

|
|
|
|
|
|
|
|
|
|
|
|
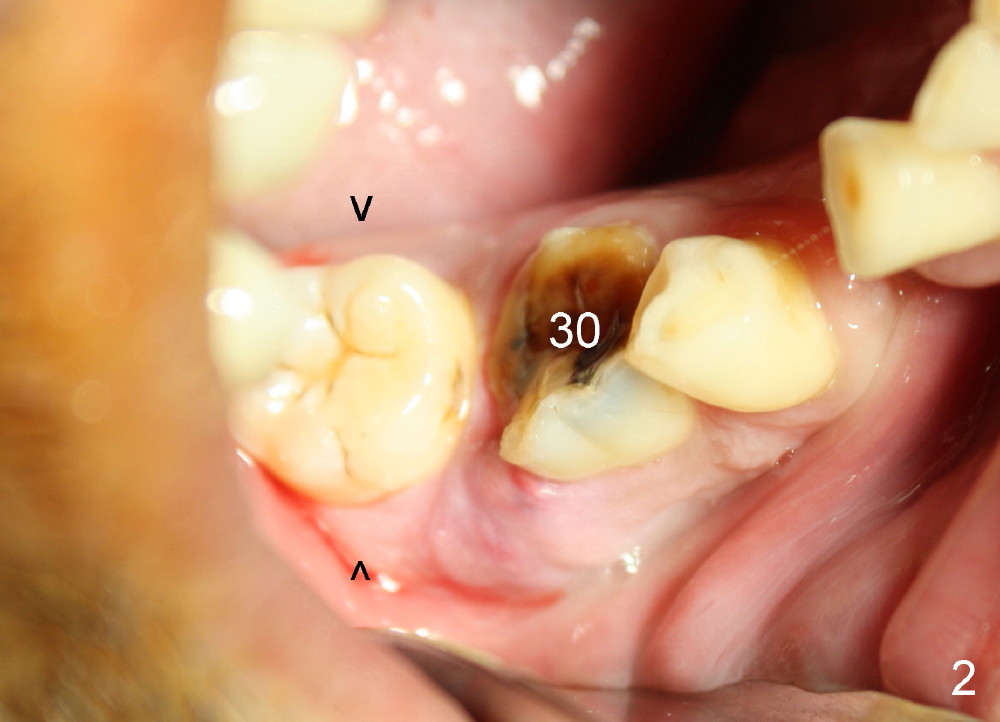
Pain Control for Immediate Implant in Severely Infected Site
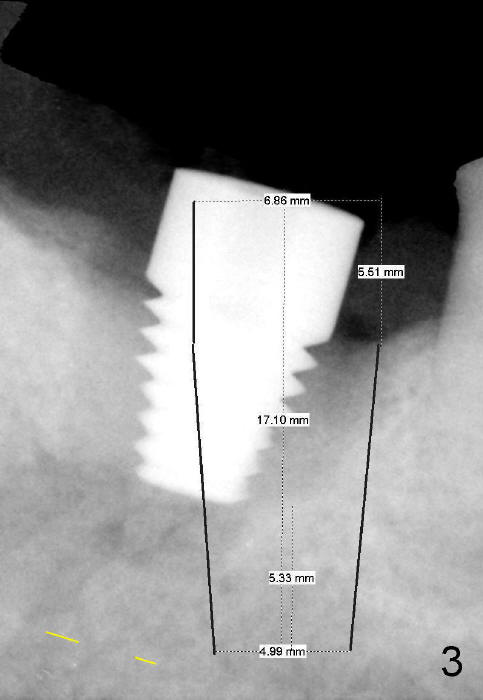
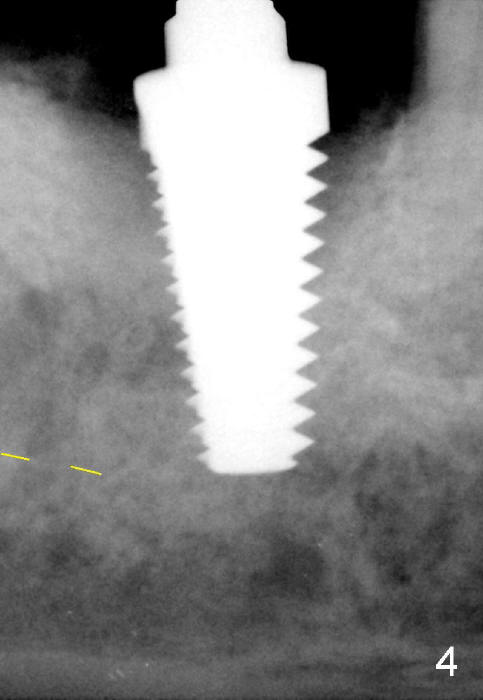
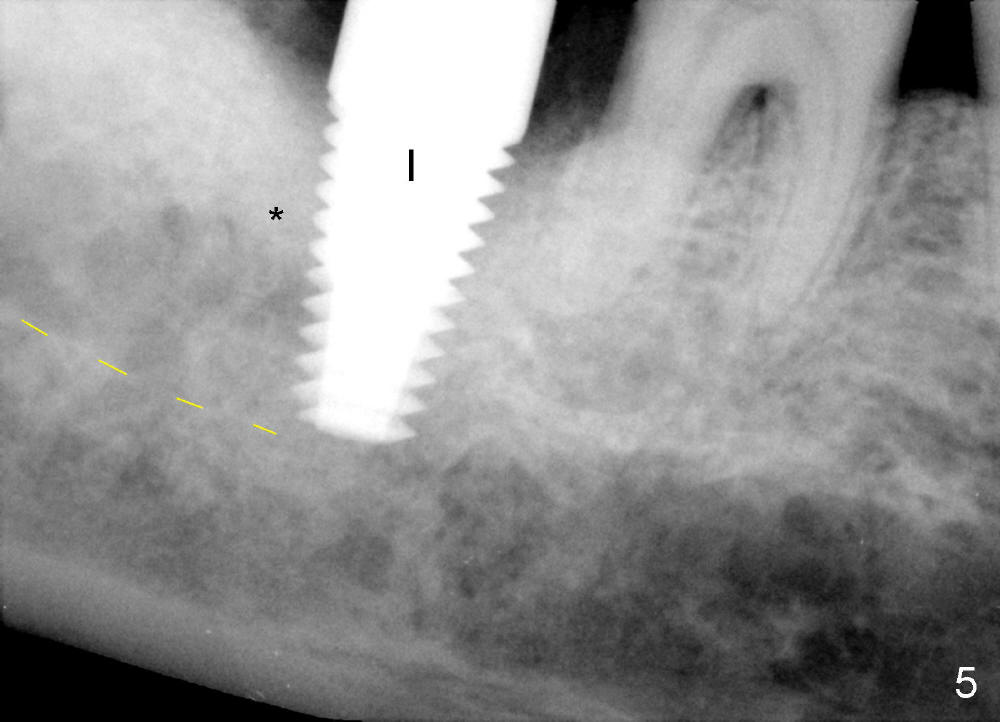
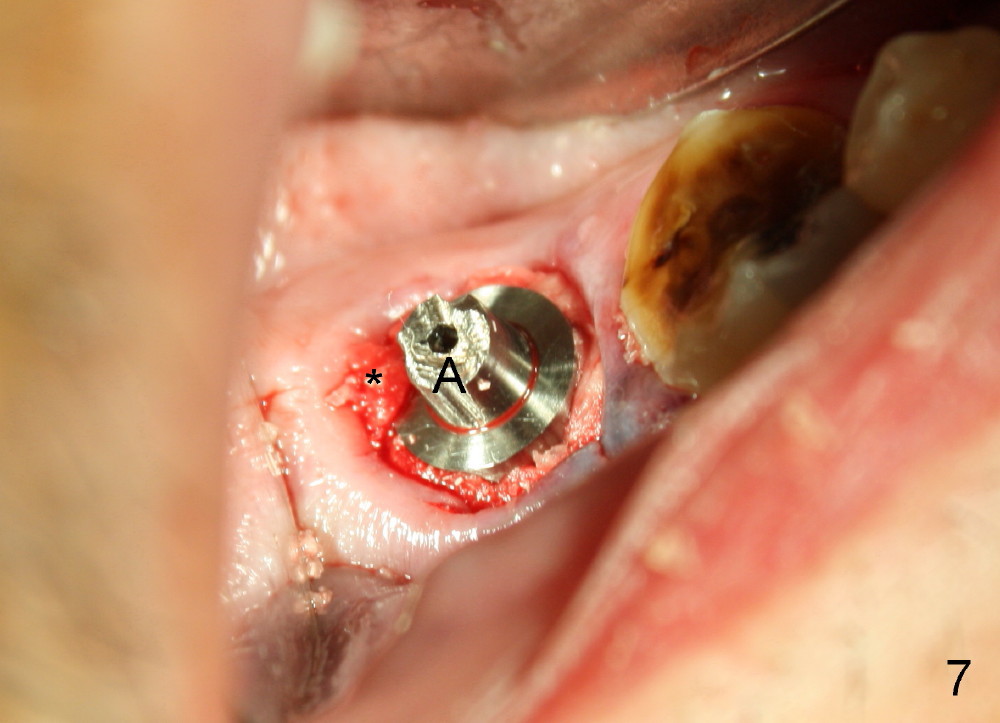
The most challenging immediate implant involves the lower 2nd molar with severe infection (Fig.1,2 *). Amoxicillin is taken 1 day prior to surgery. Six hundred mg of Advil is taken immediately preop. Infiltration anesthesia with Lidocaine 34 mg, Articaine 68 mg, Marcaine 9 mg, Epinephrine 43 mcg is not sufficient for extraction of the molar with mobility III. Gentle intraligamental injection has to be supplemented with Lidocaine 34 mg, Epinephrine 17 mcg. Even so, the patient feels some pain during debridement of the socket. A dummy implant (7x11 mm) is placed in the socket for depth control and design (Fig.3). Block anesthesia has to be administered with Lidocaine 34 mg, Epinephrine 17 mcg before using 2 mm pilot drill at 17 mm deep. The osteotomy is created by using 2.5-3.5 mm reamers at the same depth, followed by taps until 7x17 mm with stability (Fig.4). A small portion of allograft + Osteogen is placed in the distal apical socket (Fig.5 *) before placement of 7x17 mm implant (I). More bone graft is placed around the implant coronally (Fig.6 *). Collagen dressing is placed to close the gap (Fig.7 *). A short abutment (A) is placed before perio dressing is applied.
When local anesthesia subsides, there is moderate pain, control by Advil and Medrol Dose Pak. Luckily there is no paresthesia reported. In fact this is not the case.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 09/16/2014, last revision 09/21/2014