

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
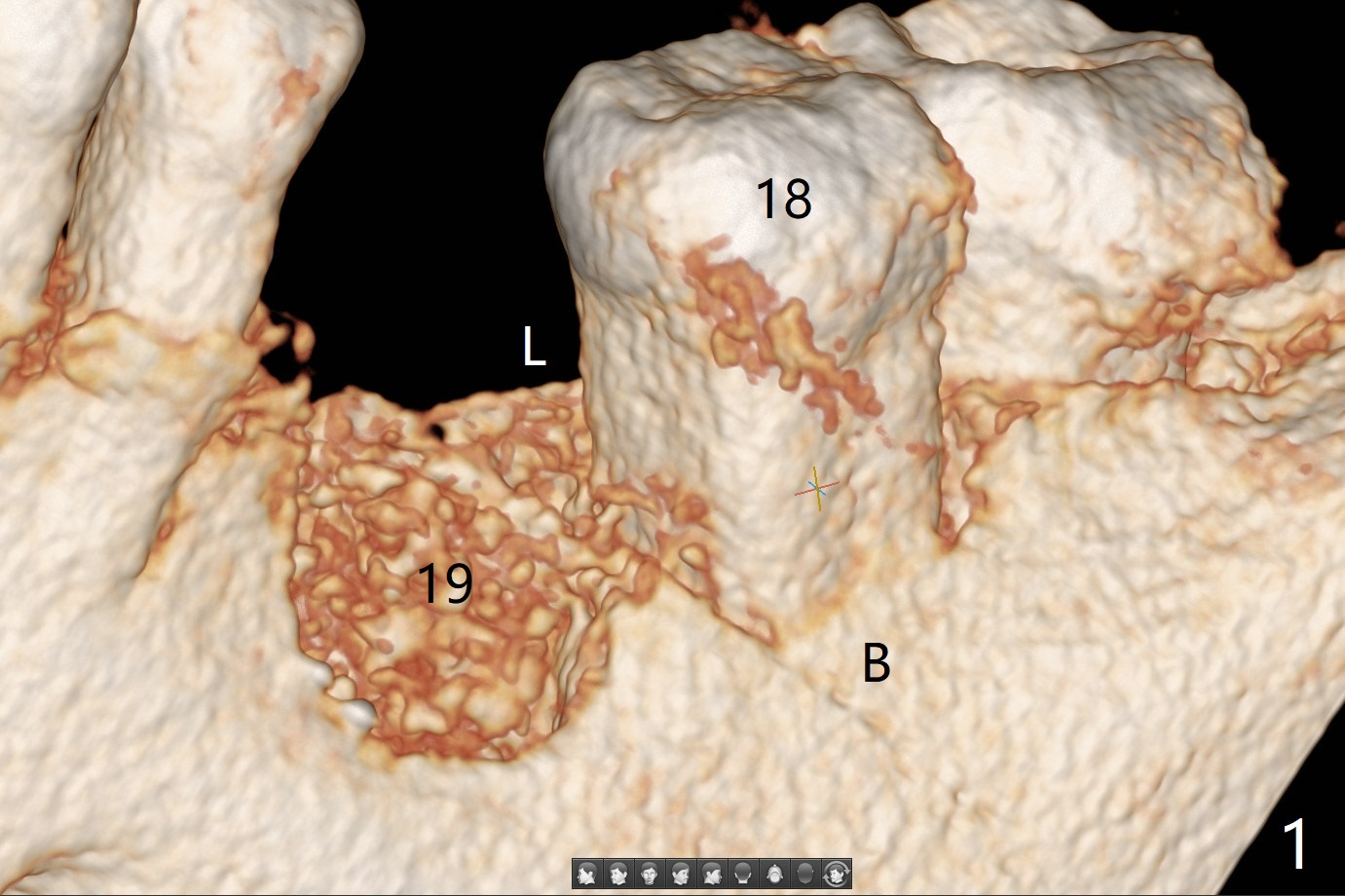
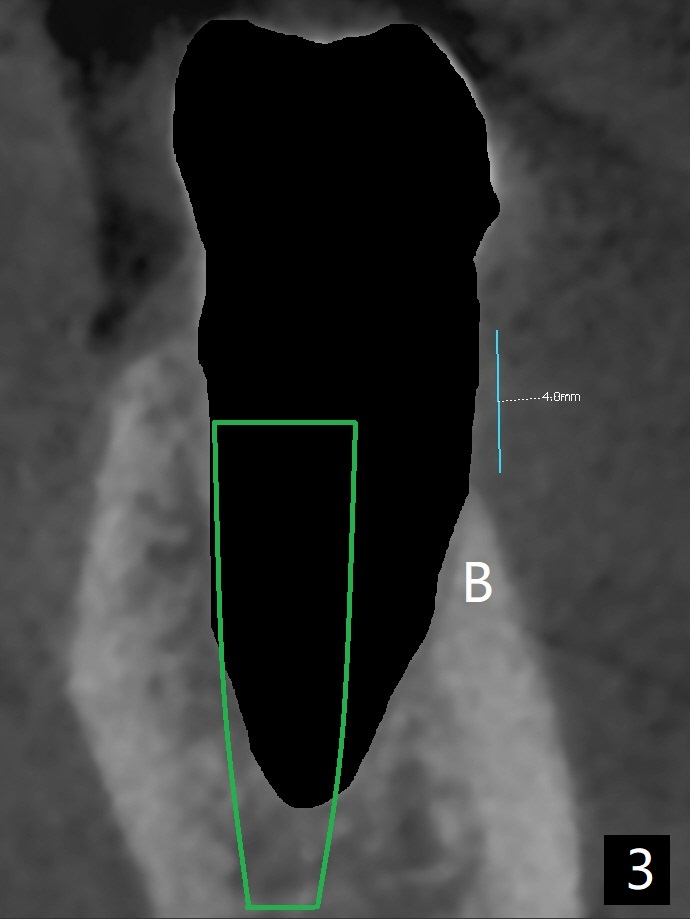
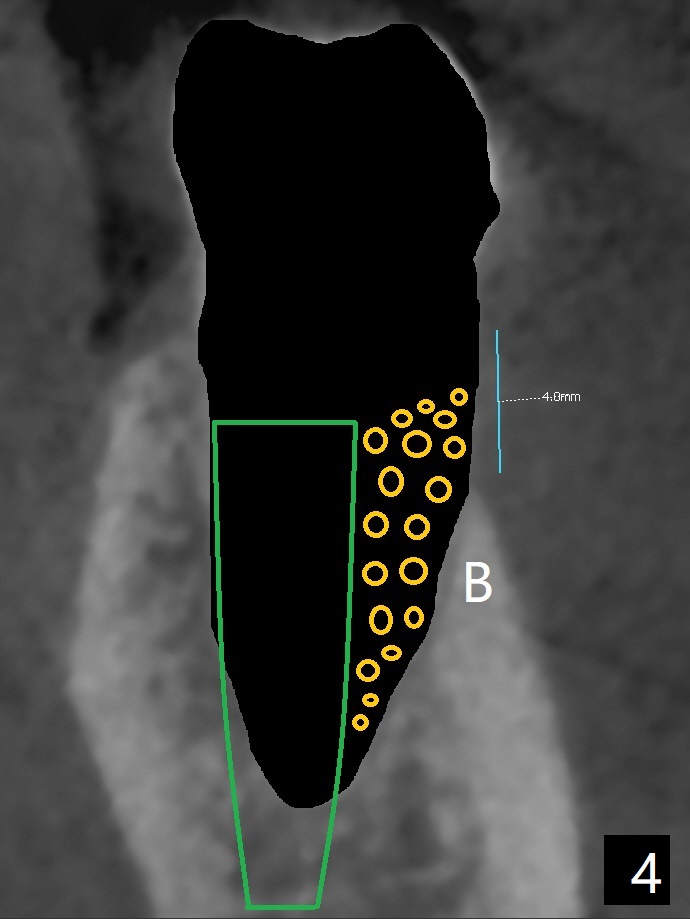
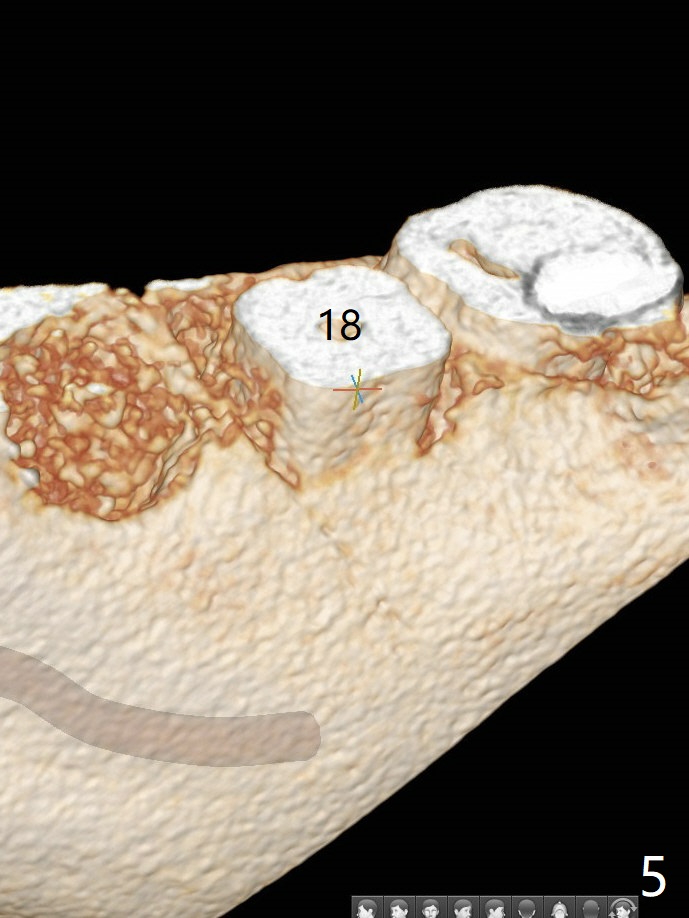
Necessity of Molar Socket Shield
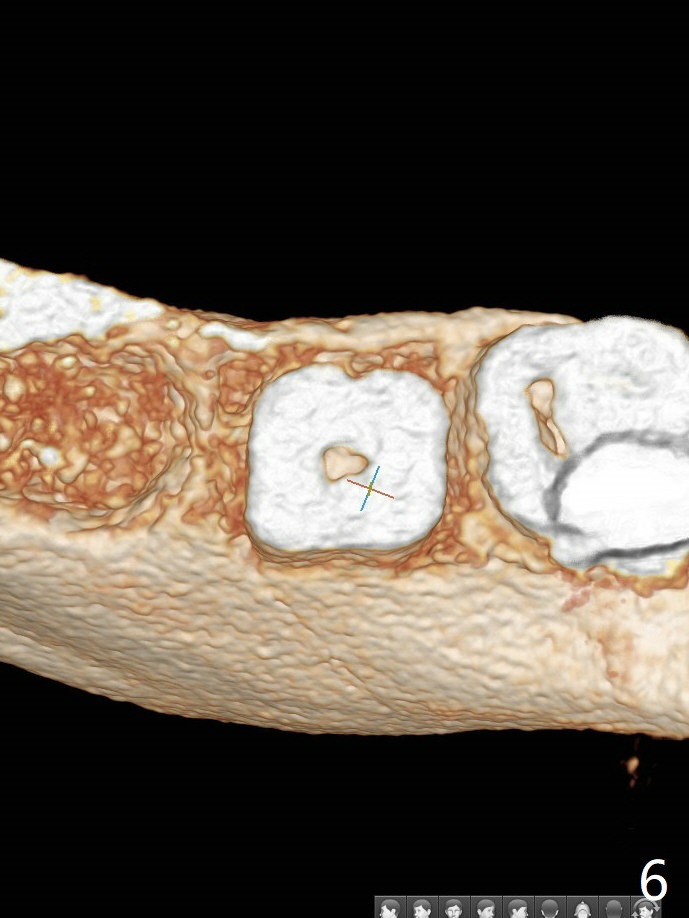
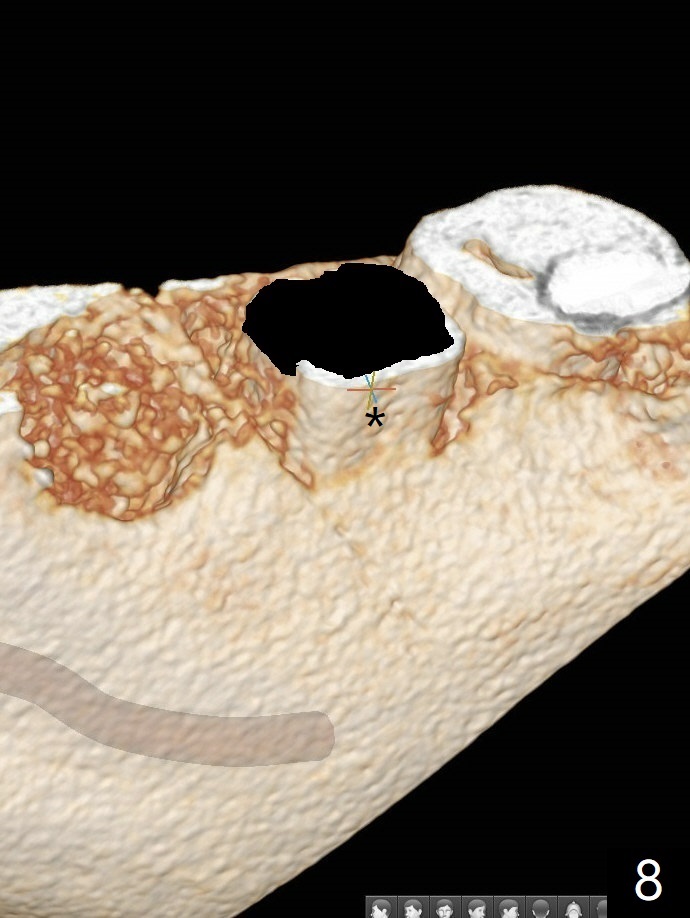
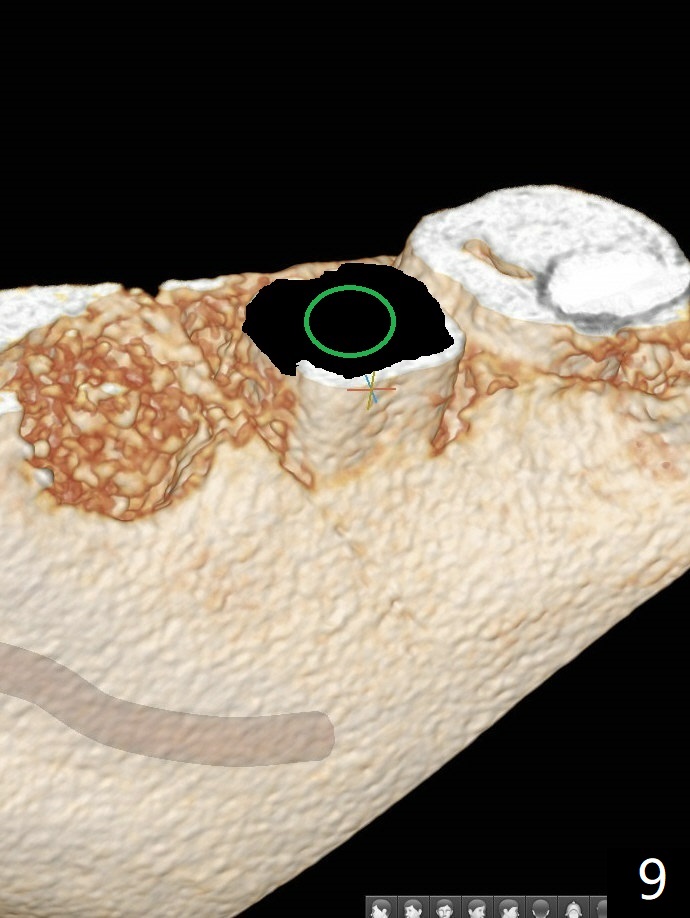
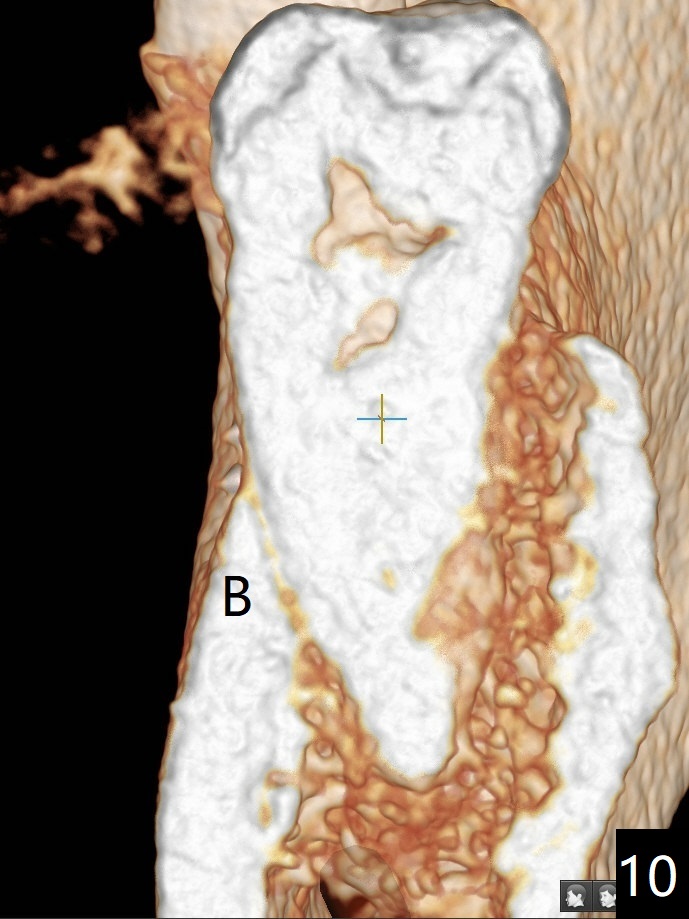
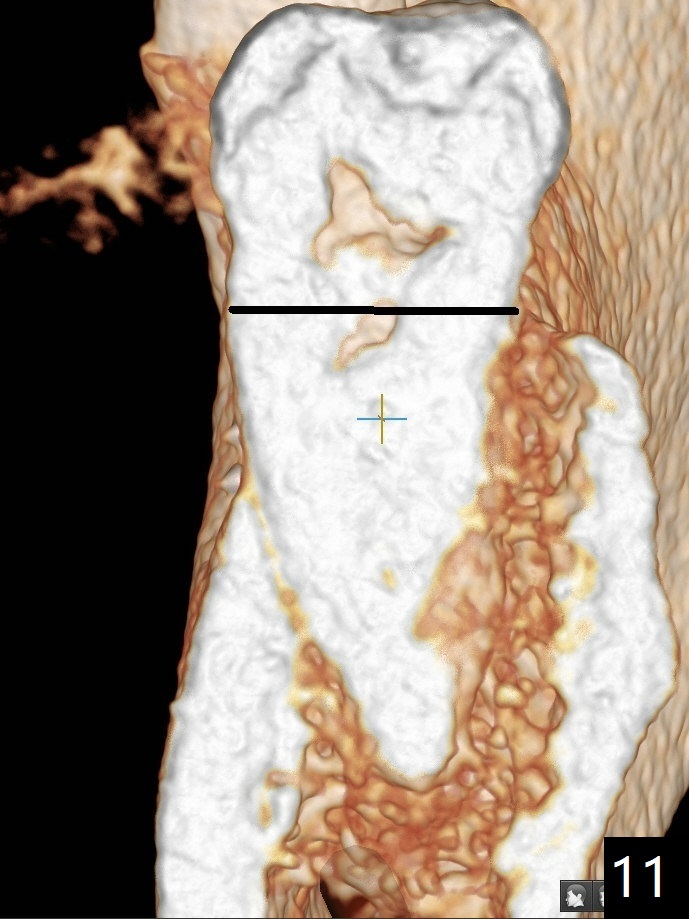
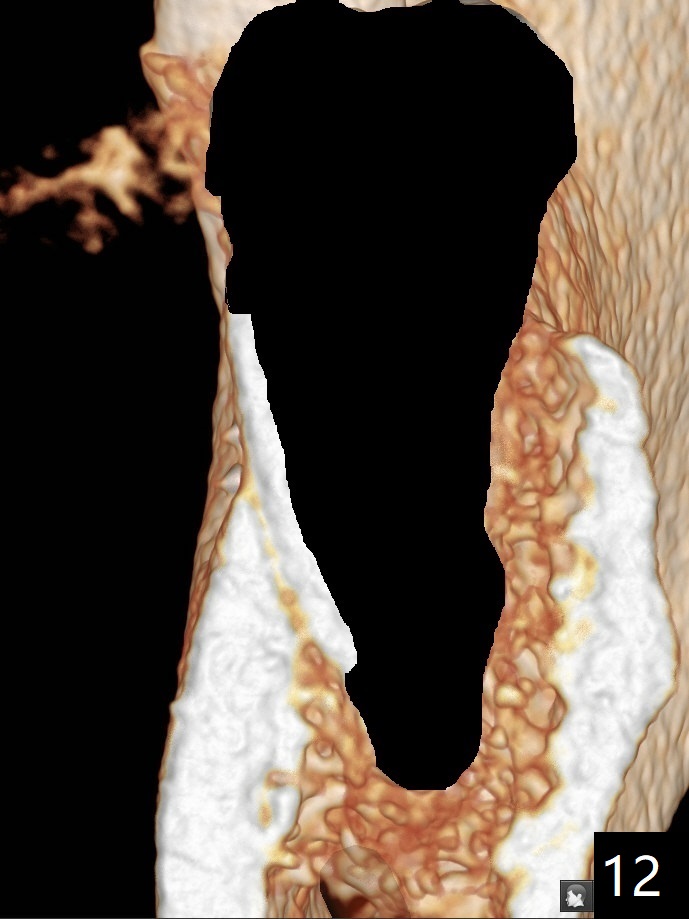
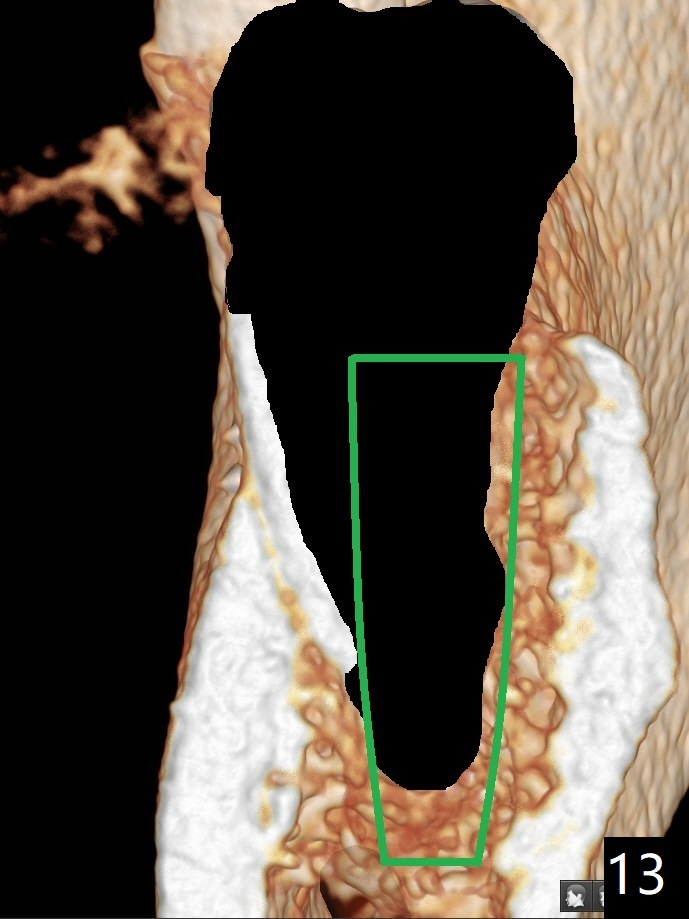
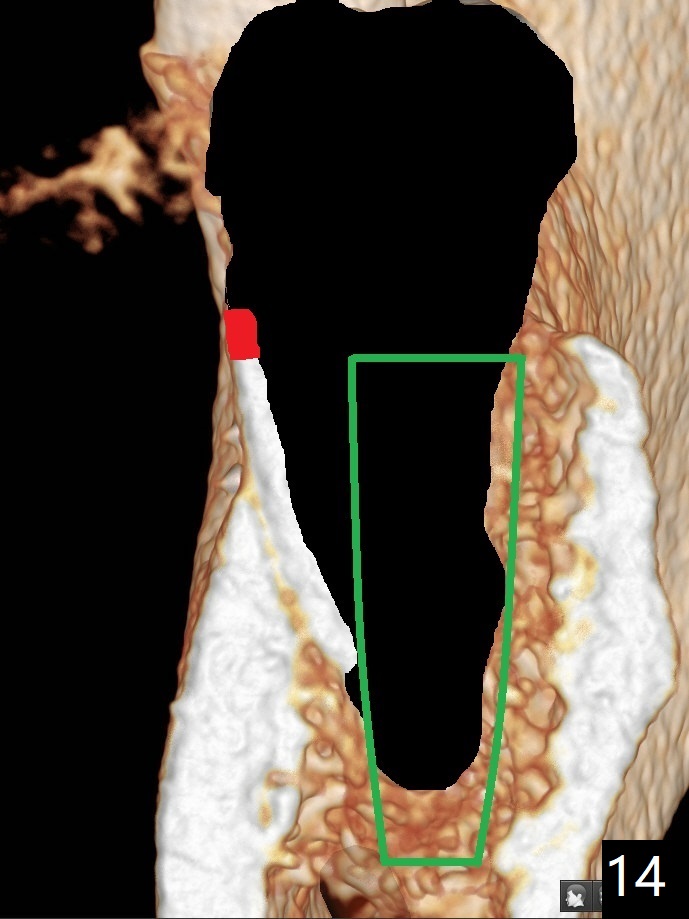
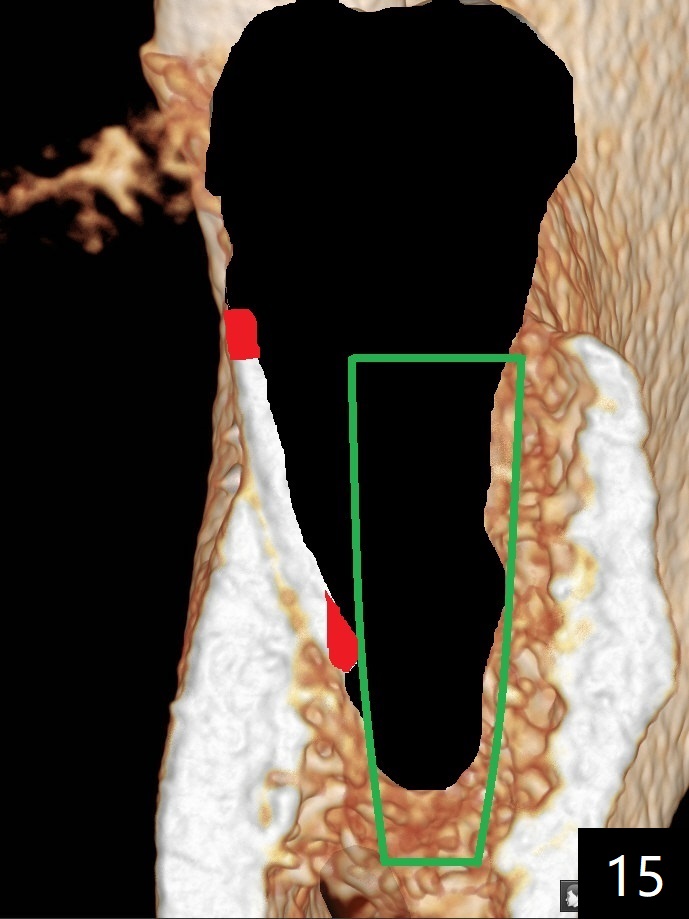
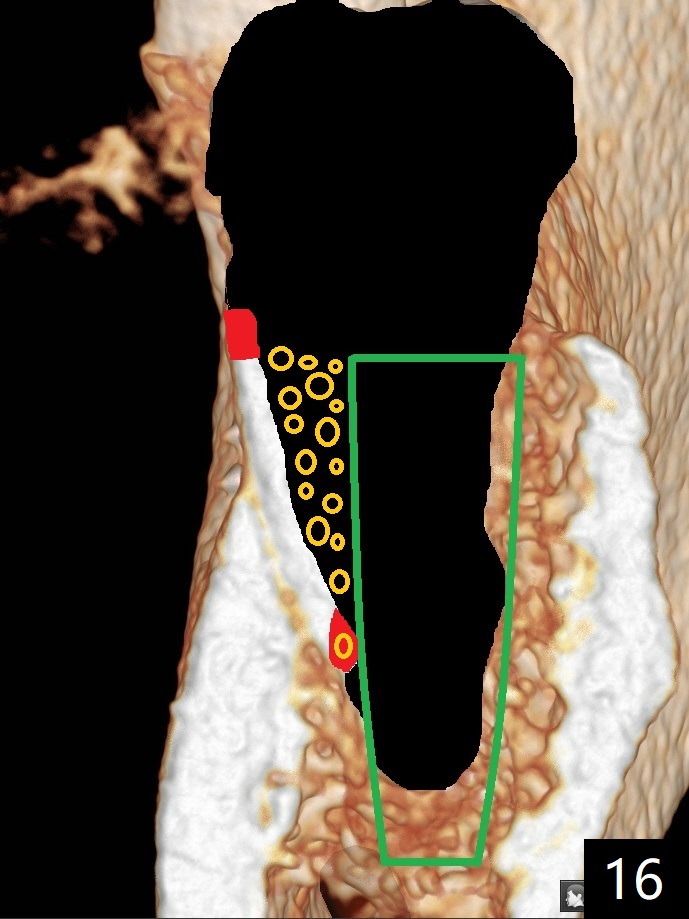
Severe buccal plate atrophy occurs after #19 extraction with socket preservation (Fig.1). How to prevent it? In fact the buccal crest at #18 (Fig.1,2 B) is inherently lower than the lingual one (L) by ~ 4 mm before extraction. After extraction (Fig.3 black), an implant (green) is placed 2 mm subcrestal lingual, while supracrestal buccal 2 mm. With bone graft (Fig.4 orange circles), there is potential of buccal thread exposure postop. Can we use the remaining buccal root (socket shield) as a substitute buccal plate (hard tissue instead of the soft one (gingiva)) to keep the bone graft in place? For socket shield, section the crown (Fig.5.6) and remove the majority of the root lingually (Fig.7). The remaining buccal root with overlying gingiva (Fig.8 *) is more capable of holding bone graft in place than the gingiva alone. The immediate implant (Fig.9 green) can be placed equigingival lingually without too much risk of buccal implant thread exposure. Fig.10 is a CT coronal section; it shows that the buccal crest is thin and low (B). For socket shield, section the tooth horizontally (Fig.11 black line) and remove the majority of the root (Fig.12 black area). The immediate implant does not have to be placed lingual (Fig.13, as compared to Fig.3). The coronal end of the shield could be trimmed slightly subgingival (Fig.14 red). Approximation of the shield with the implant should not be an issue, but it could be trimmed (Fig.15 red). With bone graft (Fig.16 orange circles), the implant will be most likely osteointegrated.
Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table) Trajectory II Clindamycin Metronidazole No Antibiotic Shield Xin Wei, DDS, PhD, MS 1st edition 10/13/2019, last revision 10/13/2019