
|
|
|
||
|
|
|
|
|
Ridge Split
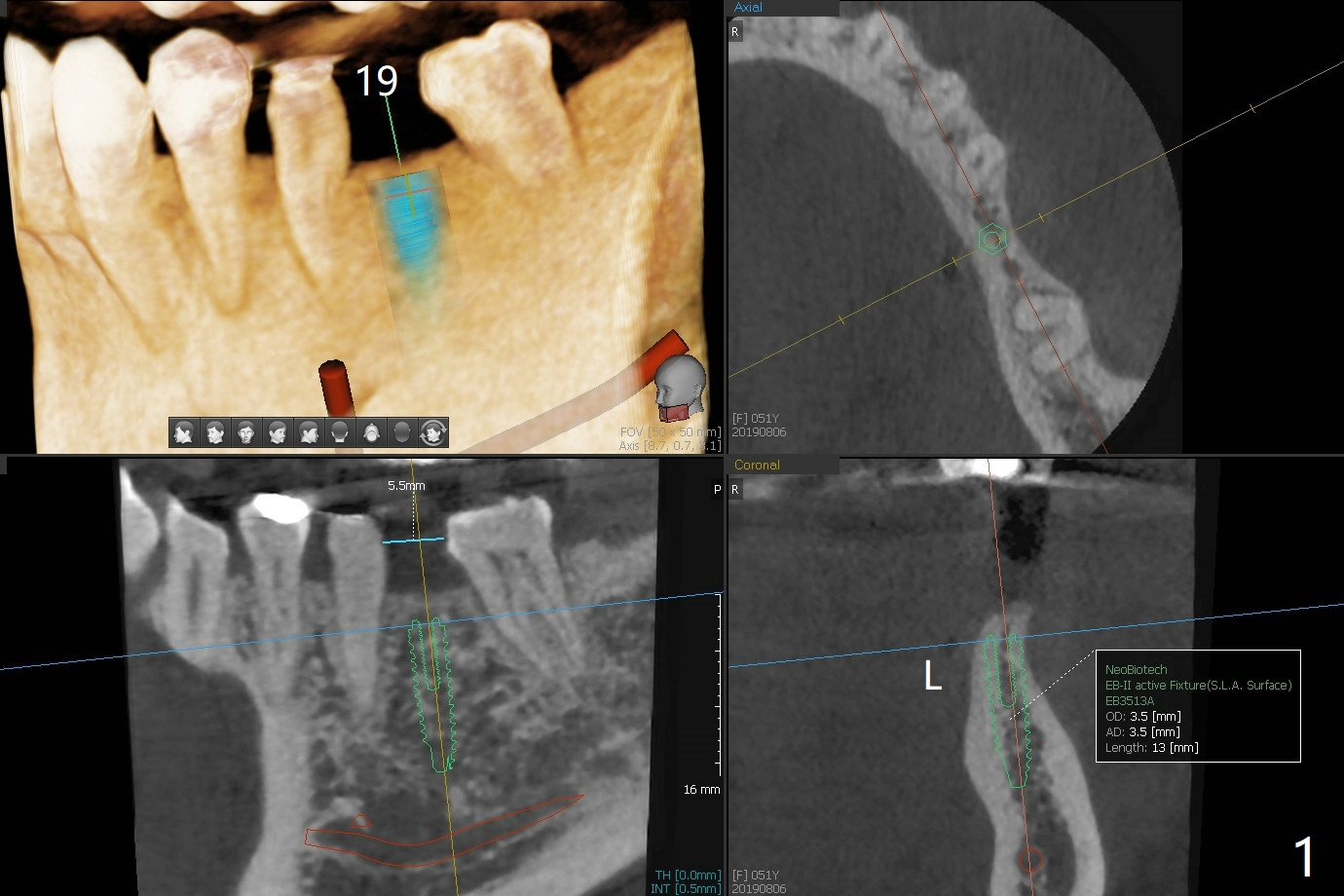
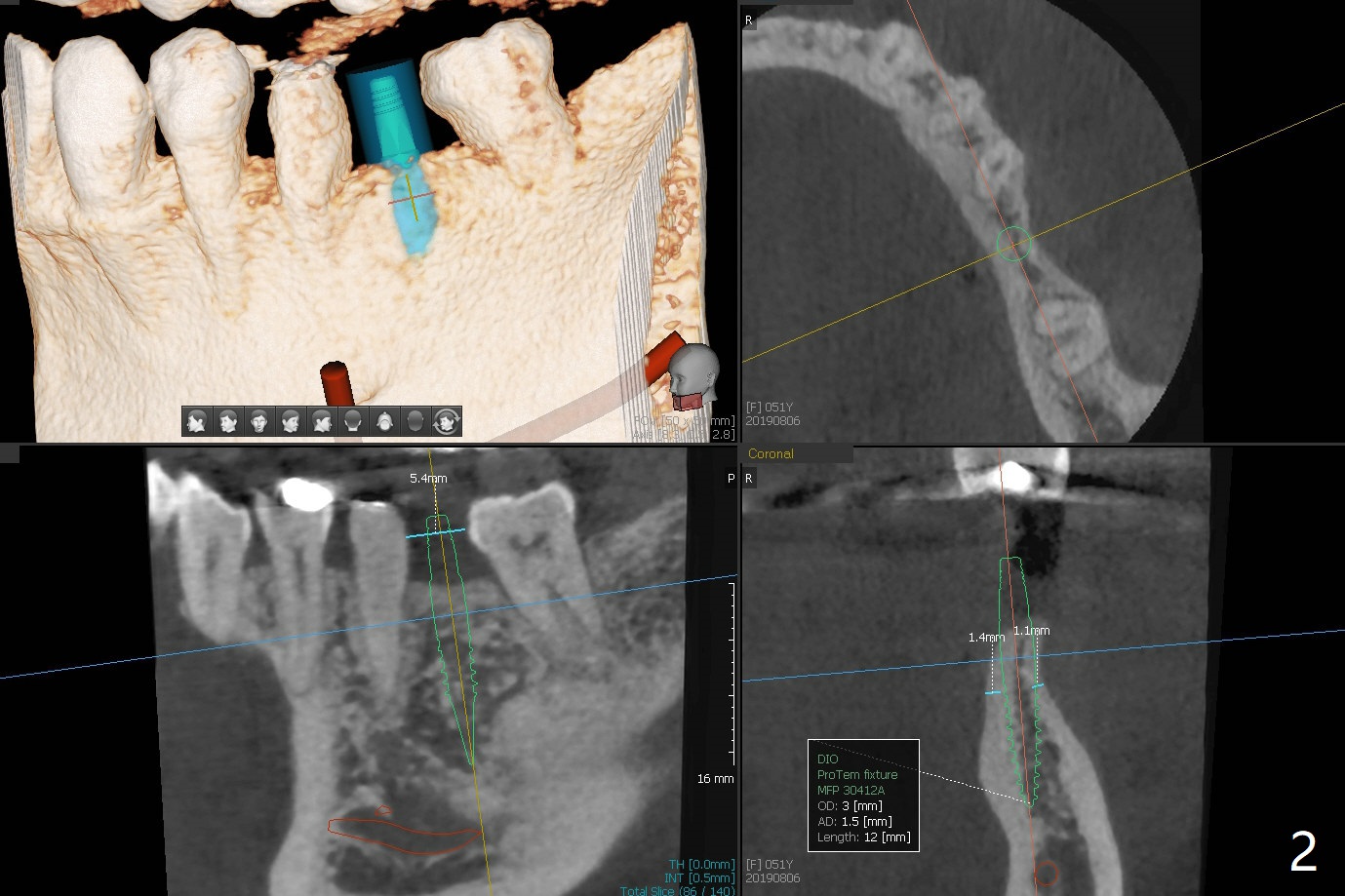
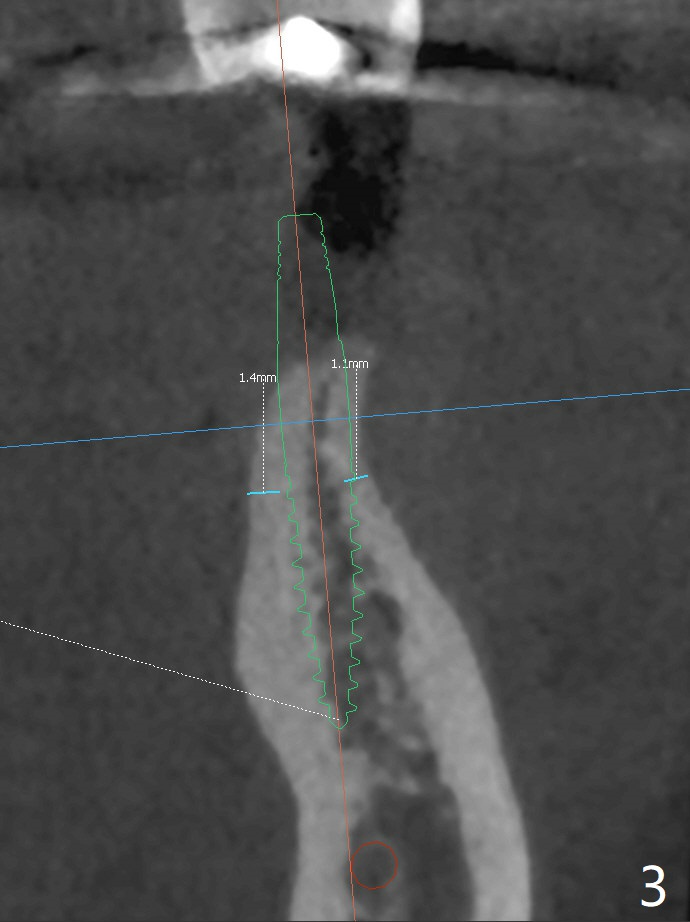
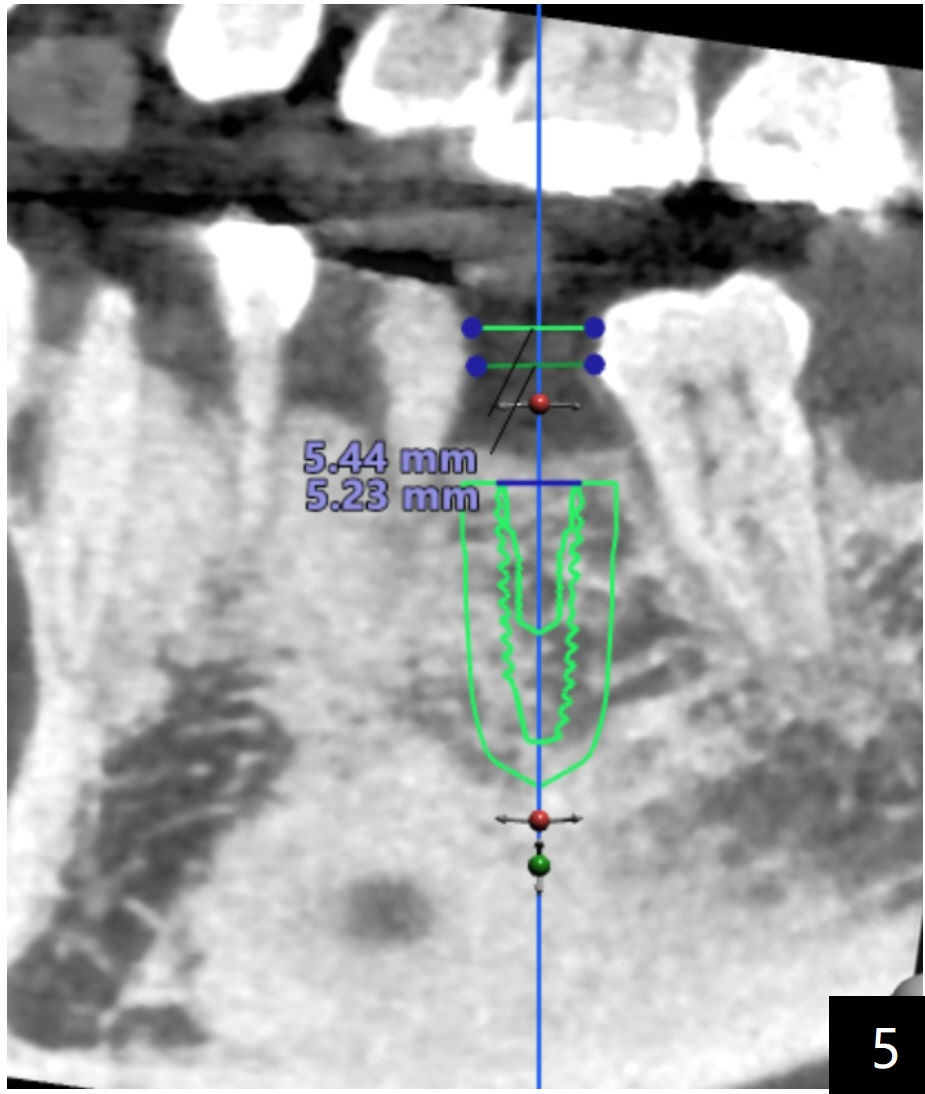
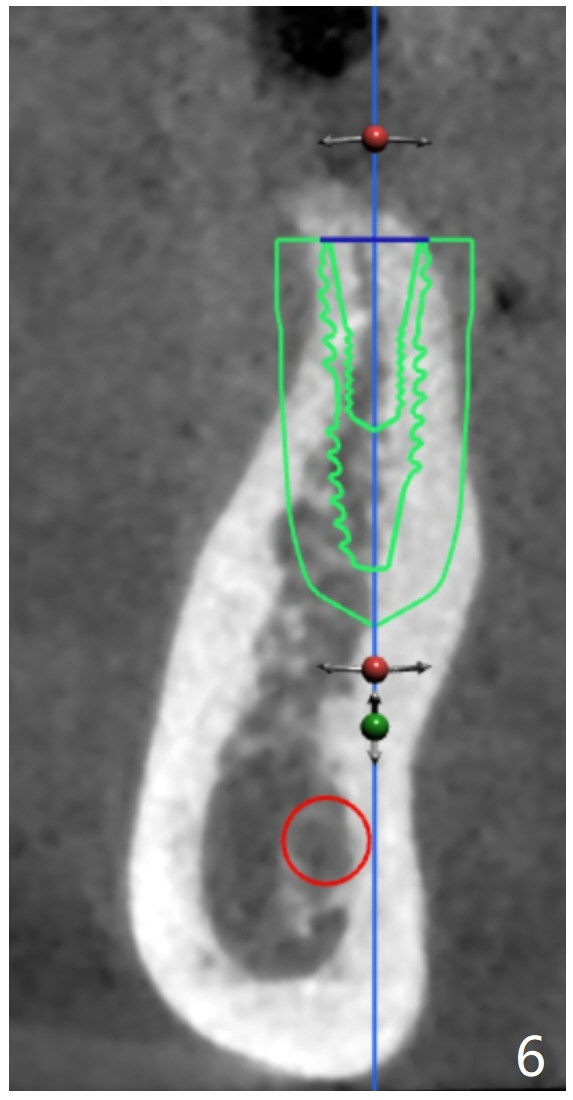
A 51-year-old woman has discomfort with #18-20 overcontoured FPD. CT, taken after removal of the FPD, shows the narrow space and narrow ridge. A 3.5 mm 2-piece (Fig.1) or 3.0 mm 1-piece (Fig.2,3) implant is indicated. For ridge split, the ridge top will be trimmed with surgical handpiece and round bur (Fig.4).
To avoid wound dehiscence associated with 1-staged ridge split, two-staged one will be conducted. In the first surgery, incision will be made (one over the ridge, two vertical). After elevation of the flaps with suture fixation, surgical handpiece and round bur will be used as a bone trimmer on the top of the ridge. Seat the surgical guide and use 2.2 mm drill until the depth. Use the handpiece and a new thin fissure bur to make bony cuts. Tap #15 blade and Tatum bone scalpels and blades for incomplete ridge split. Suture the wound.
Three weeks later, make the ridge top incision, use DIO bone expanders for ridge split and drills for necessary osteotomy and place a narrow implant.
Return to Lower Molar Immediate Implant, Trajectory II 1-staged Ridge Split 2-stage Ridge Split Xin Wei, DDS, PhD, MS 1st edition 08/15/2019, last revision 09/06/2019