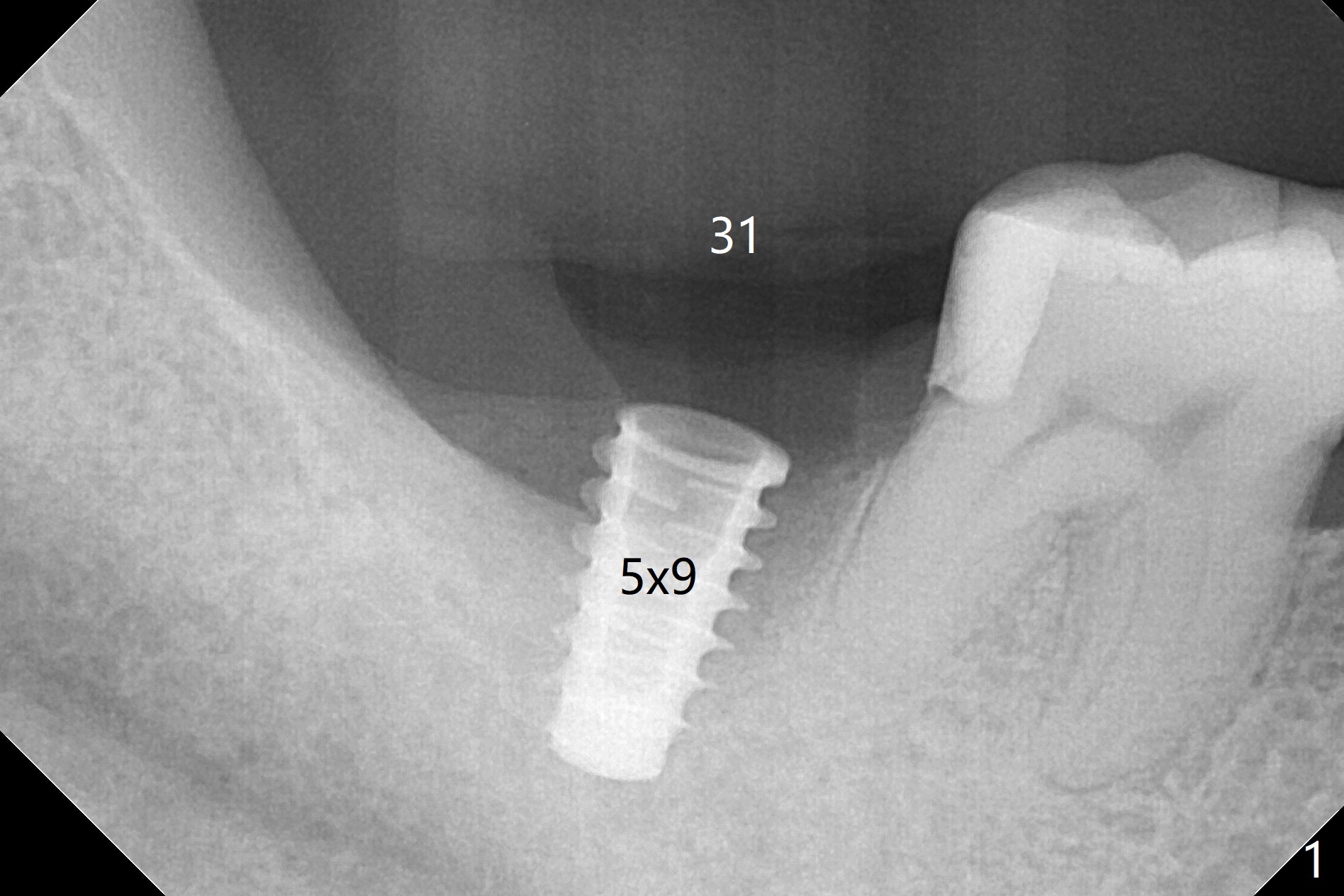
How to Improve Immediate Implant with Limited Native Bone?
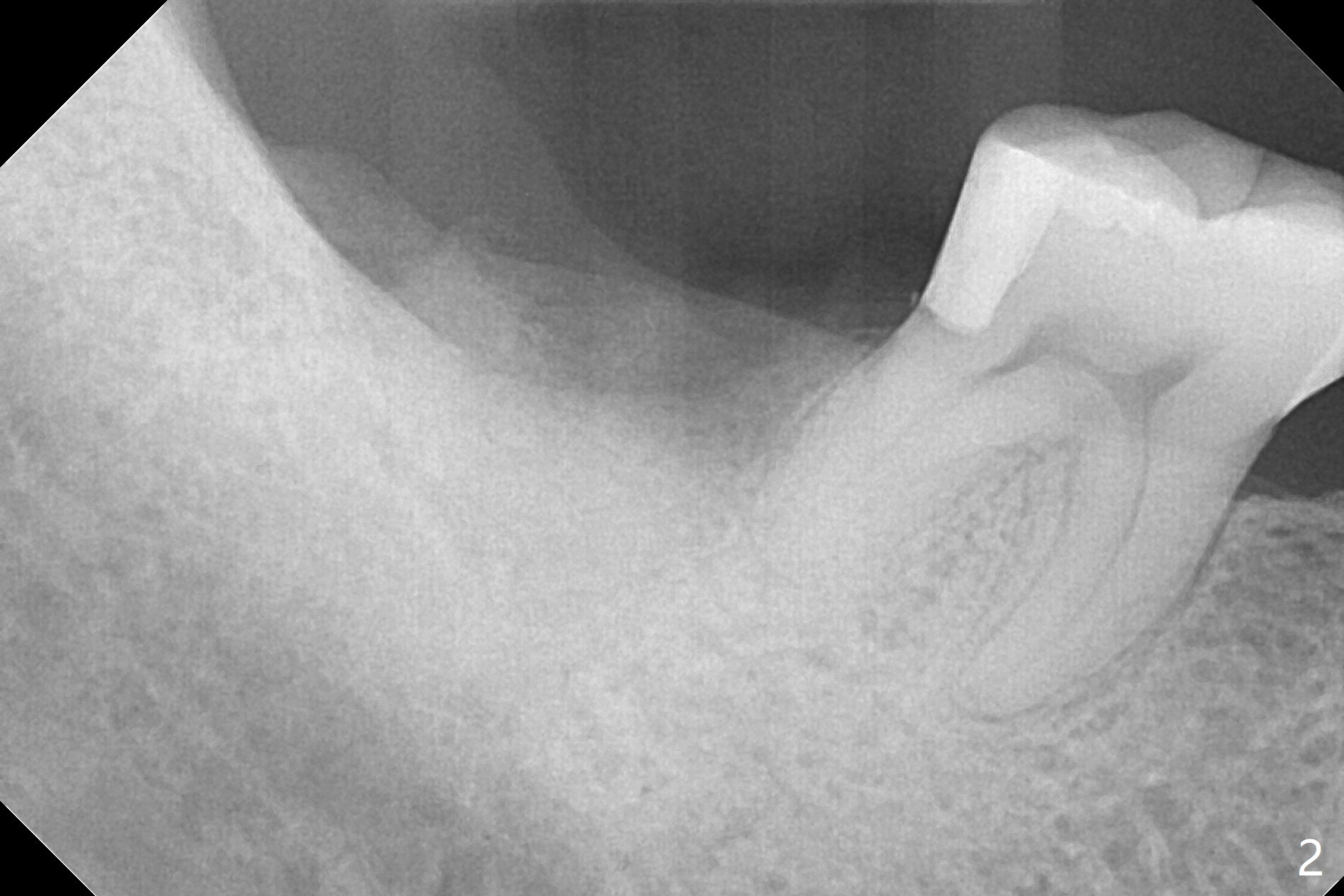
As expected, the buccodistal plate is low after extraction at #31. Osteotomy is initiated mesiolingually with 2 mm initial drill, 2.8 and 3.6 mm round drill with 4 mm stopper. The patient feels pain before the last drill reaches the depth. A 5x9 mm IBS dummy implant is placed with stability (Fig.1). When the definitive implant (5x9 mm) is placed, stability is lost. A 5.5x9 mm dummy implant achieves stability, while the definitive one loses stability. Increase in depth with 4.3 mm Magic Drill meets pain. Hemorrhage is another factor. When hemostasis is temporarily controlled, bone core is found. Nor removal of bone core with Final Drill or addition of allograft (Vera, .2-1.0 mm) in the osteotomy helps obtaining stability. Finally socket preservation is performed (Fig.2).
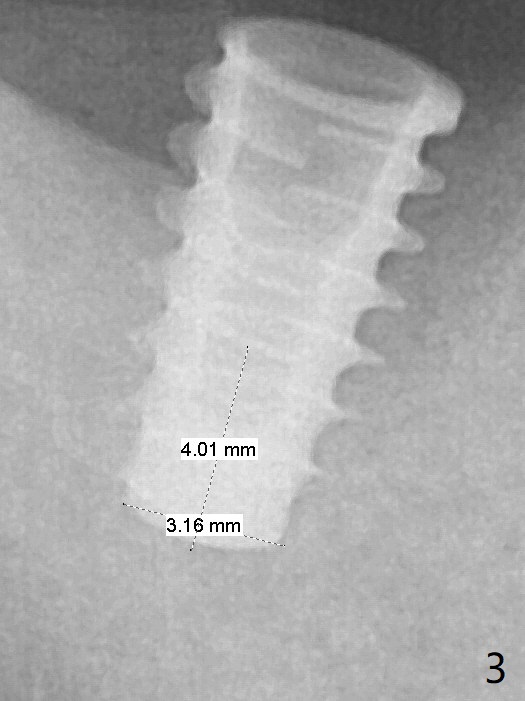
With pain and hemorrhage, the depth of osteotomy is unable to be achieved. Second the osteotomy is over prepared (Fig.3). Ideally after use of 2.8 mm round drill, a 4 or 4.5x9 mm dummy implant should be tried. In fact use of a shorter drill (4.3 mm in diameter) in Sinus Magic Kit with 4 mm stopper is a better match with the implant. When the implant becomes loose, use autogenous bone (before grinding) or Vanilla (.5-1.0 mm larger particles than Vera) may close osteotomy space.
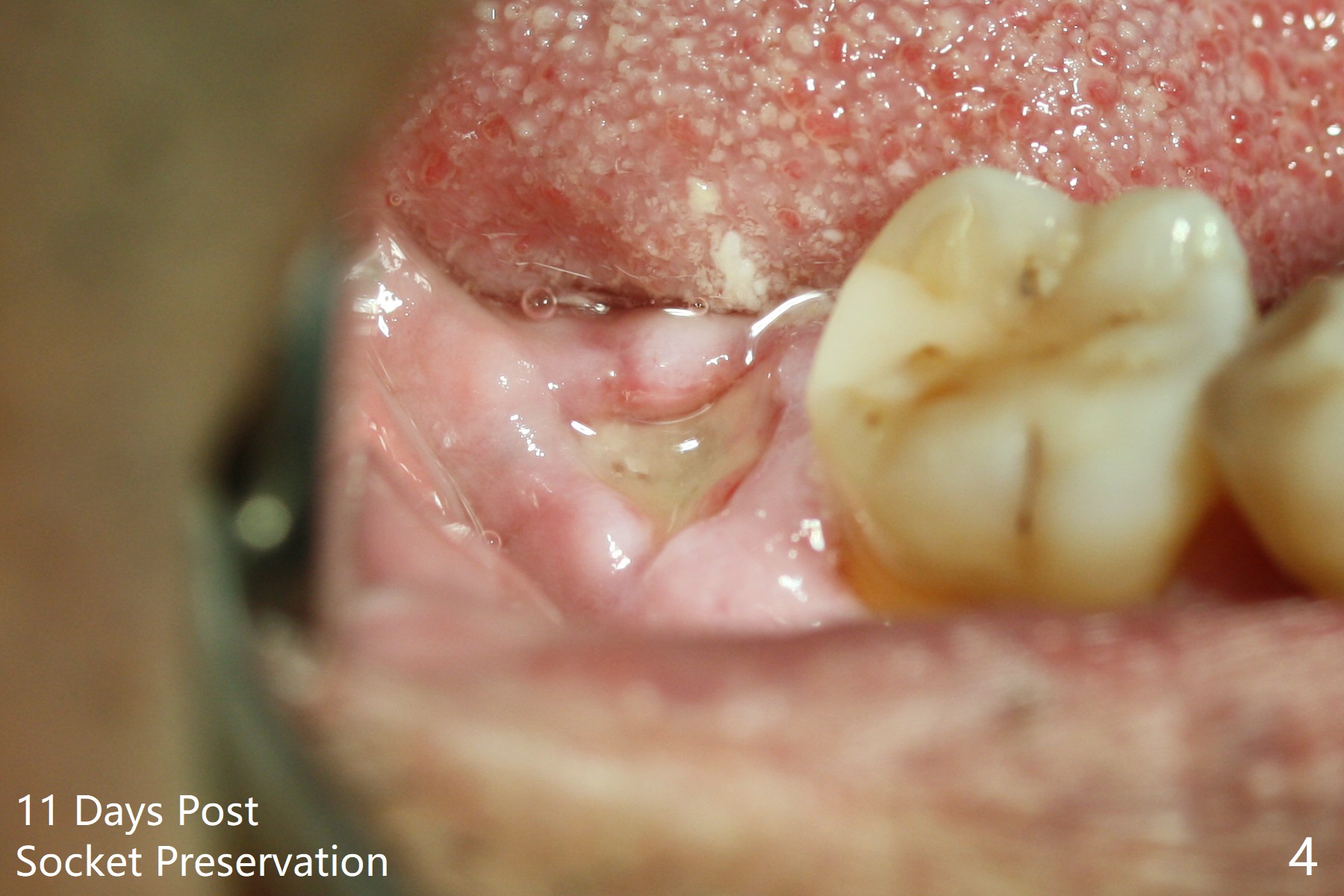
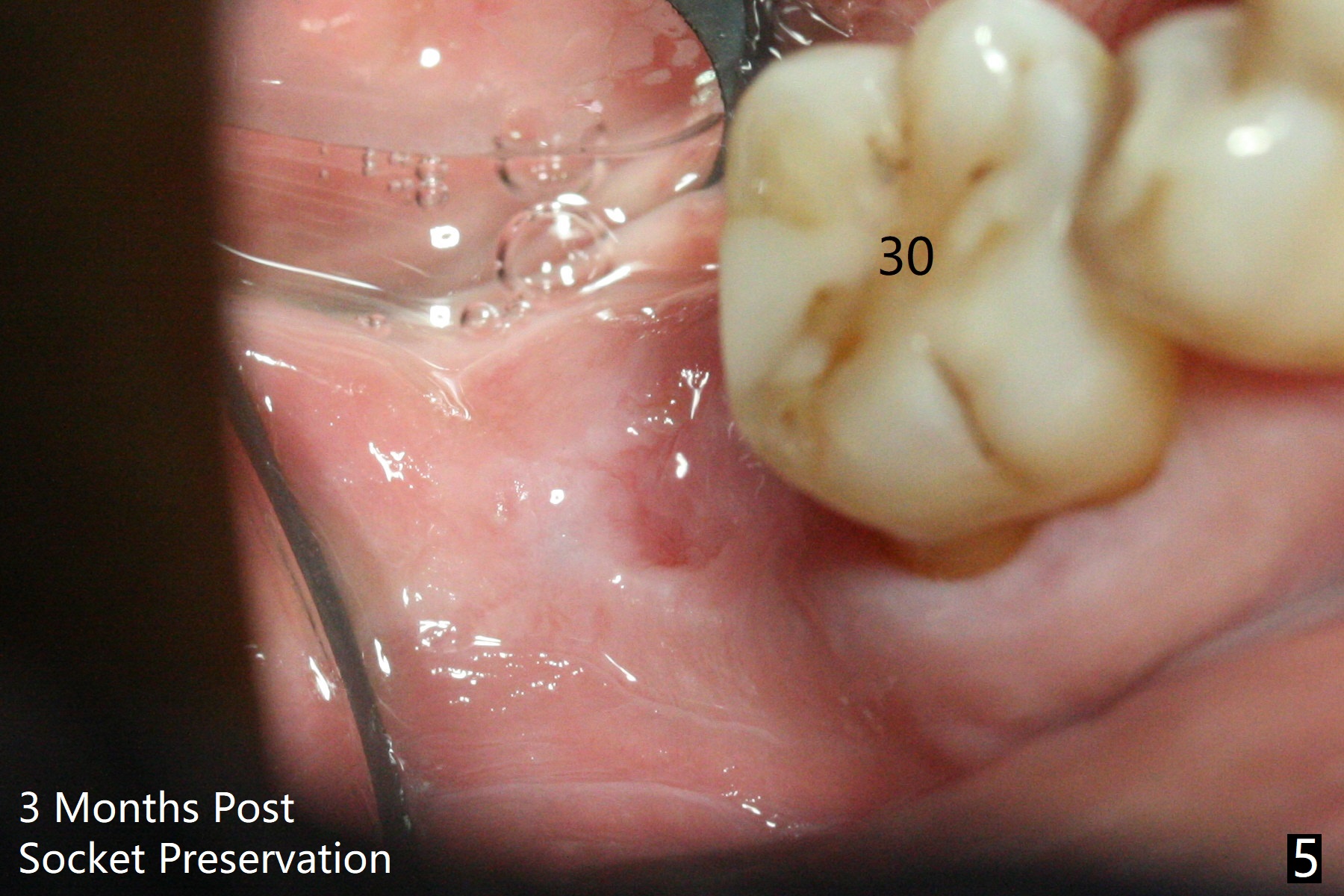
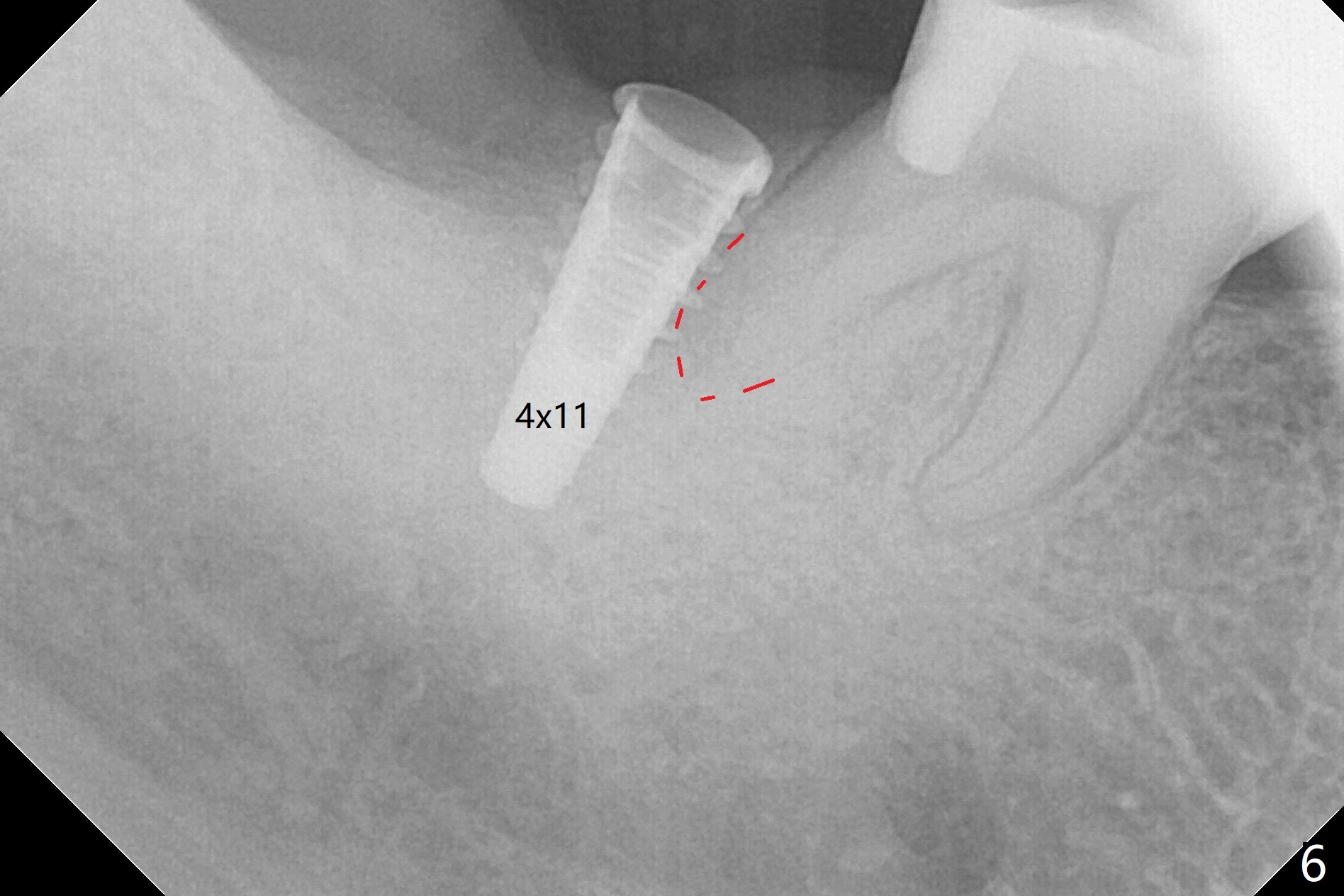
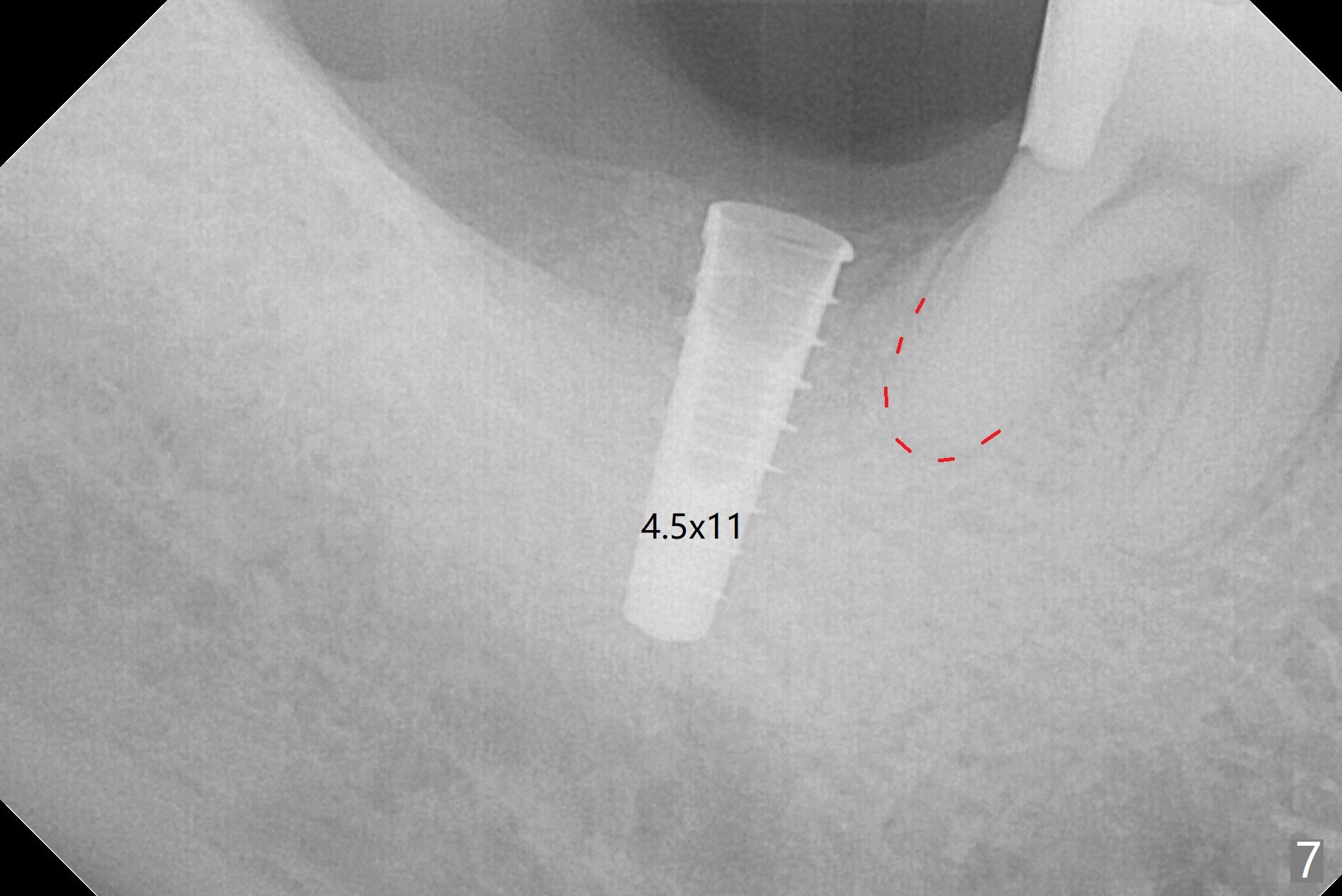
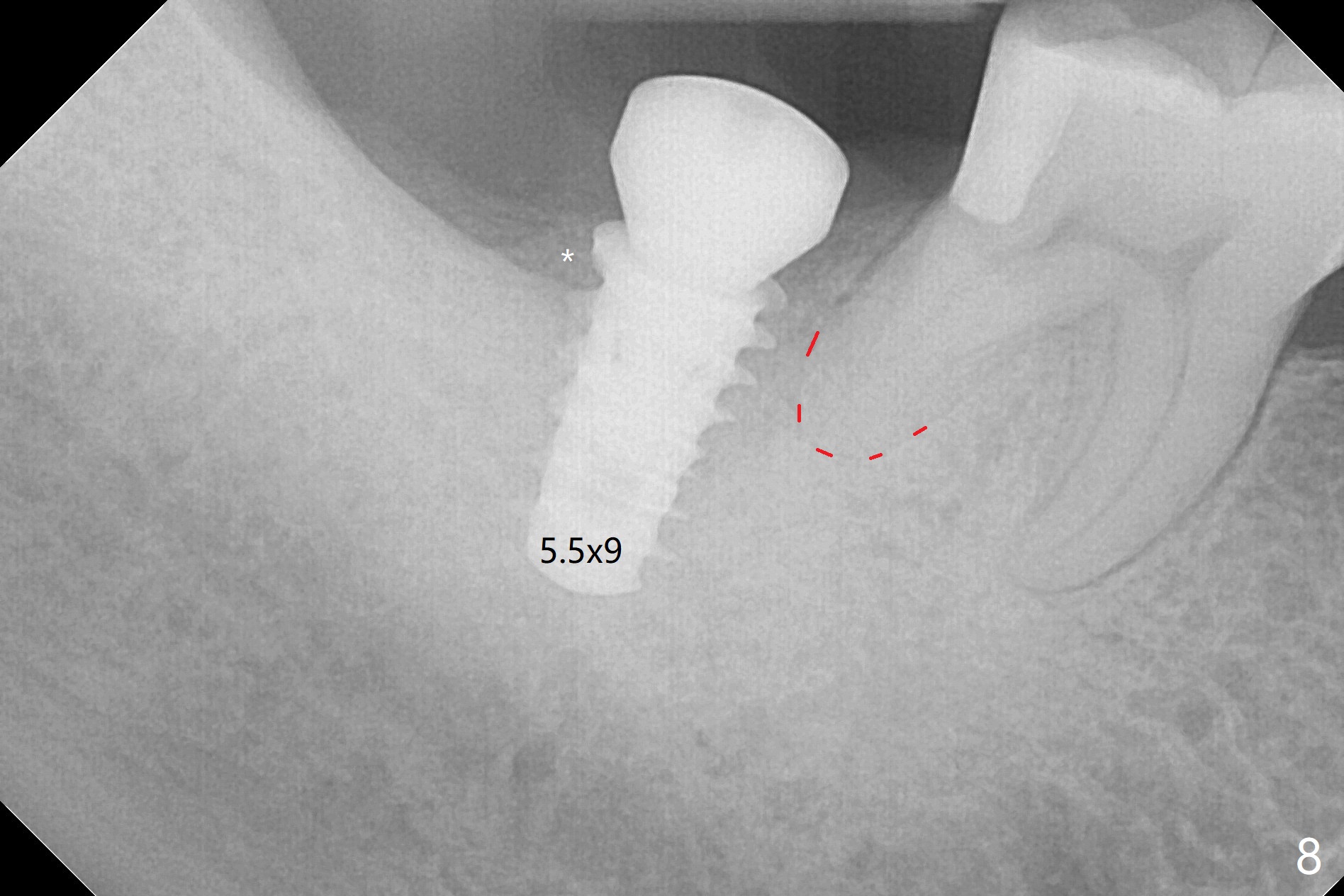
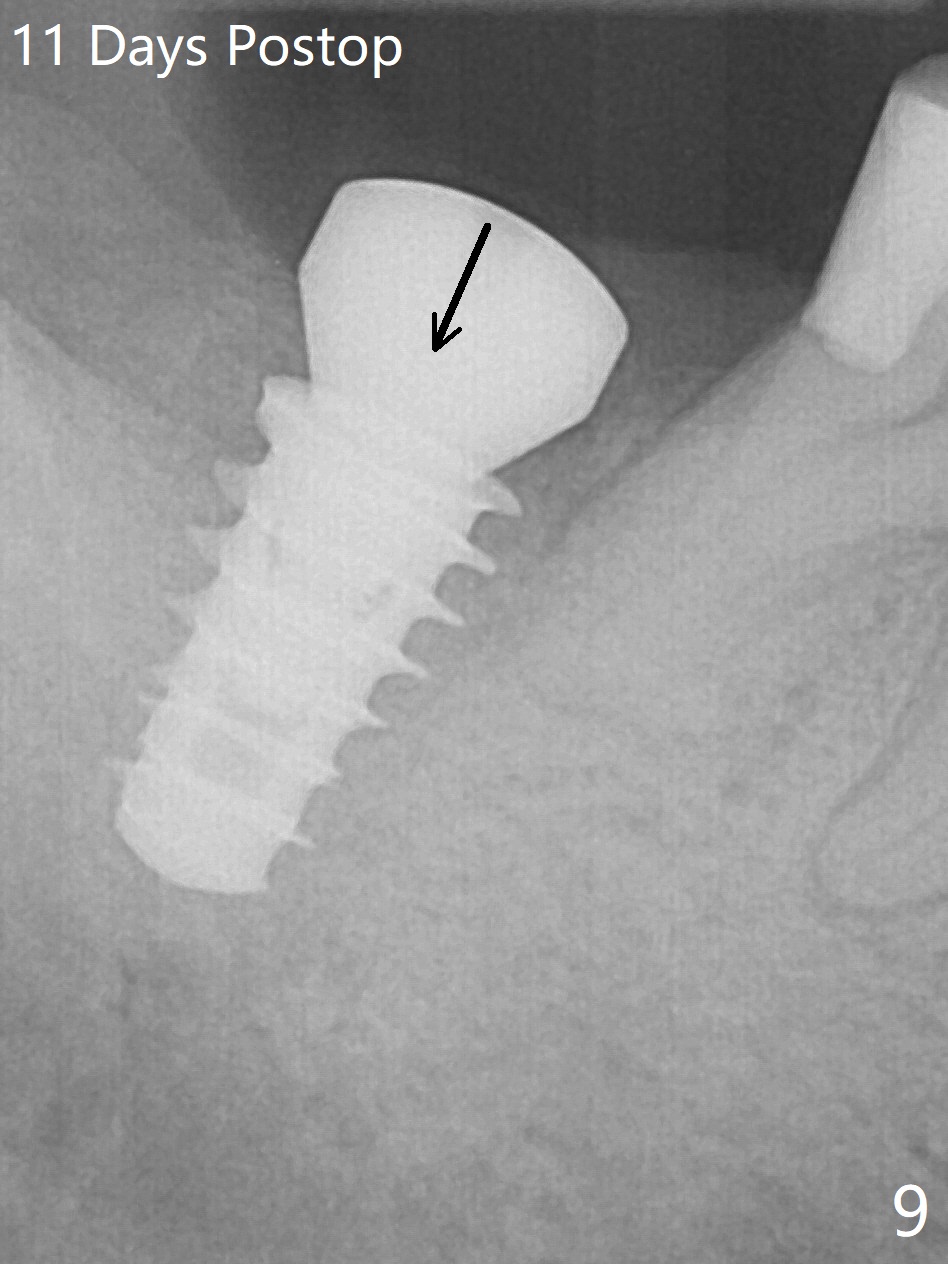
The socket shrinks with buccal plate reduction 3 months post socket preservation (Fig.5), as compared to 10 days postop (Fig.4). To restore the socket as much as possible, Magic Split is used (flapless), followed by Magic Expanders 3-3.8 mm for 11 mm (gingival level) and a 4x11mm dummy implant (Fig.6). The osteotomy is moved distal by using Lindamann bur; following 3.8 mm Magic Drill, a 4.5x11 mm dummy implant (Fig.7). Finally a definitive 5.5x9 mm implant is placed with <45 Ncm; a 6x2 mm healing abutment is placed to close the access (Fig.8). Autogenous bone harvested from the Magic Drill returns to the osteotomy mainly buccal prior to implant placement (Fig.8 *). The patient reports no discomfort immediately postop, thanks to the flapless technique. The patient has had postop pain; 11 days postop, the abutment and implant are found to be loose. After re-tightening by hand, the complex is seated deeper and more stable (Fig.9 arrow).
Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments 14 15/18 Xin Wei, DDS, PhD, MS 1st edition 10/13/2017, last revision 05/27/2019