%202.jpg)
.jpg)
,%206%20m%20postop.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
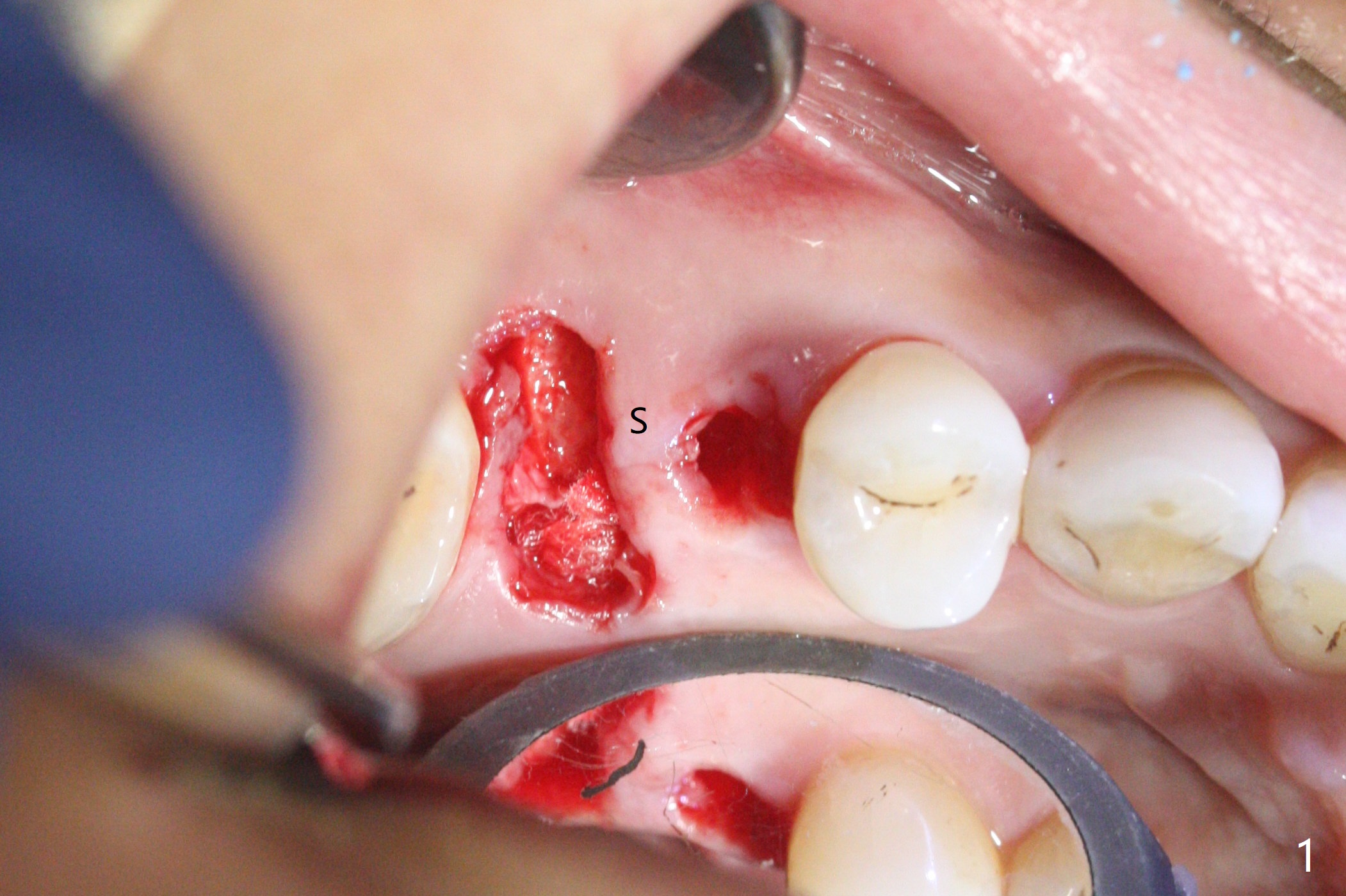
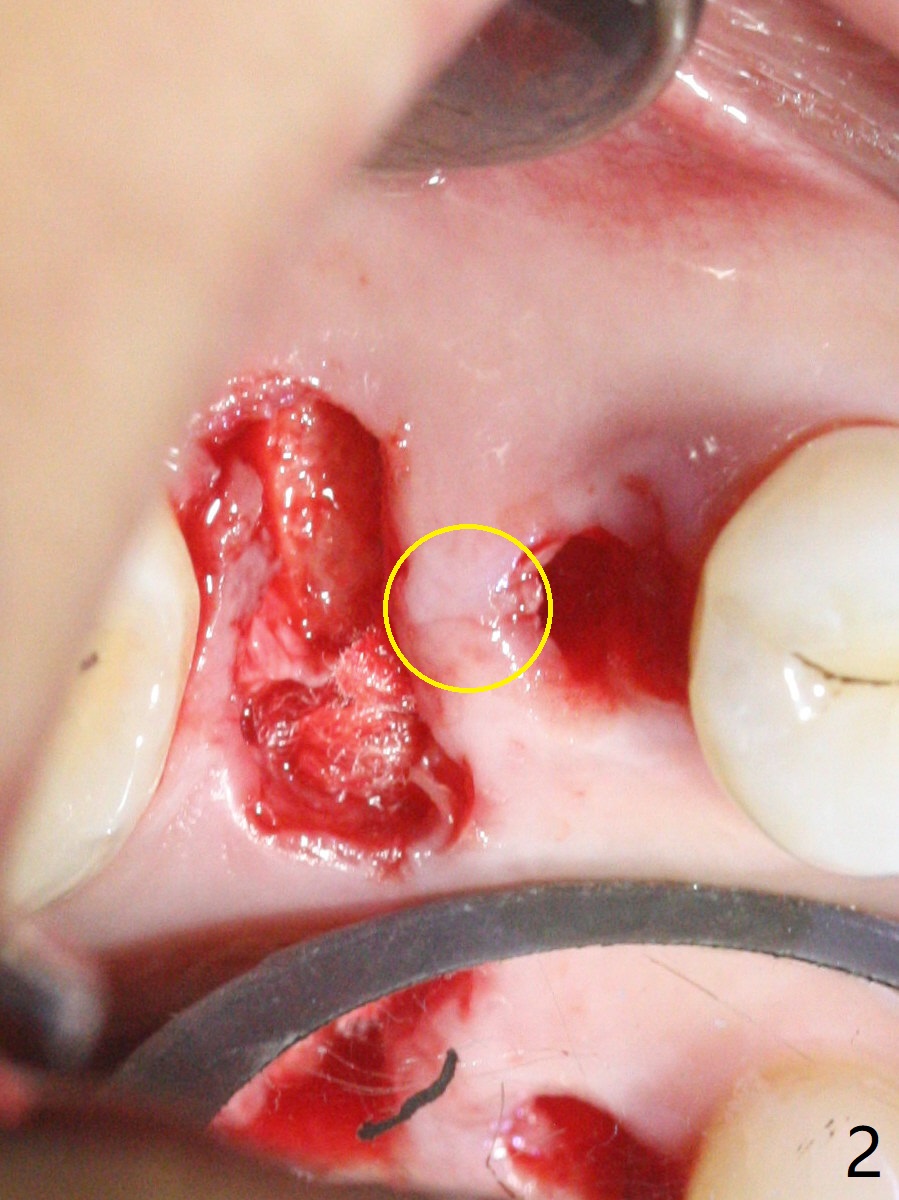
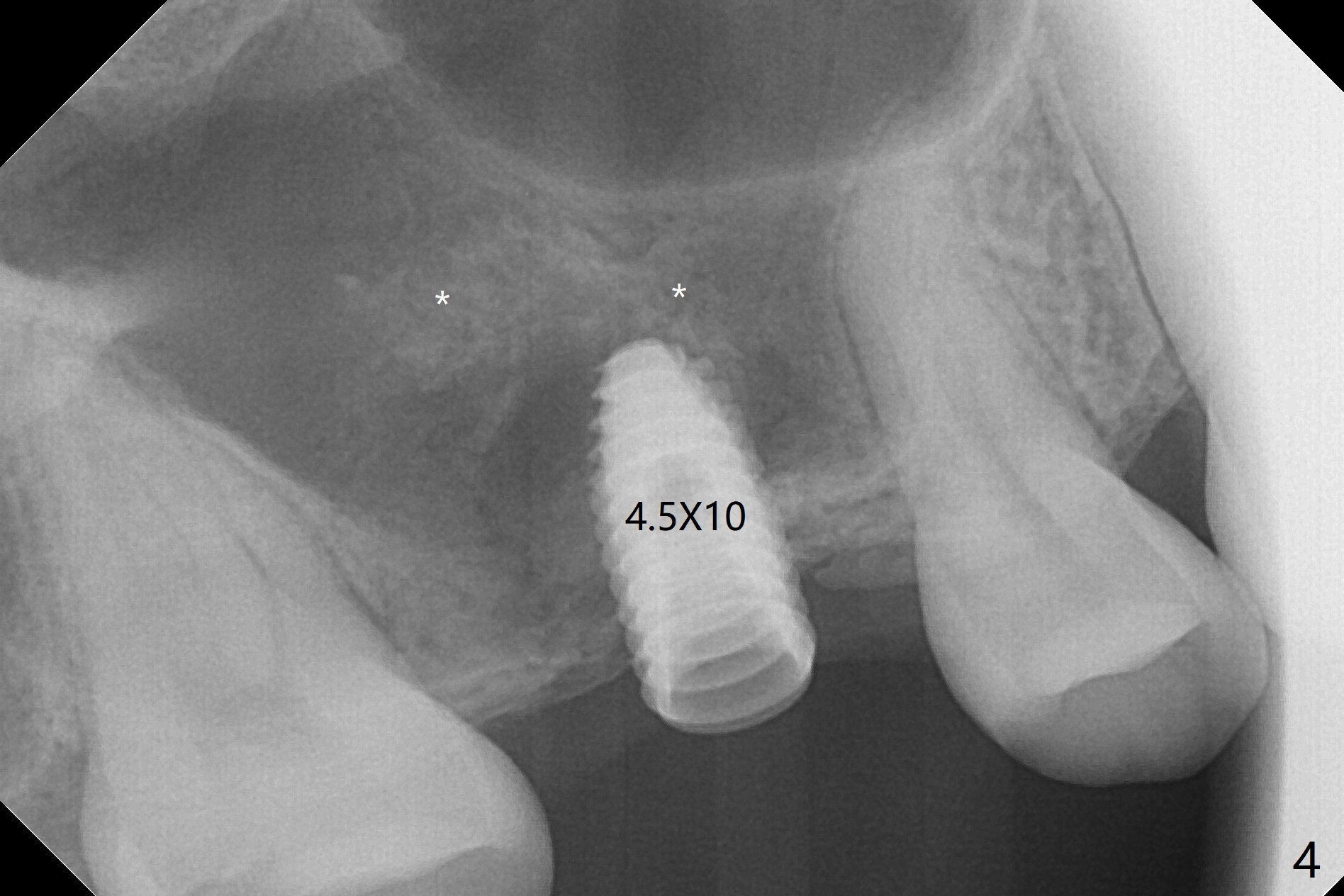
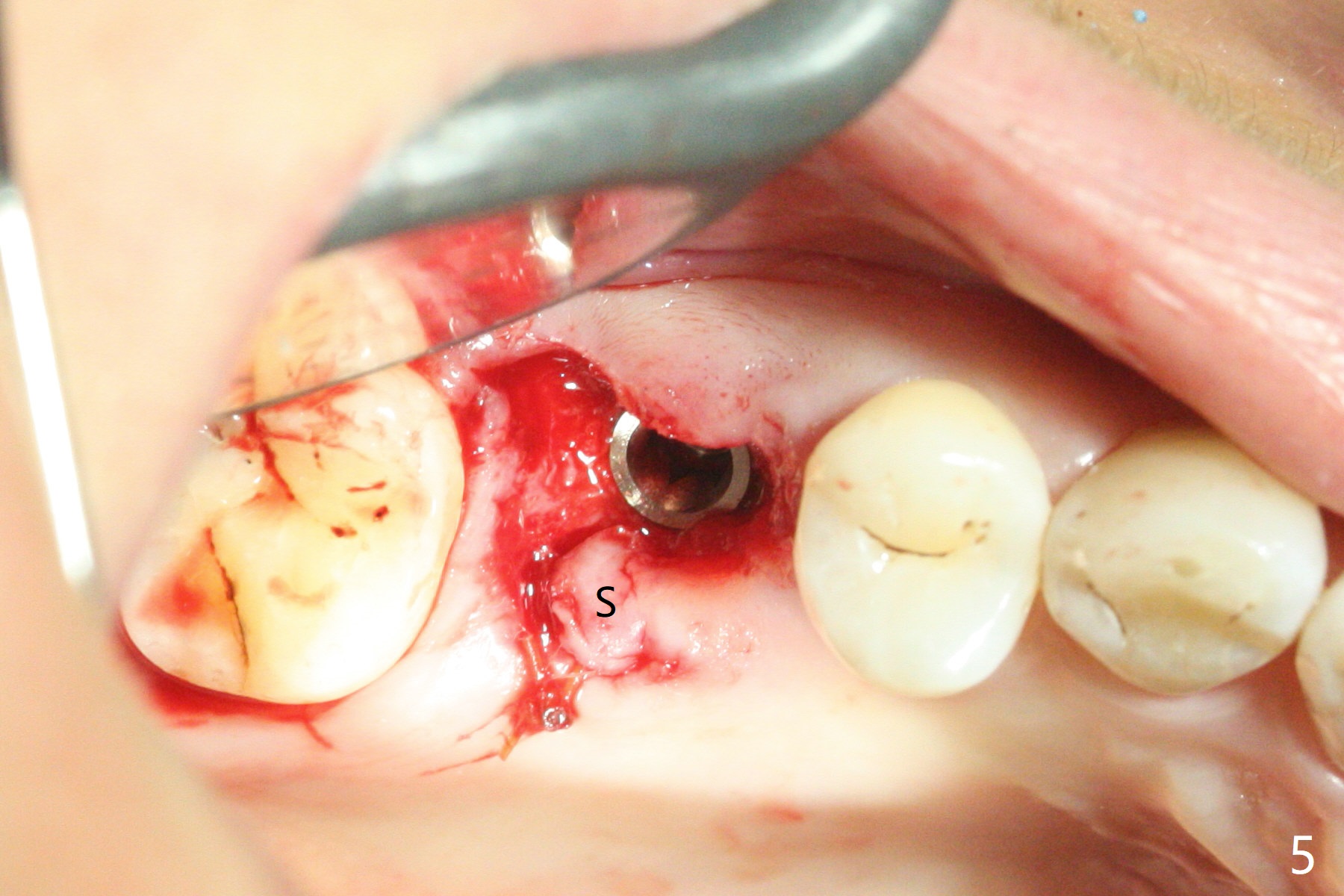
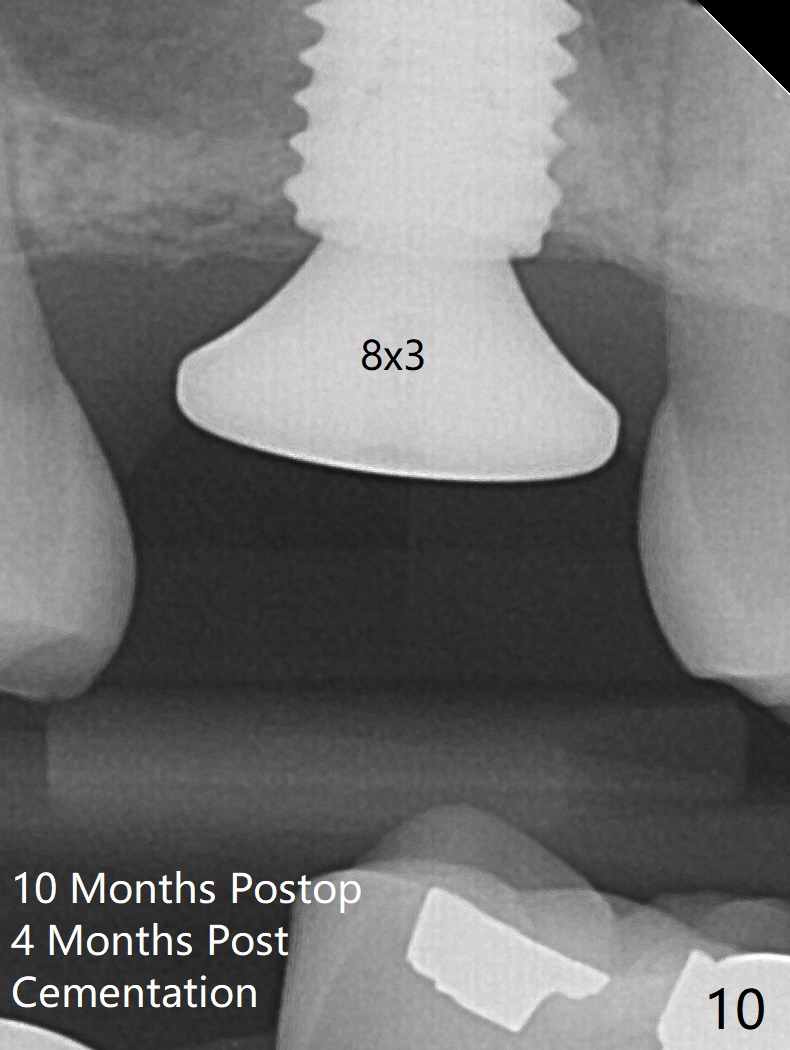
When the residual roots of the tooth #3 are removed, there is a gingival band over the septum (Fig.1 S). Osteotomy (Fig.2 yellow circle) would tear it off. To save the soft tissue, the buccal attachment is severed (Fig.3 black line), the flap is rotated palatal (Fig.3 curved arrow) and sutured in place (Fig.5 S). After sinus floor breakdown (use of sinus drill for 16 mm) and use of membrane lifter/water, two pieces of PRF membrane are inserted. The membrane is so slippery that it is easy to enter the sinus for further sinus membrane lift and later allograft placement (Fig.4 *). A 4.5x10 mm dummy implant is placed with high torque after 4x7.3 mm drill with 3 mm stopper so that 4.5x7.3 mm drill with 1 mm stopper is used before placement of a 5x8.5 mm final implant with ~ 35 Ncm (Fig.5-7). The patient reports anterior sinus wall tenderness with right nasal discharge a few days postop. The provisional has mobility without tenderness 1 week postop. It appears that the sinus membrane has been involved, which is quickly repaired probably by PRF. There is no pain when a 5.2x4(2) mm cemented abutment is torqued at 30-35 Ncm before impression (Fig.8). The surrounding soft tissue is healthy. But the patient feels pain when the crown is cemented 2-3 weeks later. Occlusal adjustment alleviates the discomfort. The latter persists 4 months post cementation (Fig.9). The crown/abutment is replaced with a healing abutment (Fig.10).
Return to Upper Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Trajectory II, 31 Xin Wei, DDS, PhD, MS 1st edition 07/26/2019, last revision 06/01/2020