







|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
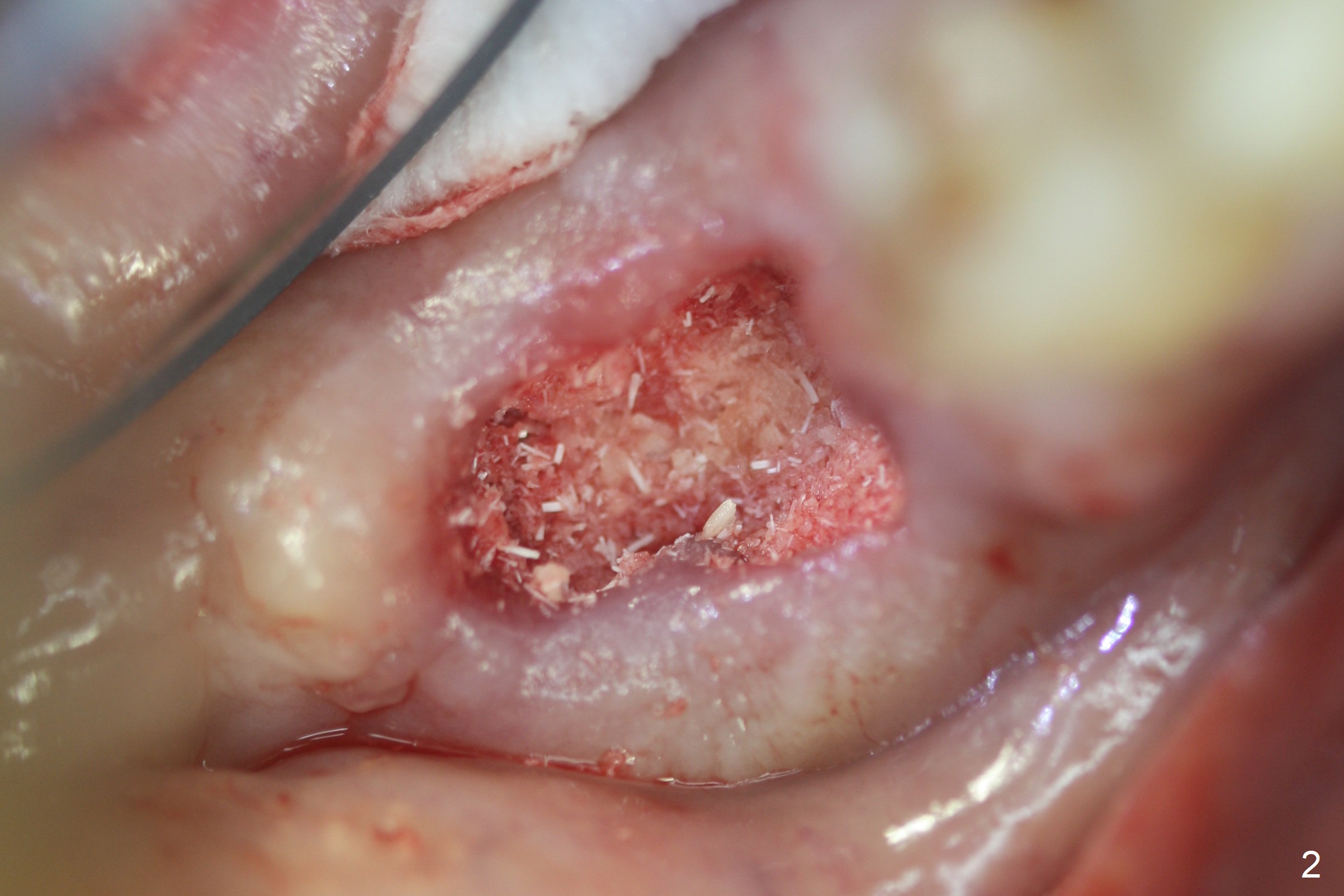
Socket Preservation Instead of Implant
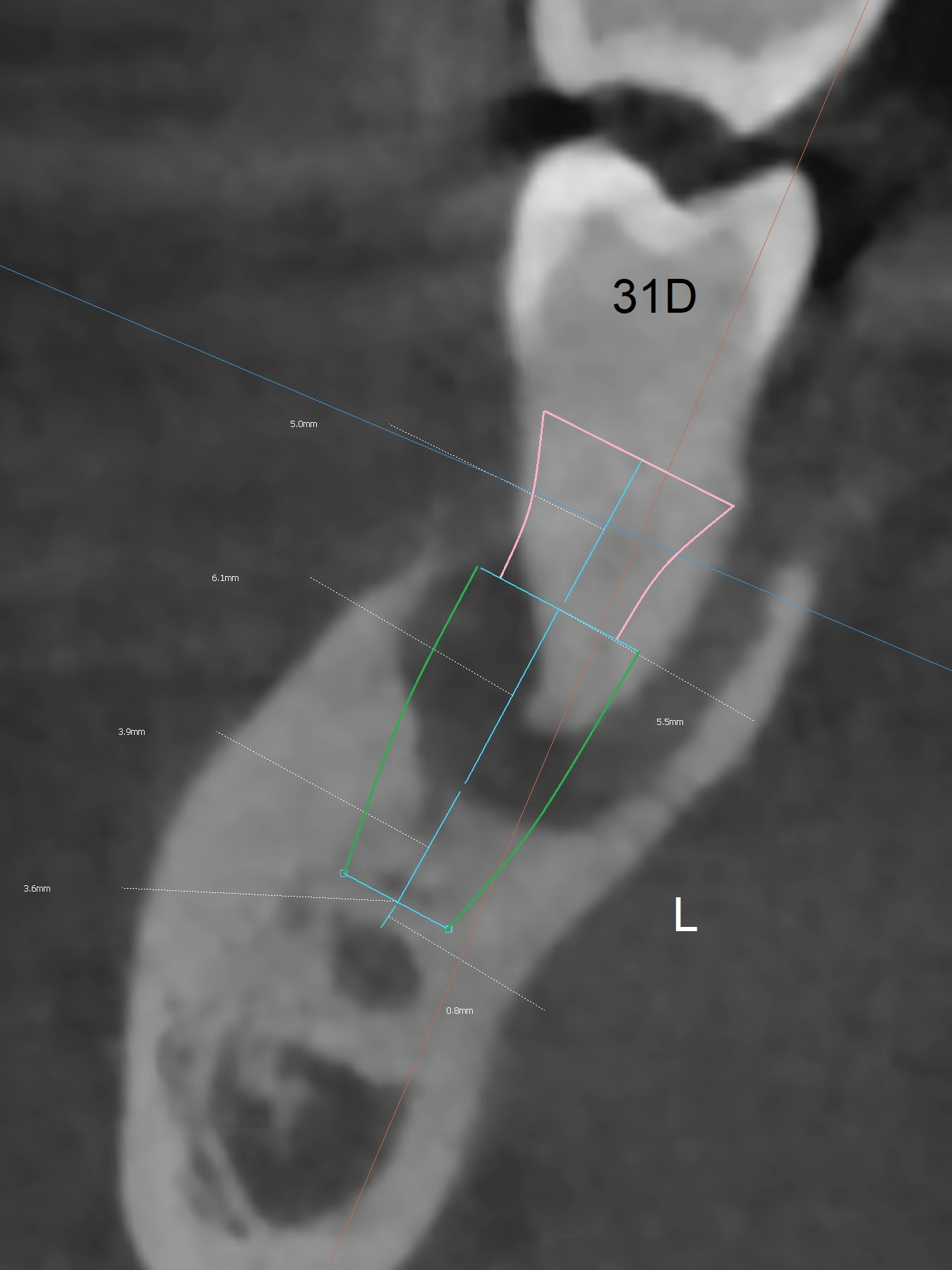
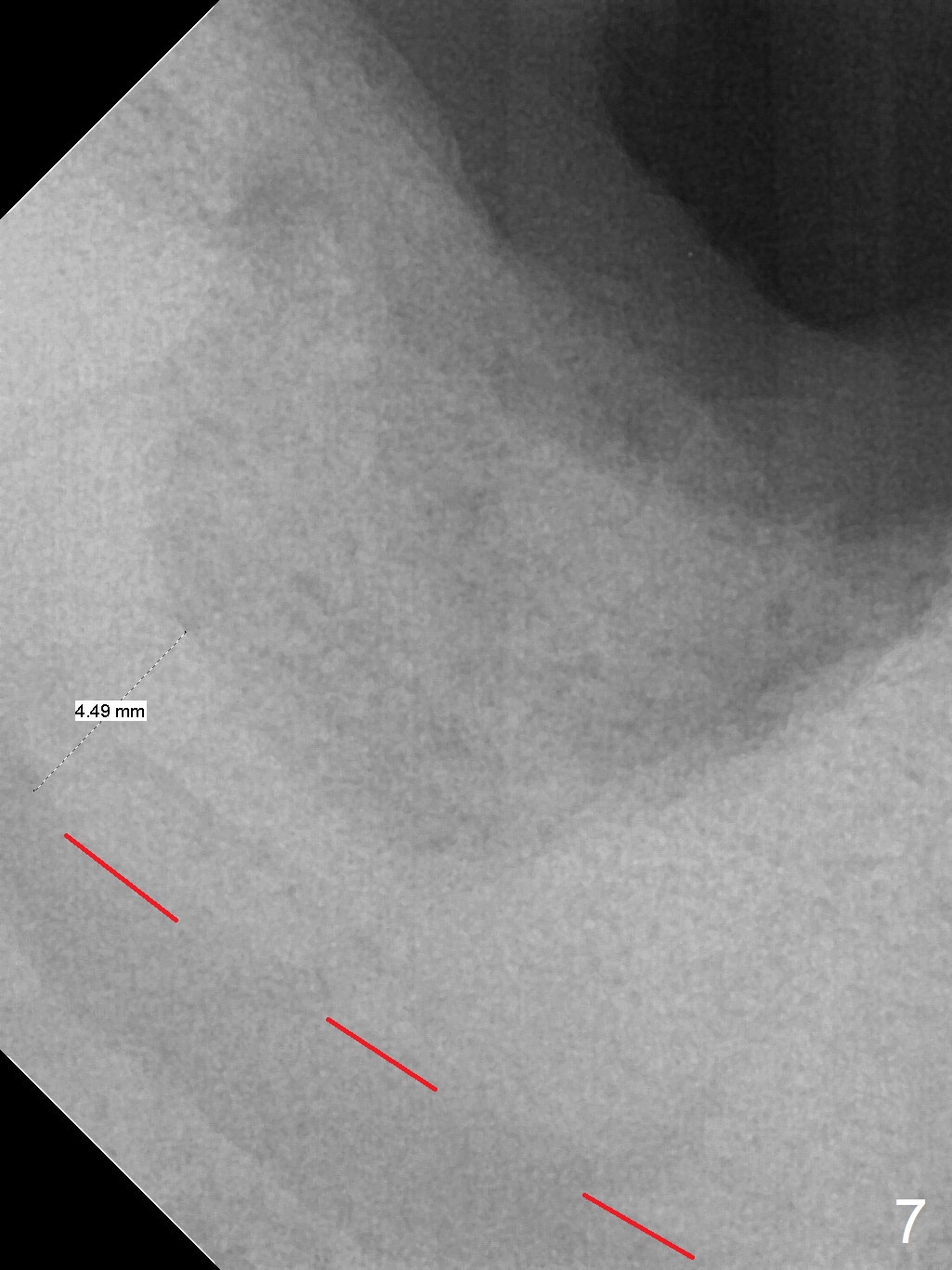
Extraction of the mobile tooth #31 (Fig.1) and debridement of the large socket are not difficult. But making osteotomy buccally does not seem to be easy. It will be difficult to restore. Instead, socket preservation is accomplished by filling the socket with approximately 1.5 cc of Mineralized Cortical/Cancellous allograft until the crest (Fig.2,5). The socket opening is closed by insertion of 4 pieces of PRF membranes (Fig.3) and 4-0 Chromic gut sutures (Fig.4). In the end of surgery, it appears that osteotomy in the center of the socket could be a better approach. Postop re-analysis of CT (Fig.6) and PA (Fig.7) shows that there is 3.9 mm of the native bone to support a 5.5x10 mm implant. Sinus Lift Master Kit should be used with 2 mm initial drill and 2.8 and 3.6 mm round drills with 4 mm stopper.
The socket heals 3 months postop (Fig.8,11). There is vertical loss of the ridge at #31 (Fig.9,10). The implant placed at #31 will be shorter than that at #30 (Fig.12). The patient will return for implant placement 4 months postop.
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
IBS,
Armaments
Xin Wei, DDS, PhD, MS 1st edition 08/09/2017, last revision 04/15/2020