

|
|
|
|
|
|
|
|
|
|
|
|
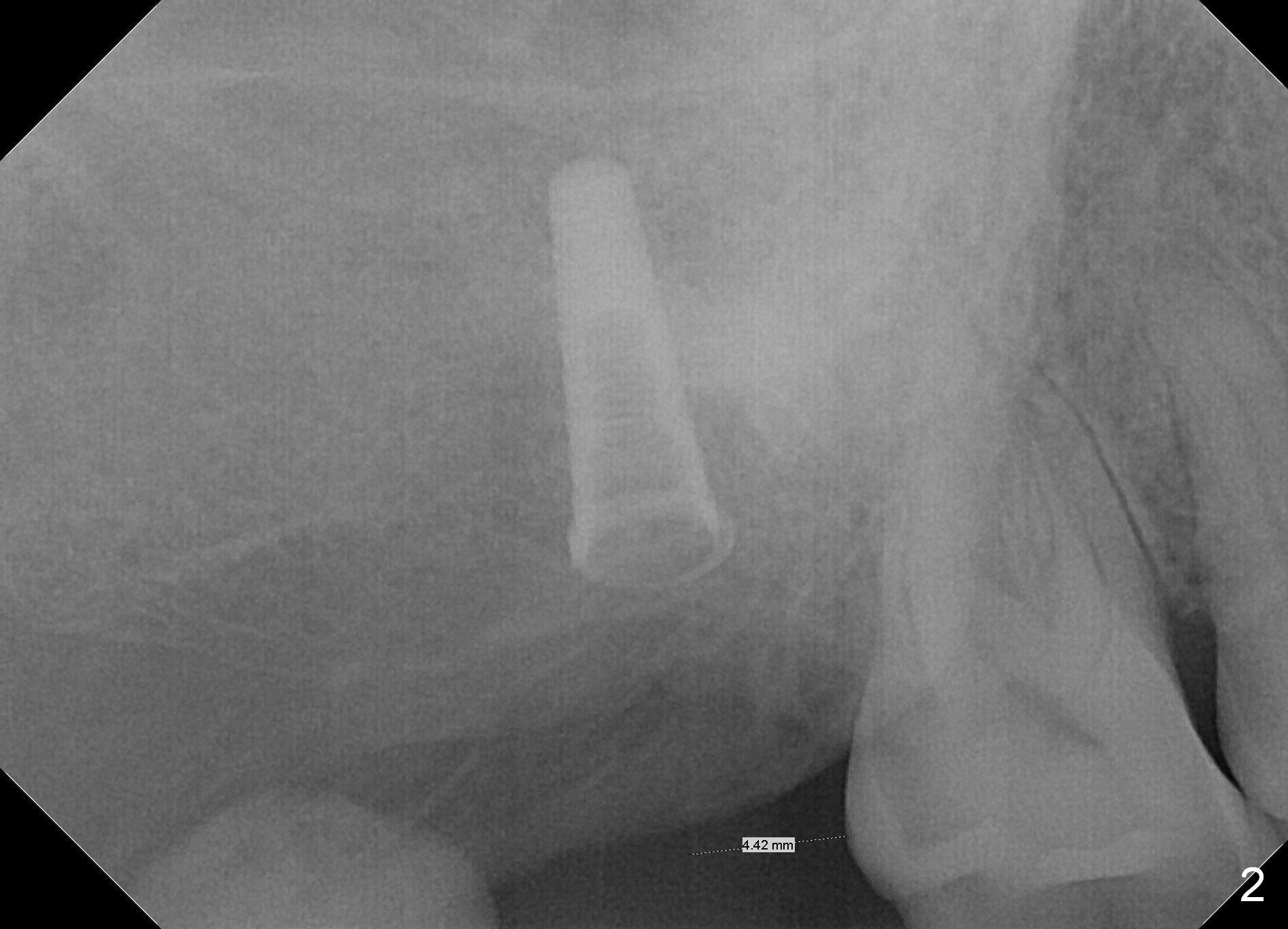
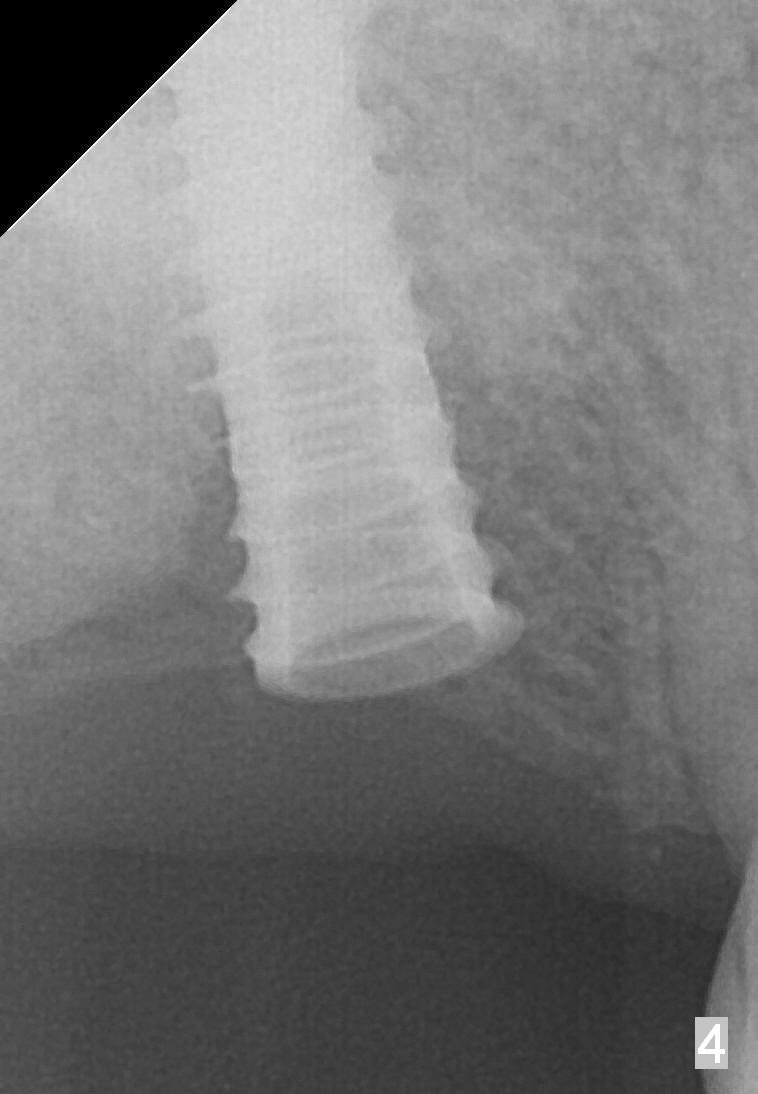
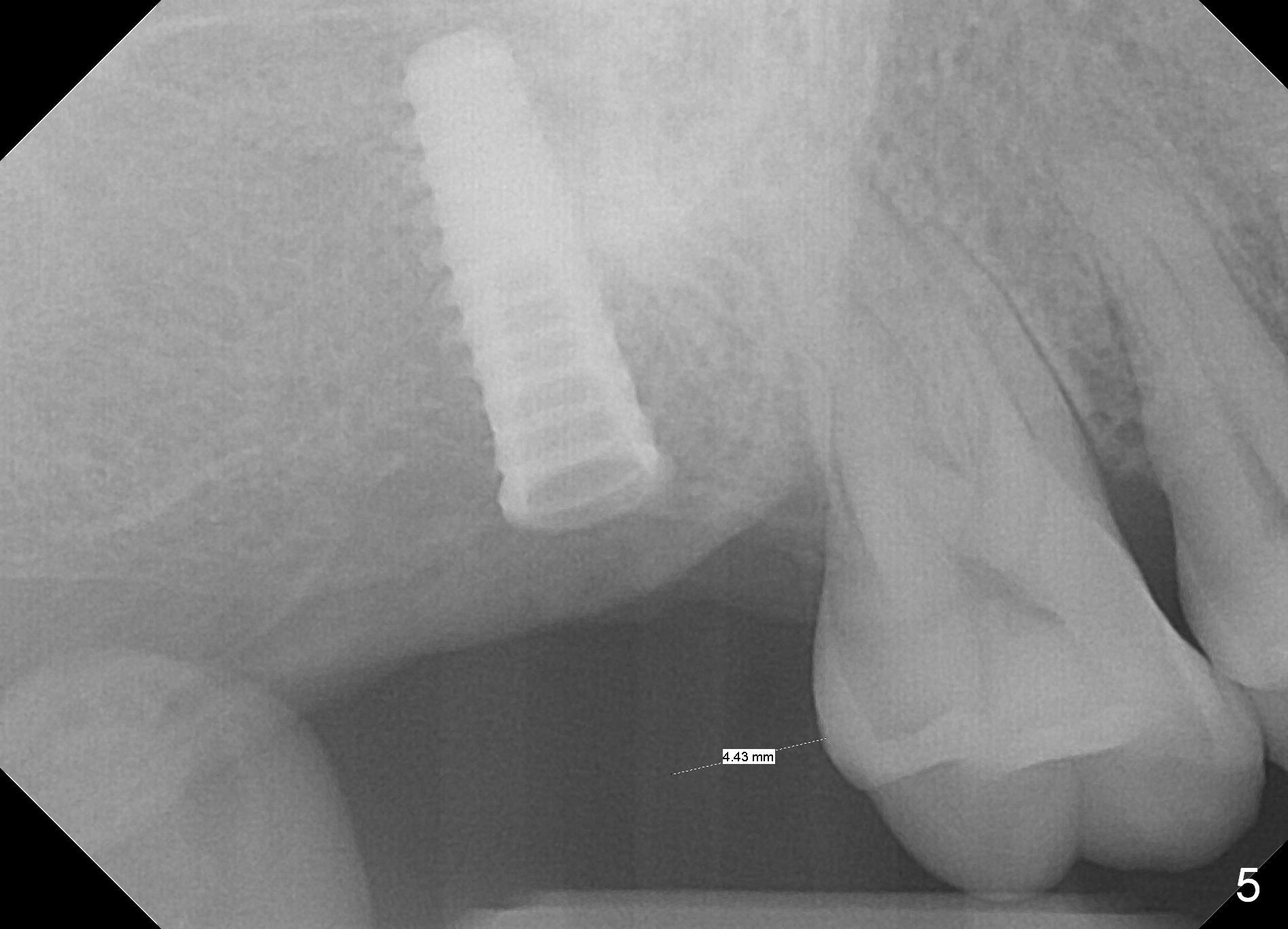
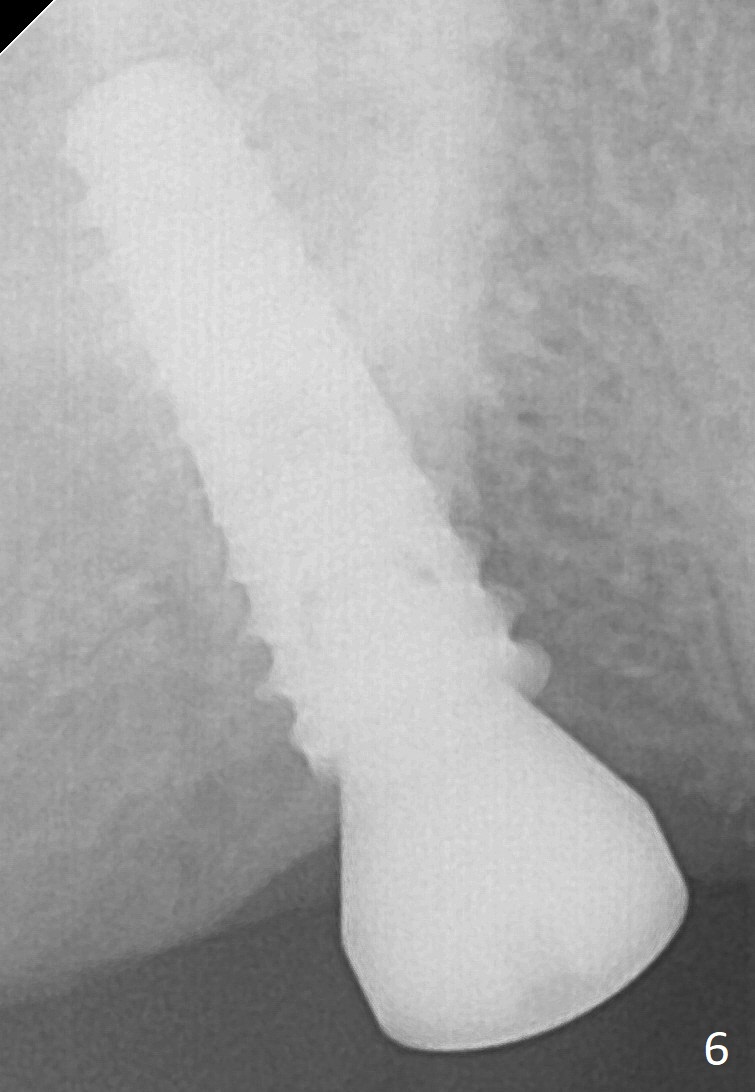
Control Osteotomy Position of the 2nd Molar
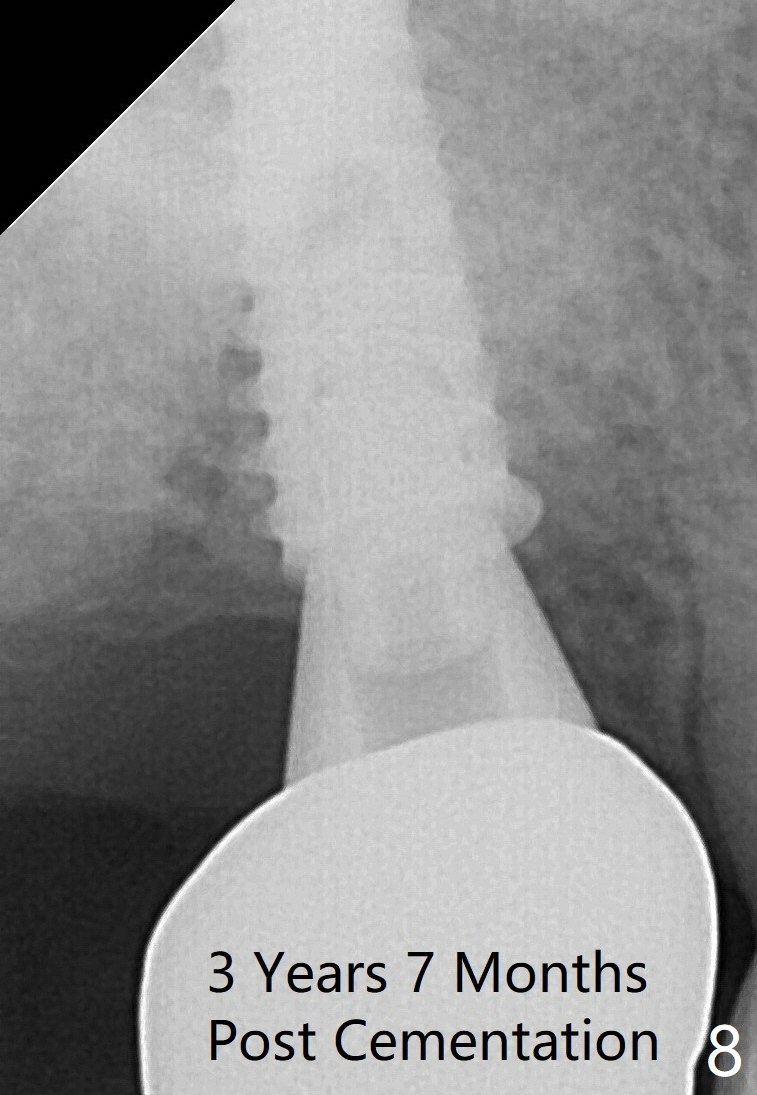
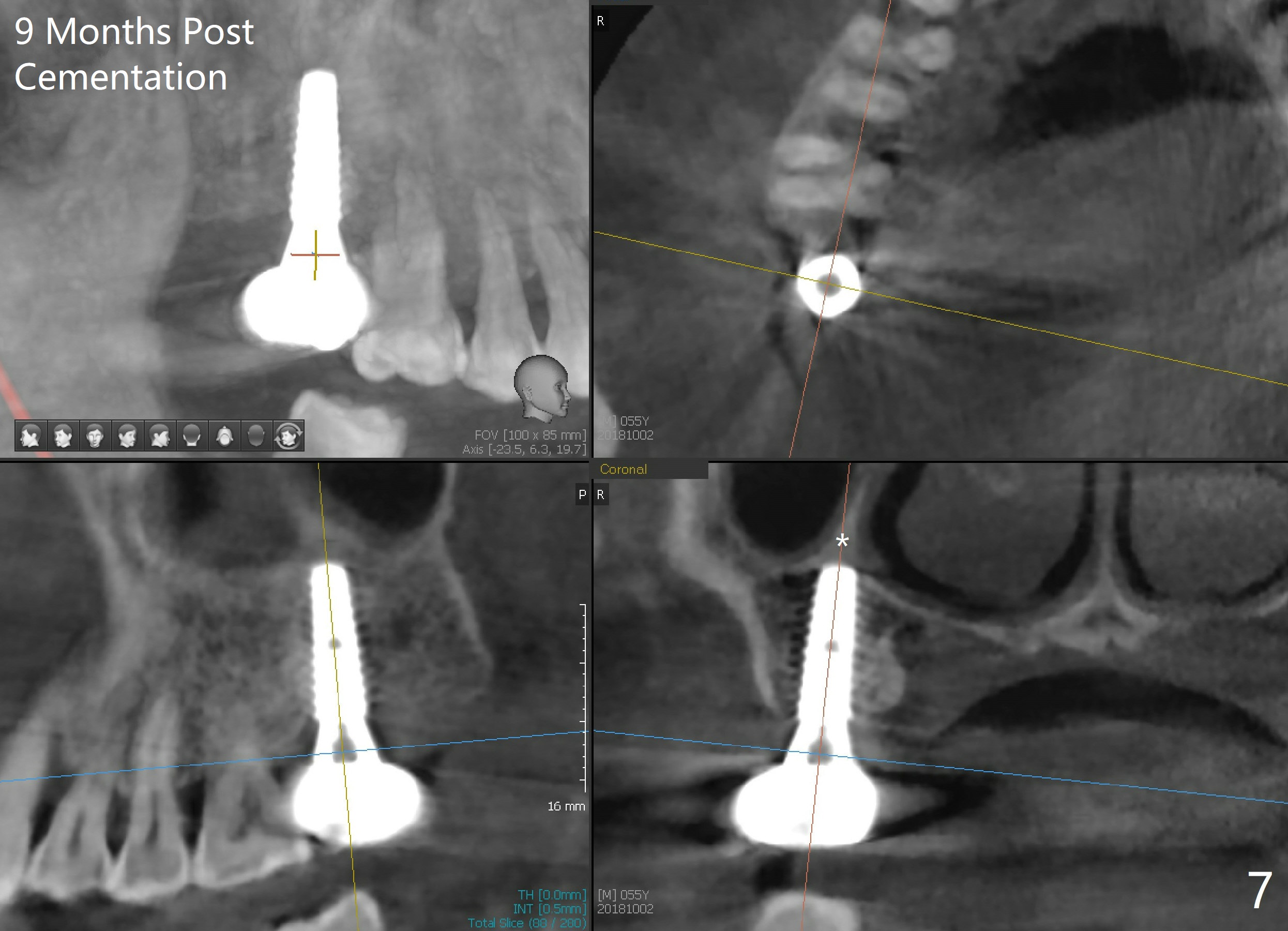
The edentulous ridge at the site of #2 is wide. Magic split is used to gain access, test bone density and start osteotomy for 9 mm (gingival level). A 1.6 mm drill is used to extend the osteotomy for depth of 13 mm. The osteotomy position and trajectory is confirmed with a parallel pin (Fig.1), which is ideal. The remaining osteotomy is finished with Magic Expanders from 3 to 4.3 mm for 15 mm. The trajectory is confirmed again with insertion of a 4.5x11 mm dummy implant at the depth of 15 mm (Fig.2). When a definitive IBS implant (5x13 mm) is placed with insertion torque >45 Ncm, the distal coronal end is not subcrestal (Fig.3-5). As the implant is placed deeper, it started to lose primary stability. When a pair abutment is placed, it keeps turning. Finally a healing abutment (6x3 mm) is placed unstable. In brief, taking several X-ray films help control osteotomy and implant position and trajectory. The implant is unstable 7 months postop (Fig.6). With local anesthesia, the implant is placed deeper by 1 mm with apparent increase in torque and a 6x4 healing abutment placed. The implant is stable 11 months postop. With 5.5x4(4) mm abutment placed, impression is taken. PA and BW will be taken after cementation of the crown. There is no bone loss 9 months post cementation (Fig.7). Return to Upper Molar Immediate Implant, 18-20, 29,30 Xin Wei, DDS, PhD, MS 1st edition 01/09/2017, last revision 08/15/2021