
,%20Vanilla.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
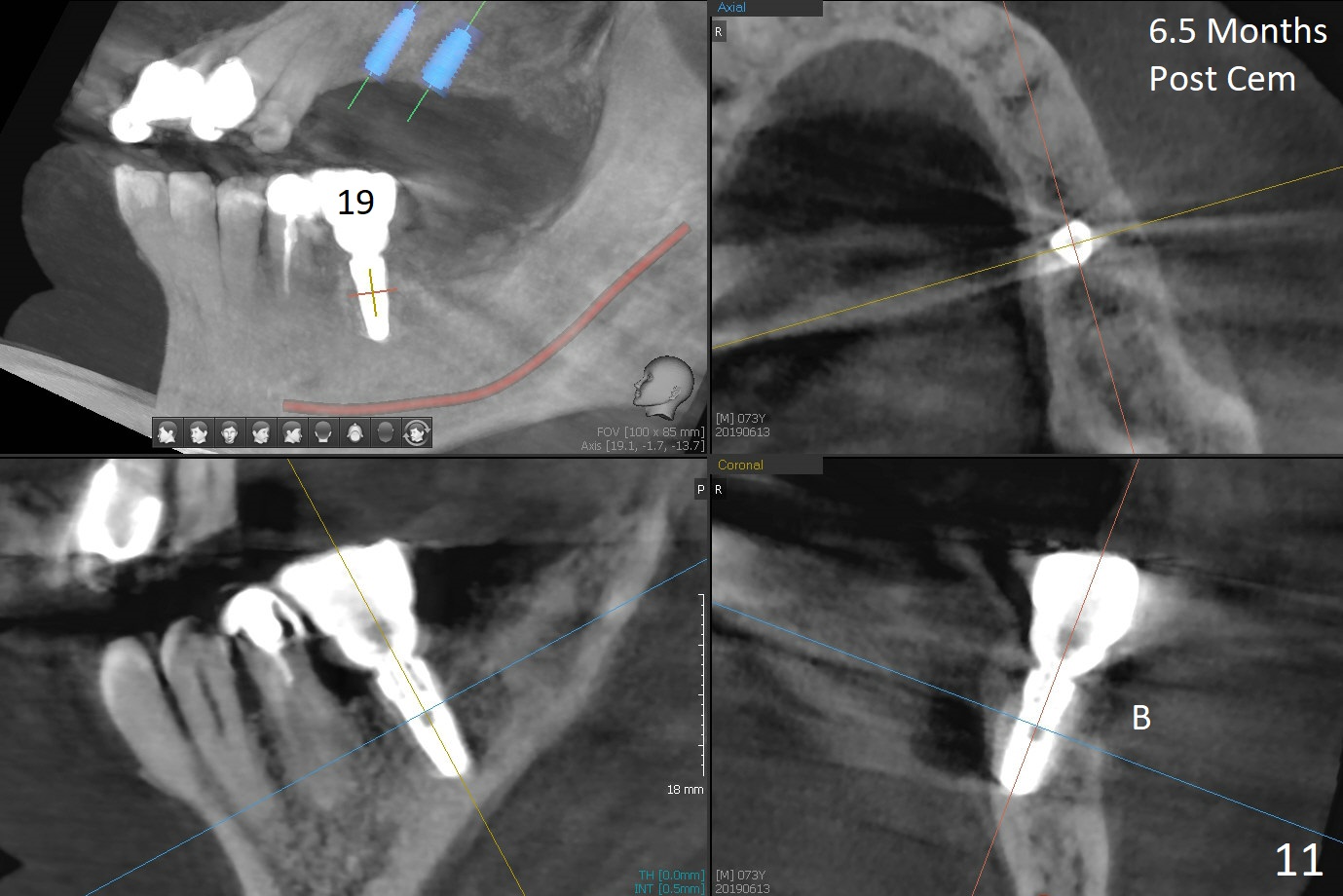
Implant Placed 3 mm Above the Bone
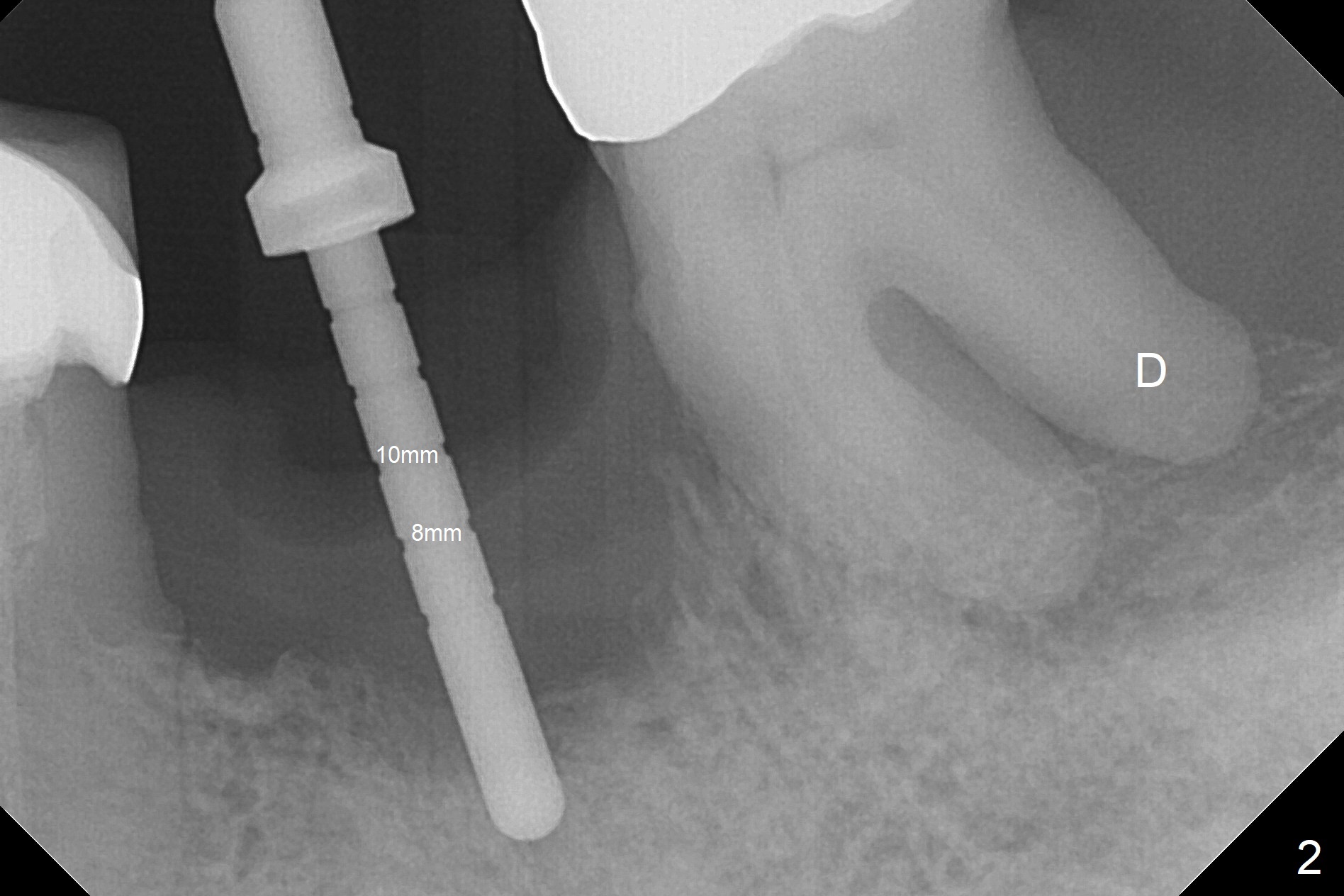
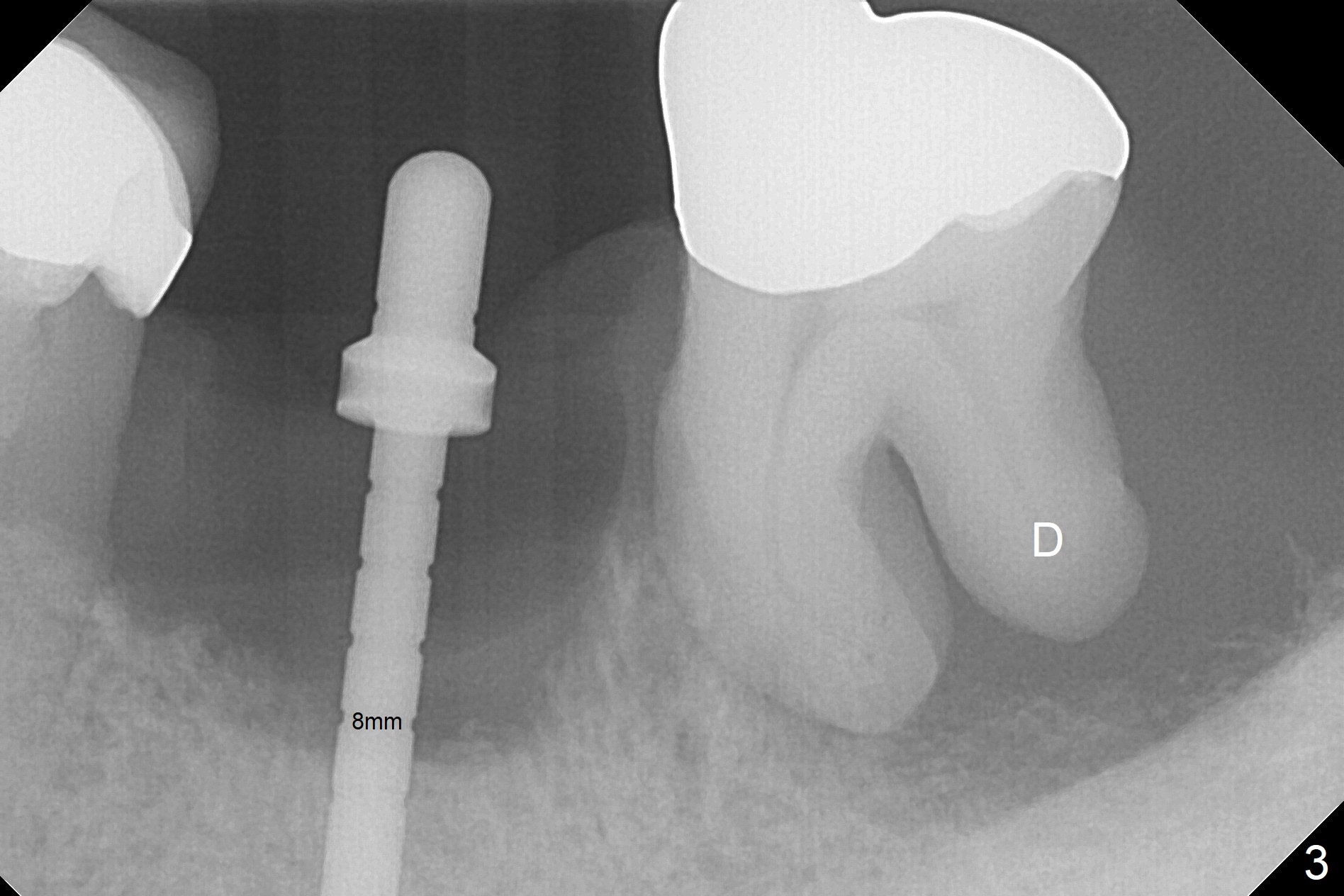
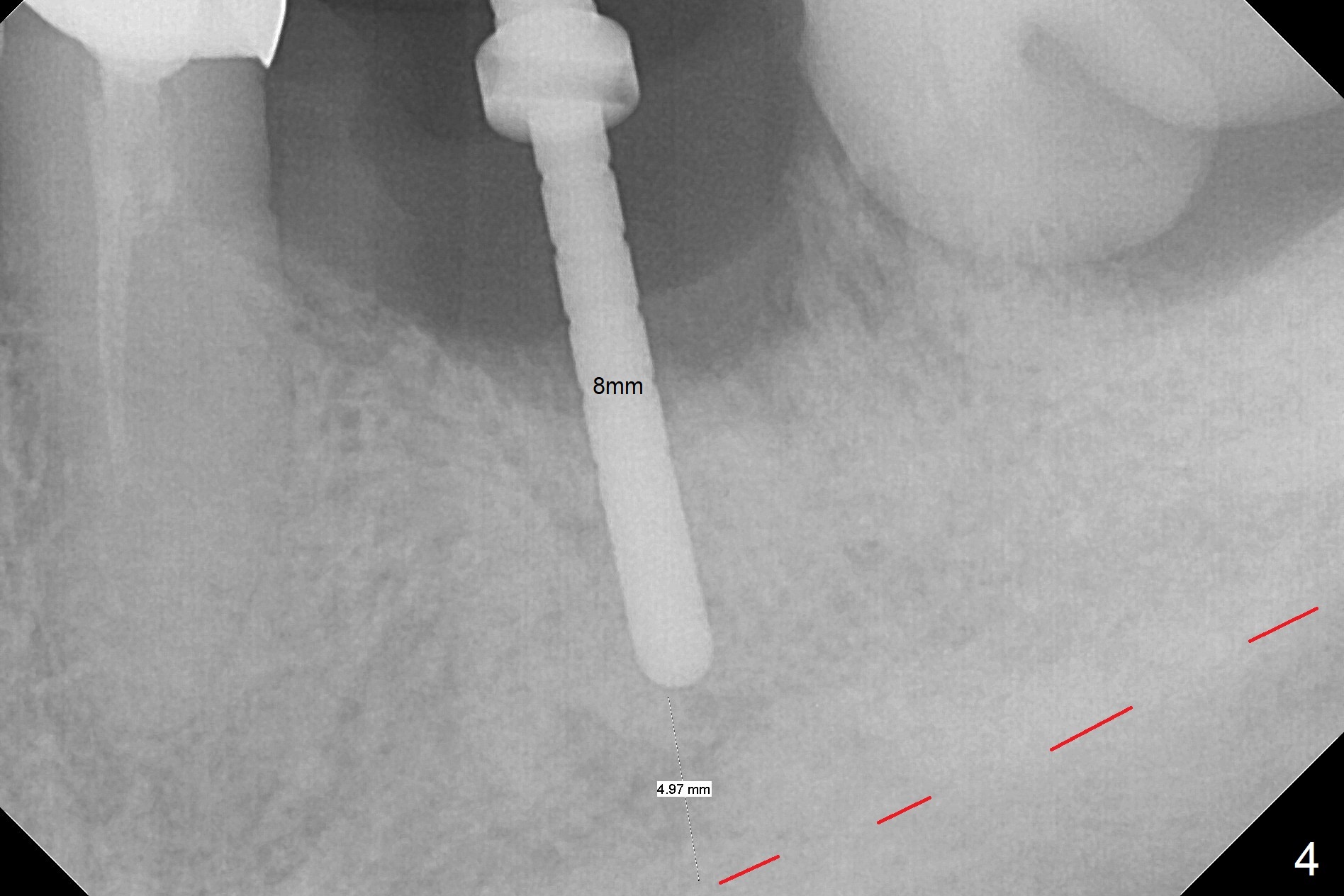
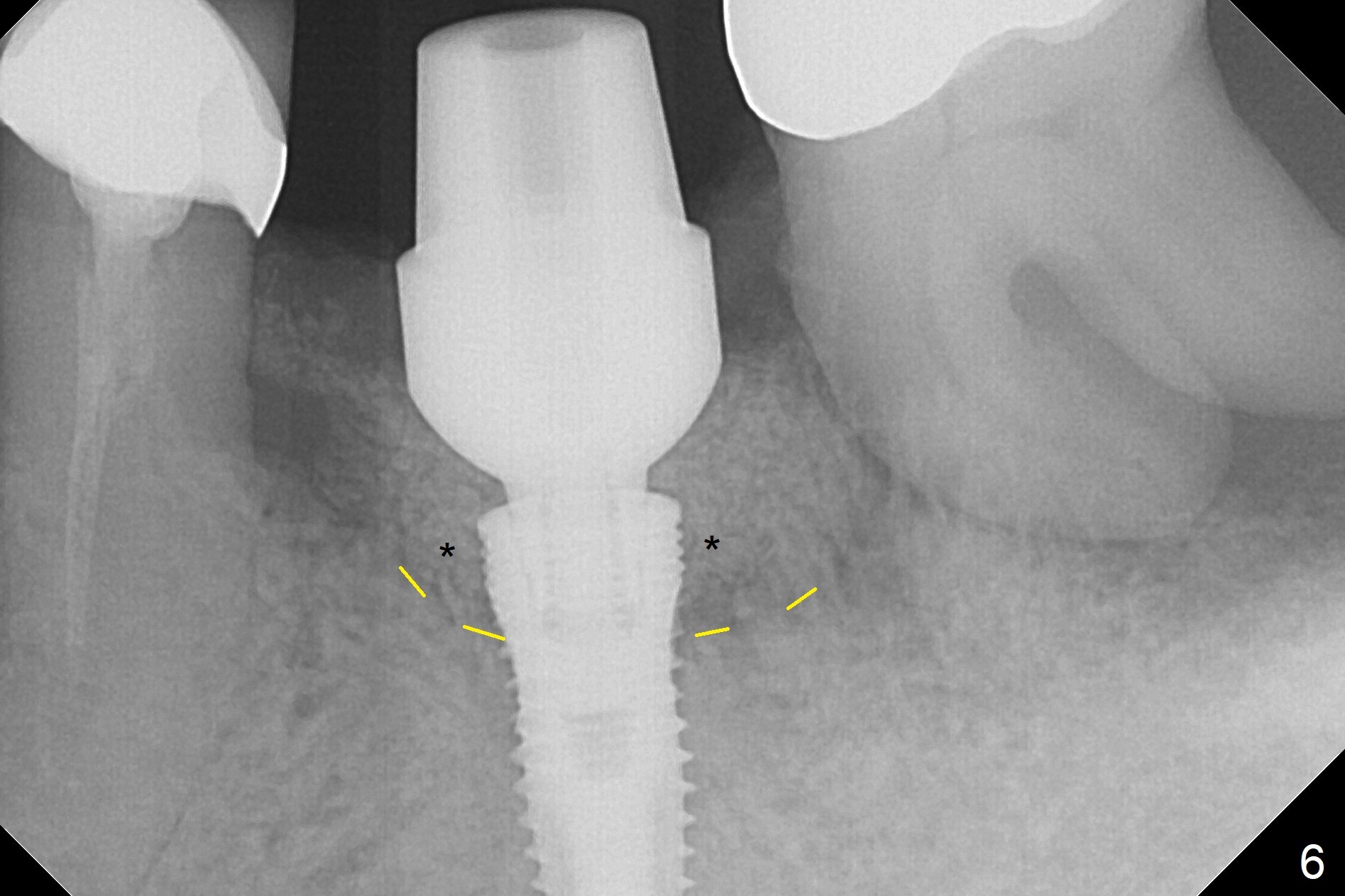
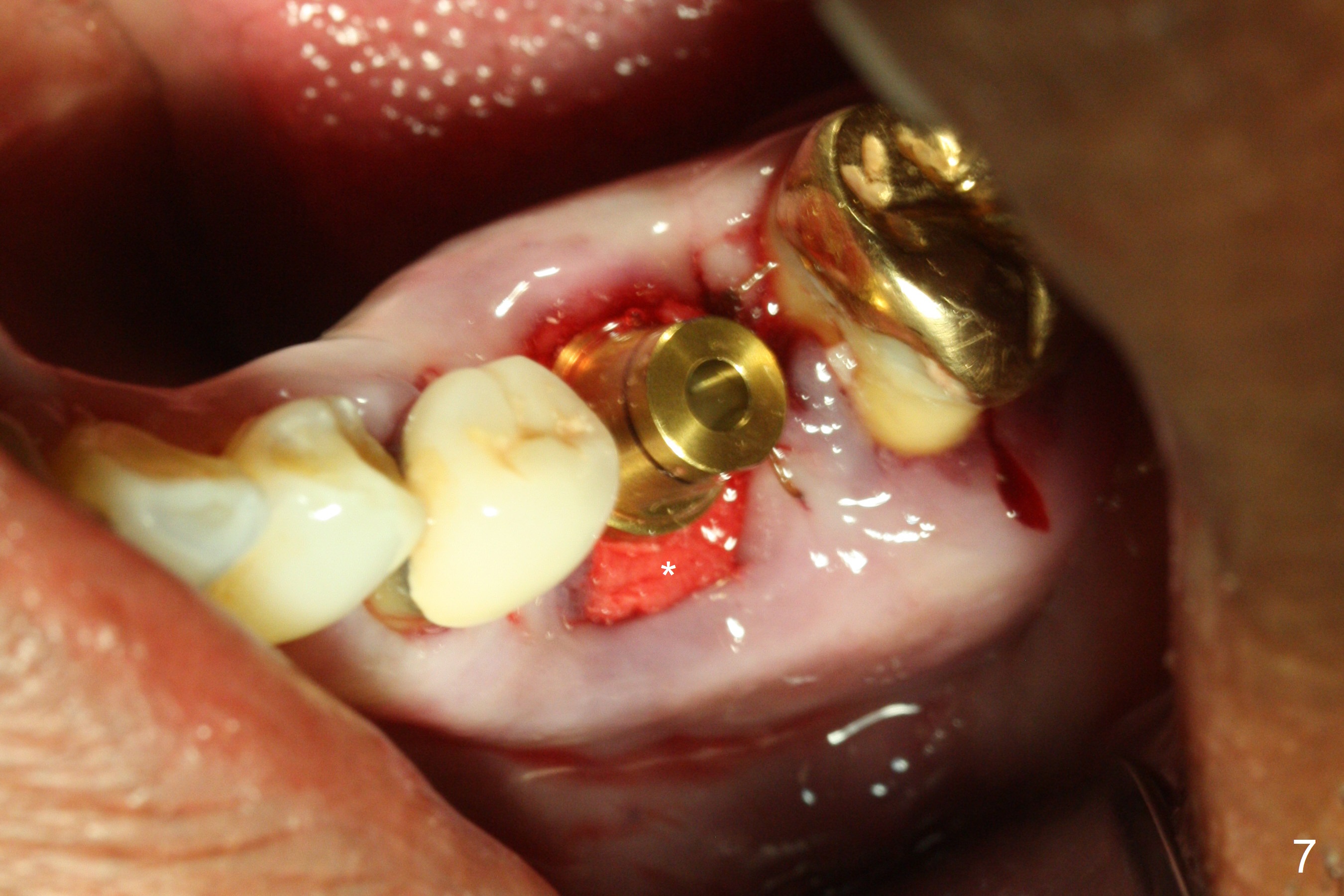
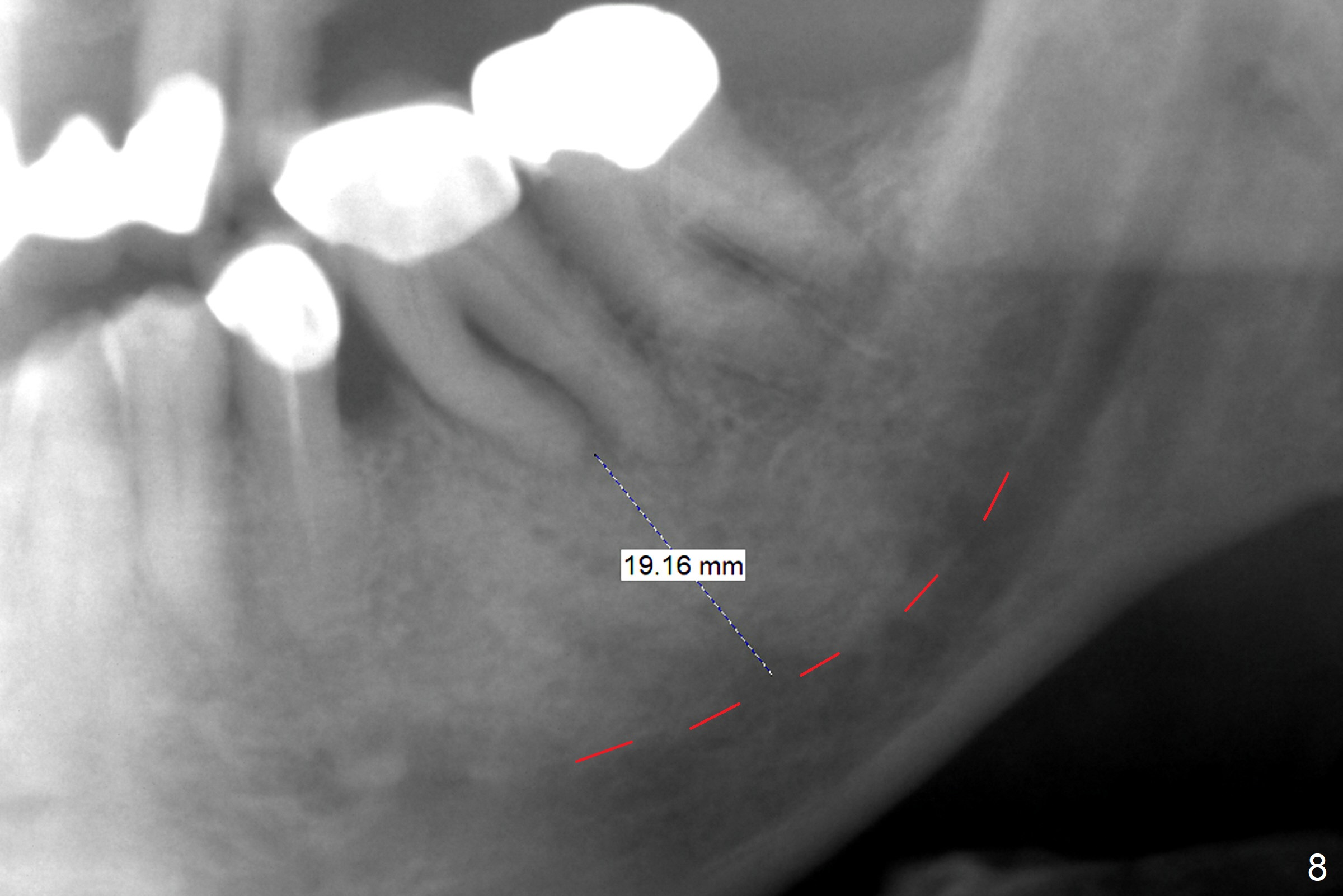
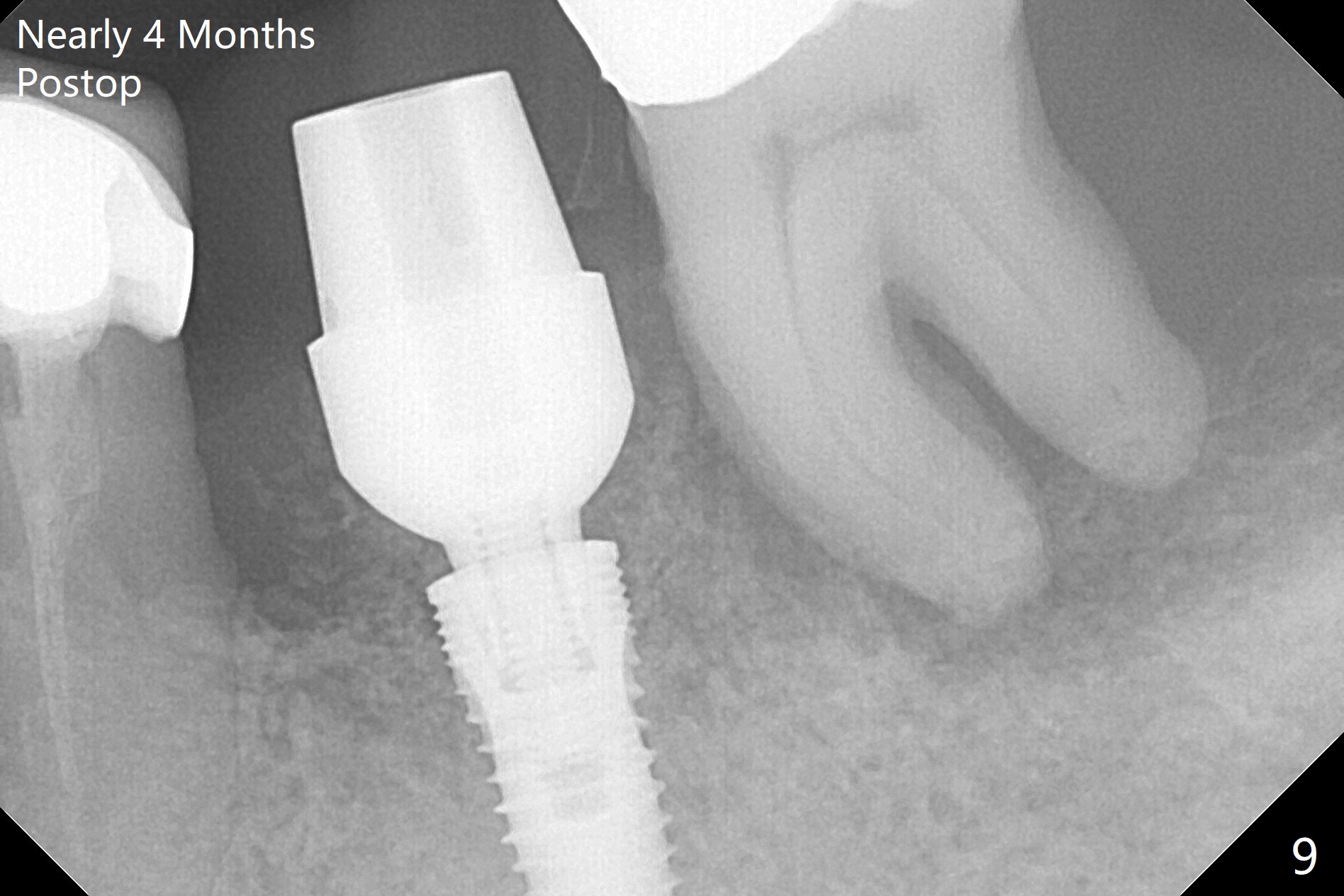
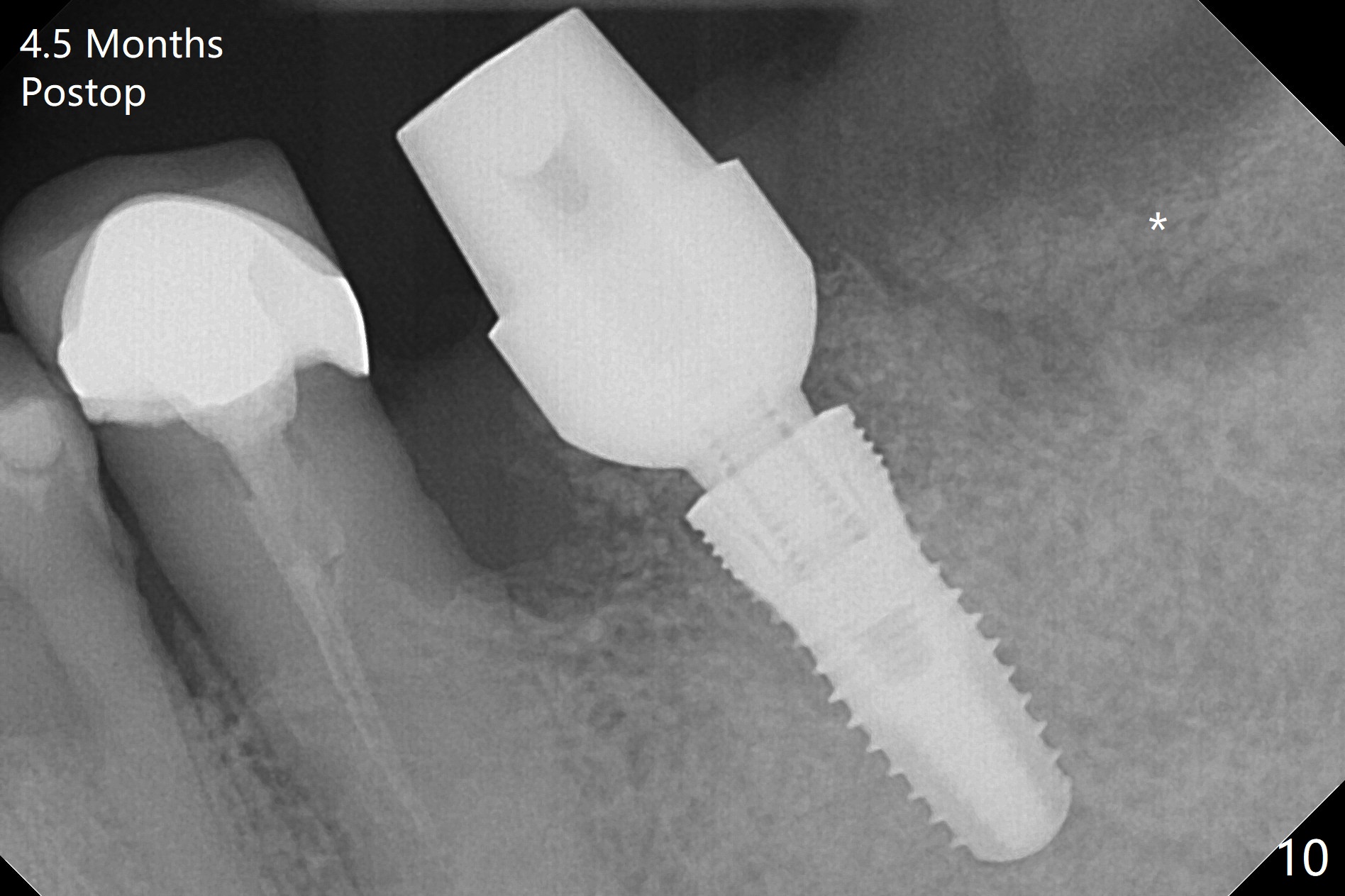
After extraction of the supraerupted tooth #19 with severe buccal gingival recession, the buccal and lingual plate are found to be lost. The sockets are fused and flat without the septum. The bone is hard and painful for the initial osteotomy with infiltration anesthesia (Fig.2). Following block anesthesia, the initial osteotomy depth extends to 8 mm (Fig.3,4). With apparent 4.9 mm clearance, the osteotomy is further extended to 10 mm. The osteotomy walls are apparently intact without severe hemorrhage after each drill. Due to the thick gingiva and severe bone loss, a 5x12 mm implant is intentionally placed 3 mm above the base of the socket bone (Fig.5,6 (yellow dashed line)). Vanilla Cortical and Cancellous allograft (Fig.6 *) is placed around the exposed implant and 7.8x5(6) mm abutment with 4 and 2 mm buccal and lingual gaps. Next collagen plug cut in strip is placed to fill the most coronal aspect of the socket (Fig.7 *). The buccal and lingual gingivae are approximated with sutures proximally. Finally periodontal dressing is applied. Since the Inferior Alveolar Canal is vague in intraop PAs (Fig.4,5), there is worry about potential nerve damage during and after osteotomy. This should be no issue if preop panoramic X-ray is reviewed with measurement (Fig.8). The bone graft appears to remain in place nearly 4 months postop (Fig.9). Two weeks later, he returns for impression. When the provisional is removed, the gingiva is unhealthy. Without the provisional and with improved oral hygiene, the gingiva is healthy one week later, but the tooth #18 is symptomatic. The latter is extracted with socket preservation (Fig.10 *). There is no apparent bone loss around the implant at #19 6.5 months post cementation (Fig.11).
Return to
Lower
Molar Immediate Implant,
Prevent Molar Periimplantitis (Protocols,
Table),
Armaments,
Trajectory,
FPD,
13,14
Xin Wei, DDS, PhD, MS 1st edition 06/12/2018, last revision 06/16/2019