



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
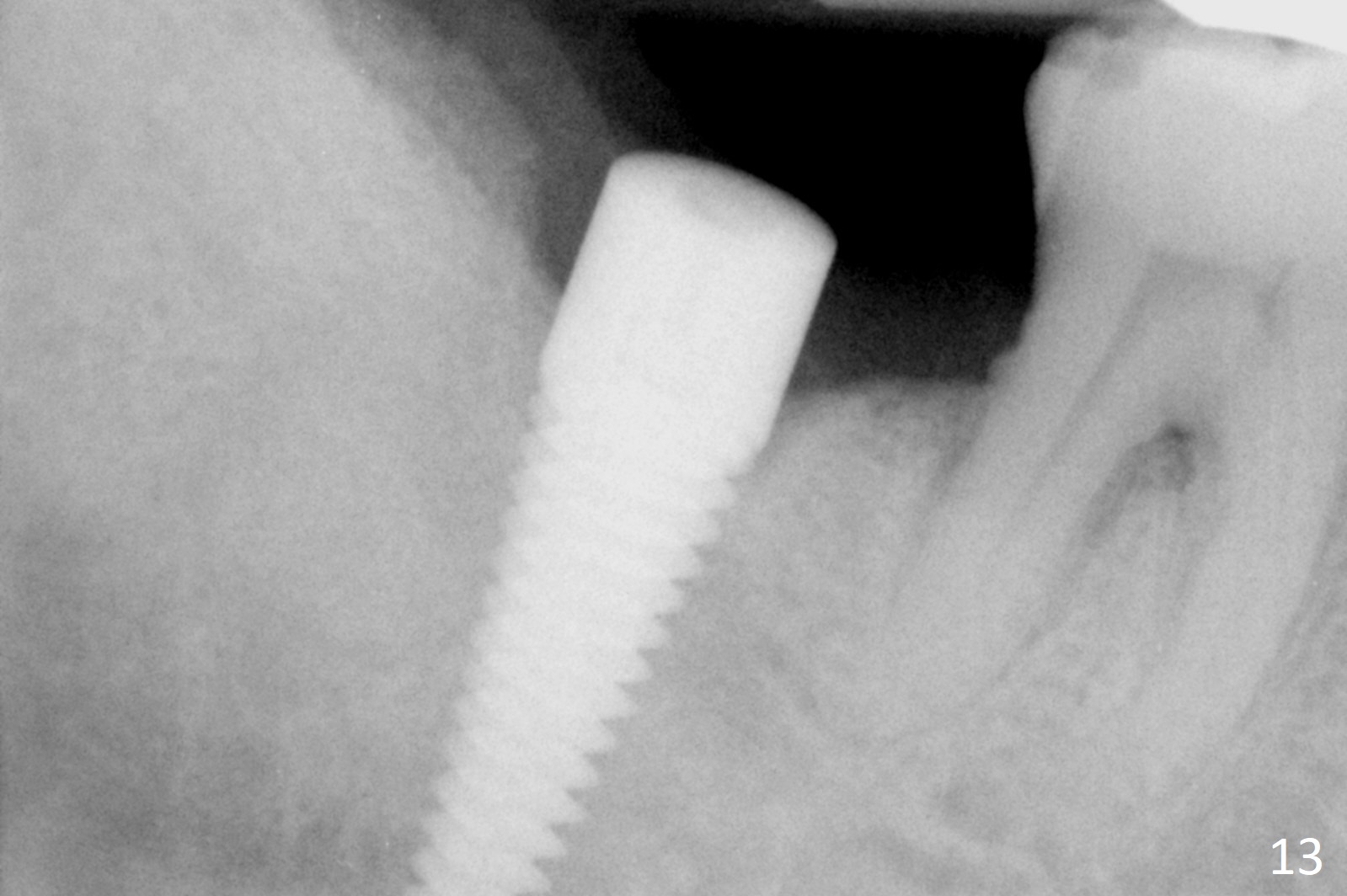
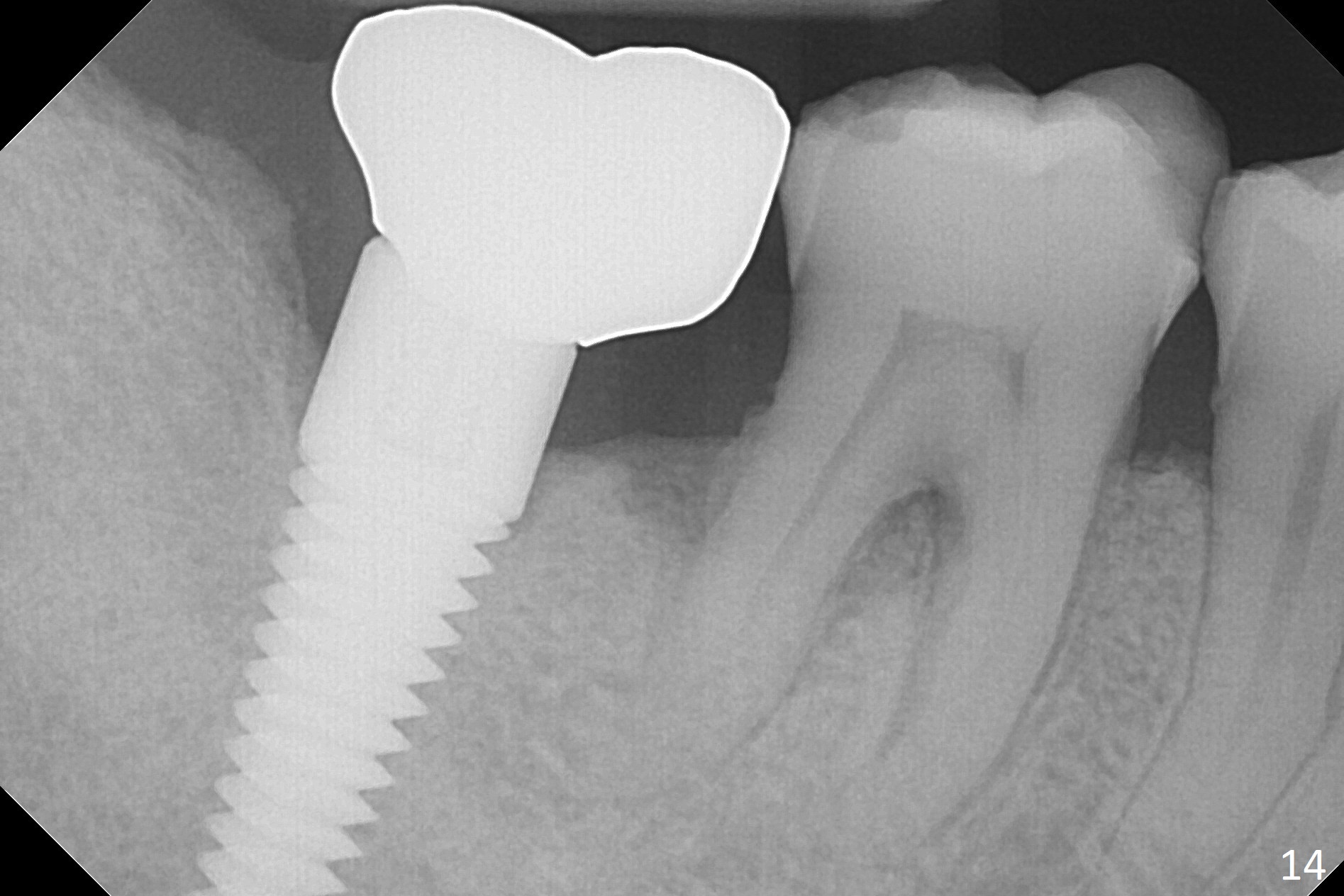
Overloading
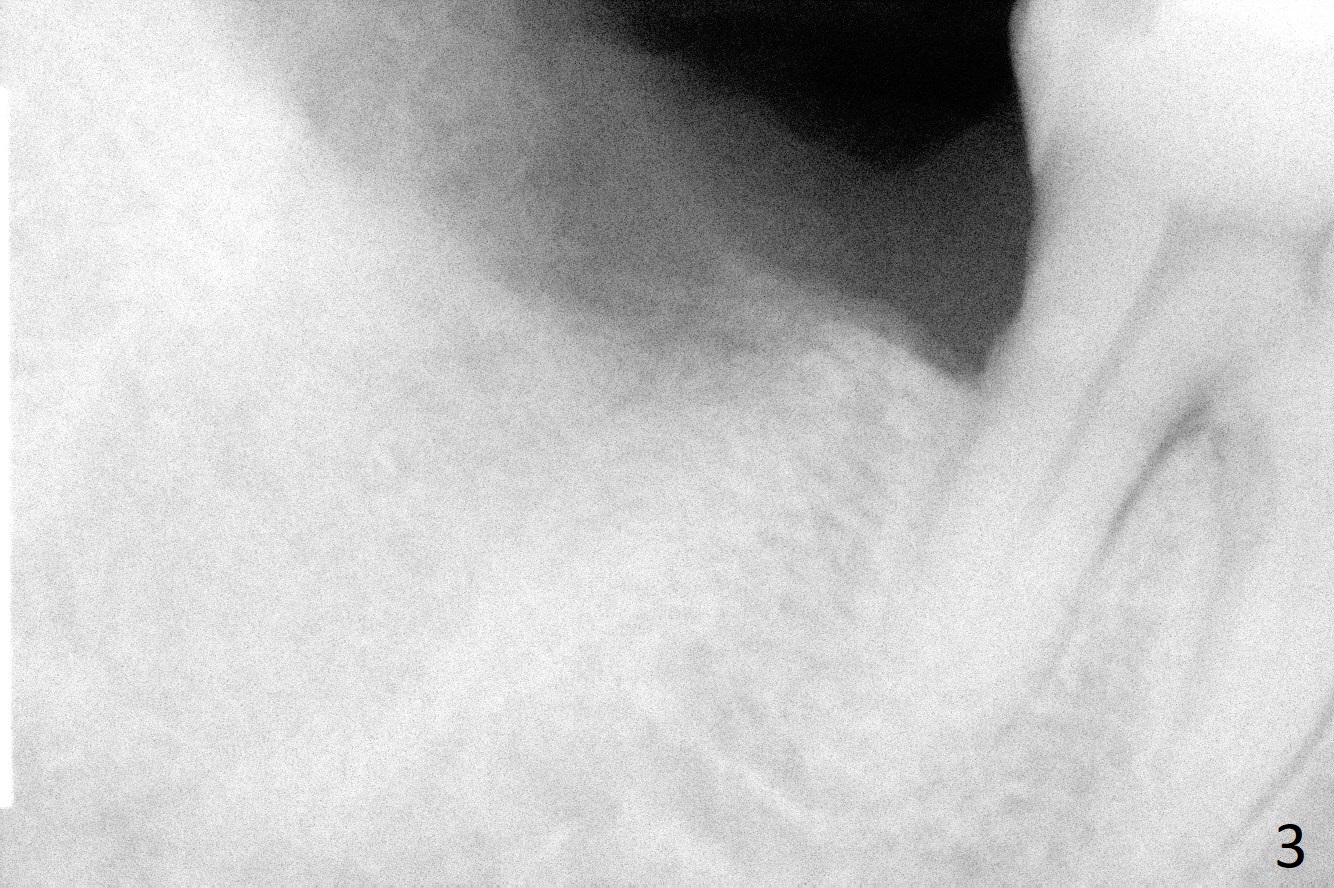
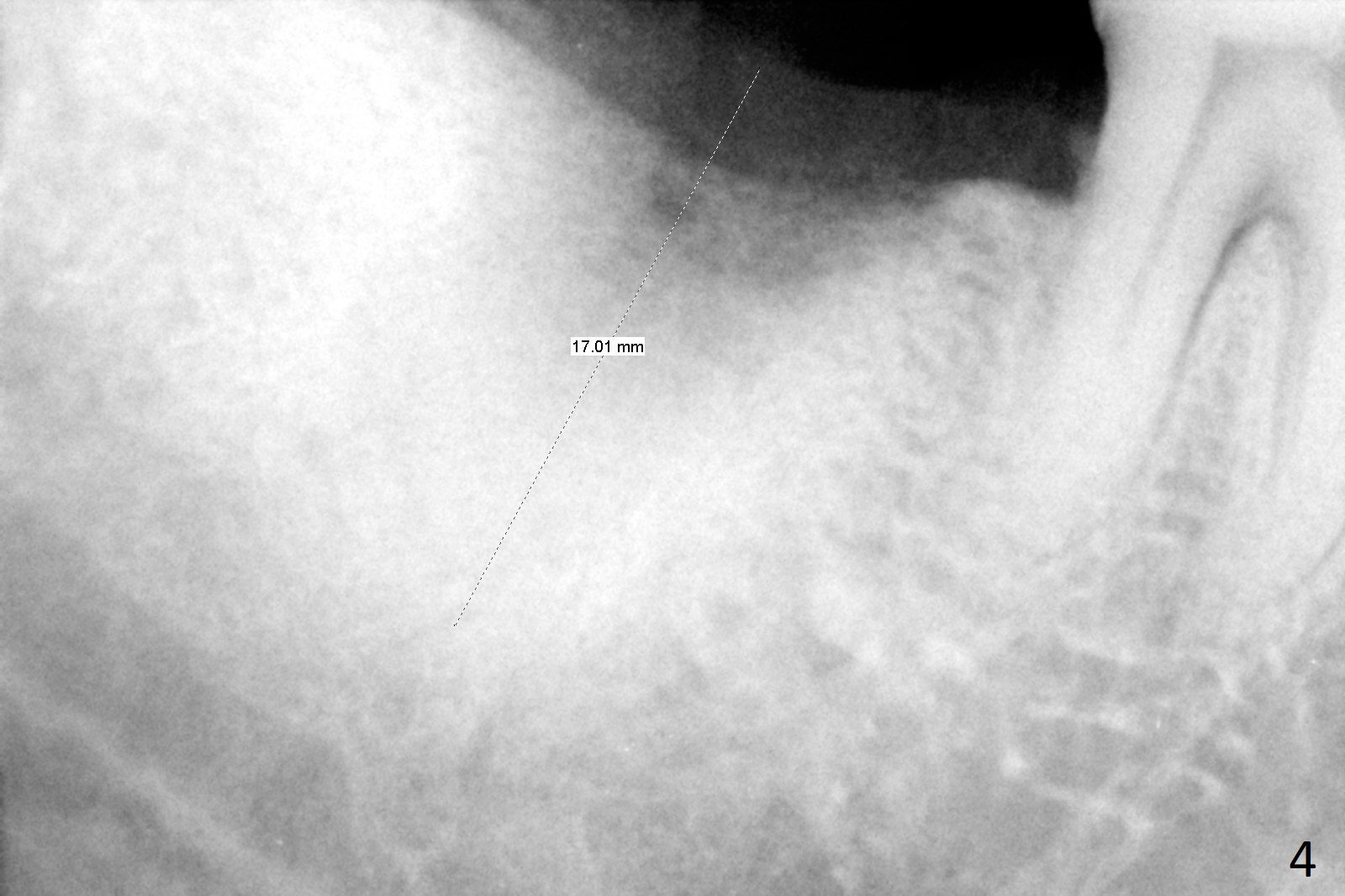
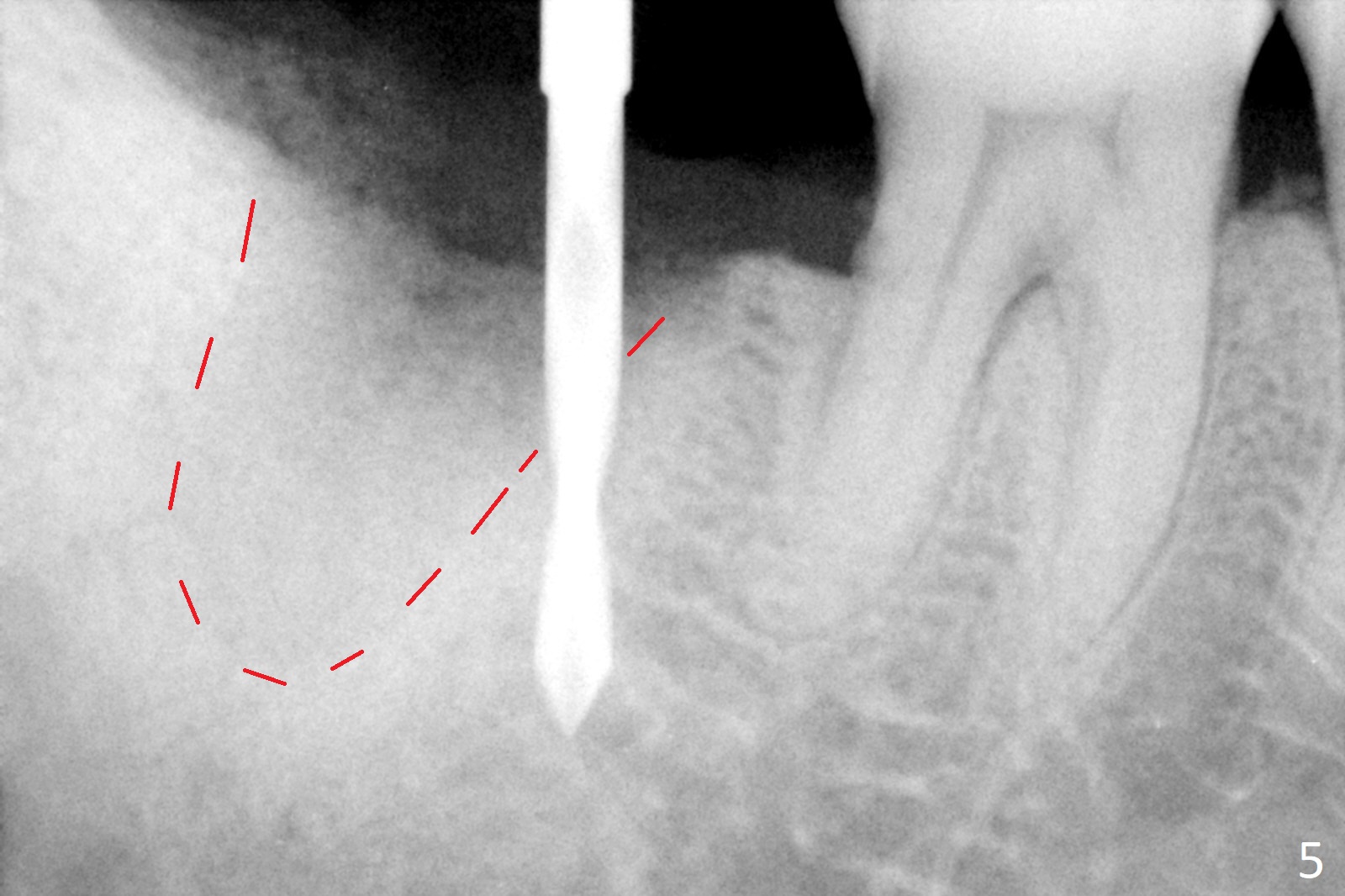
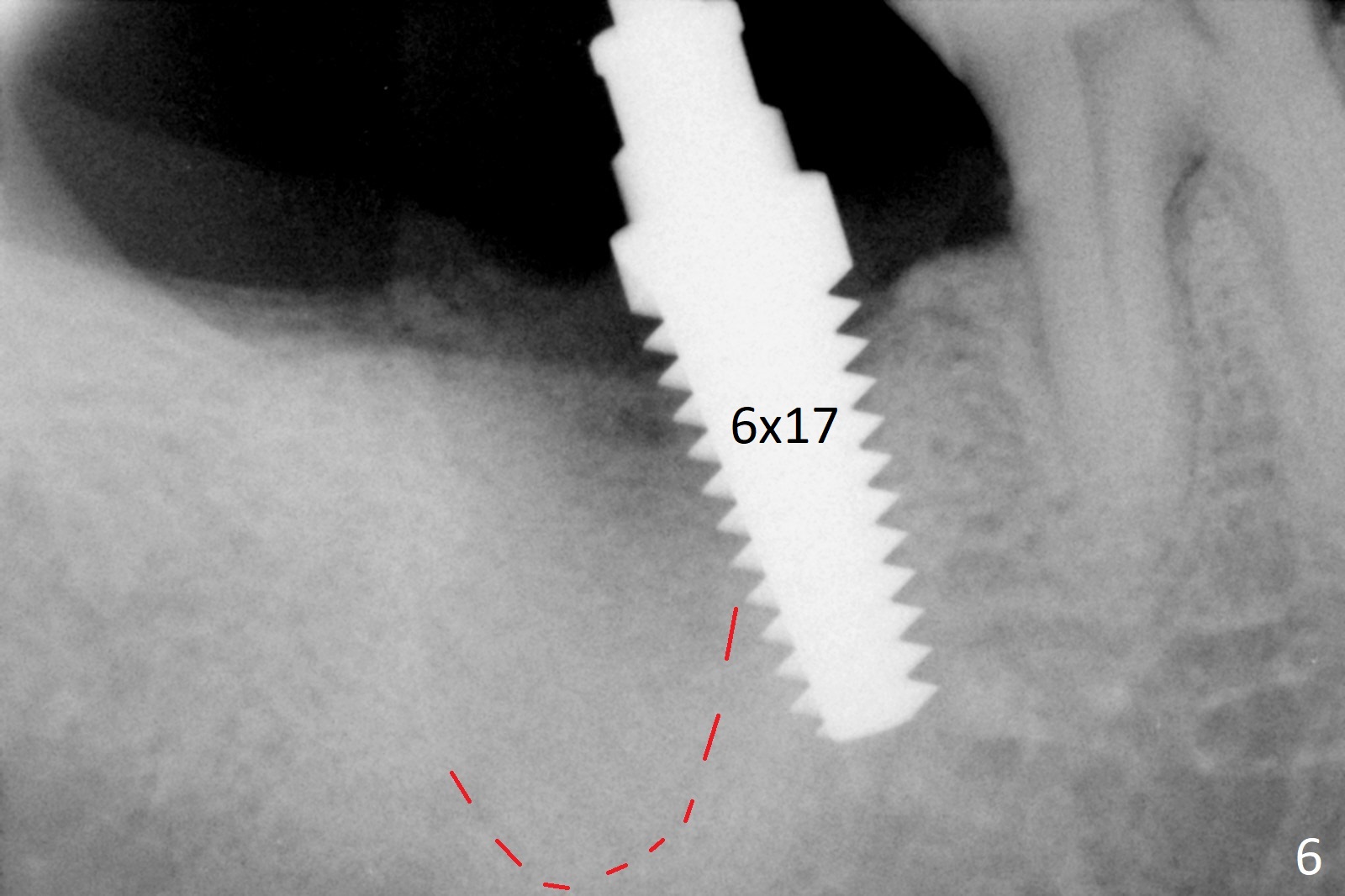
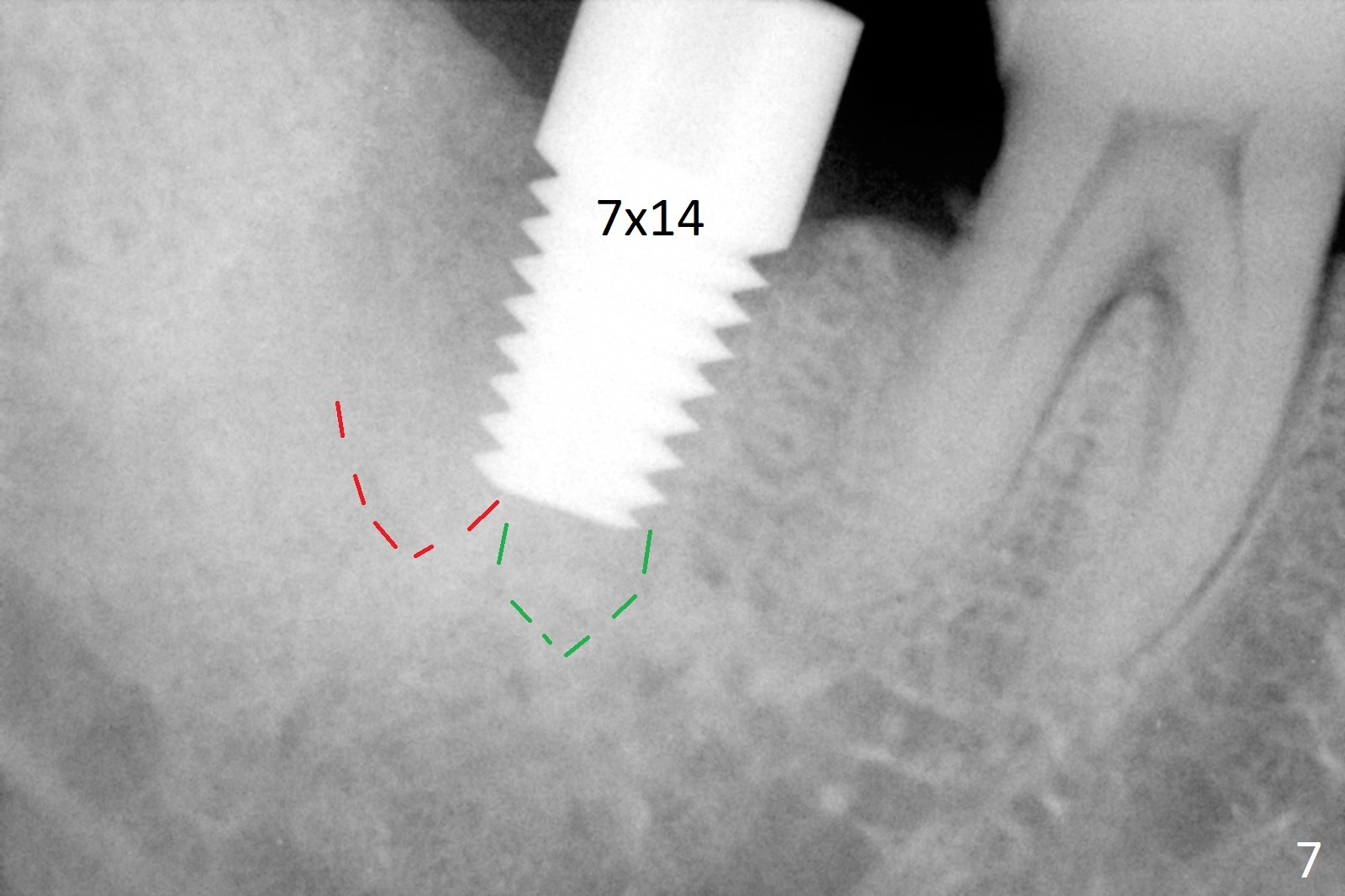
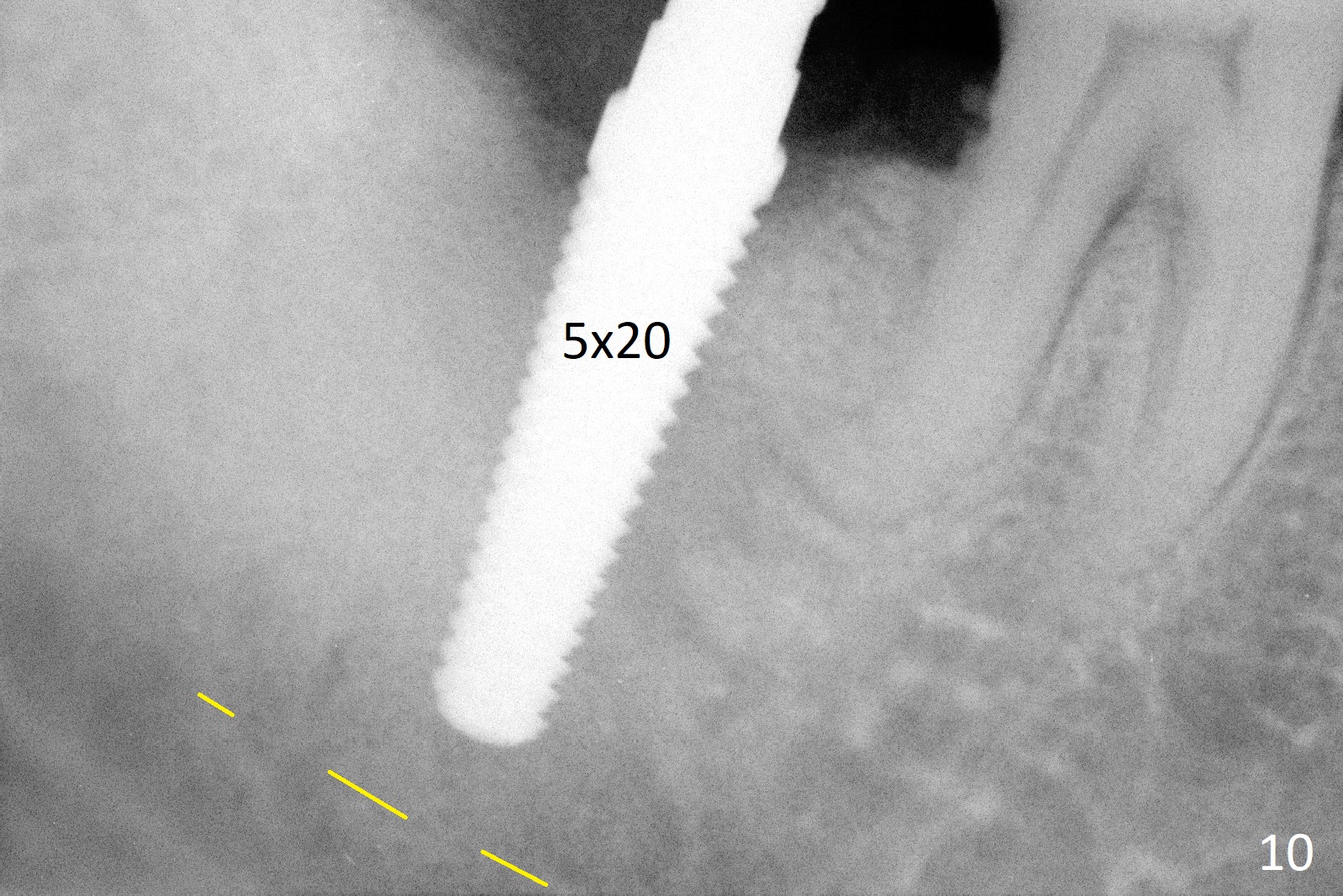
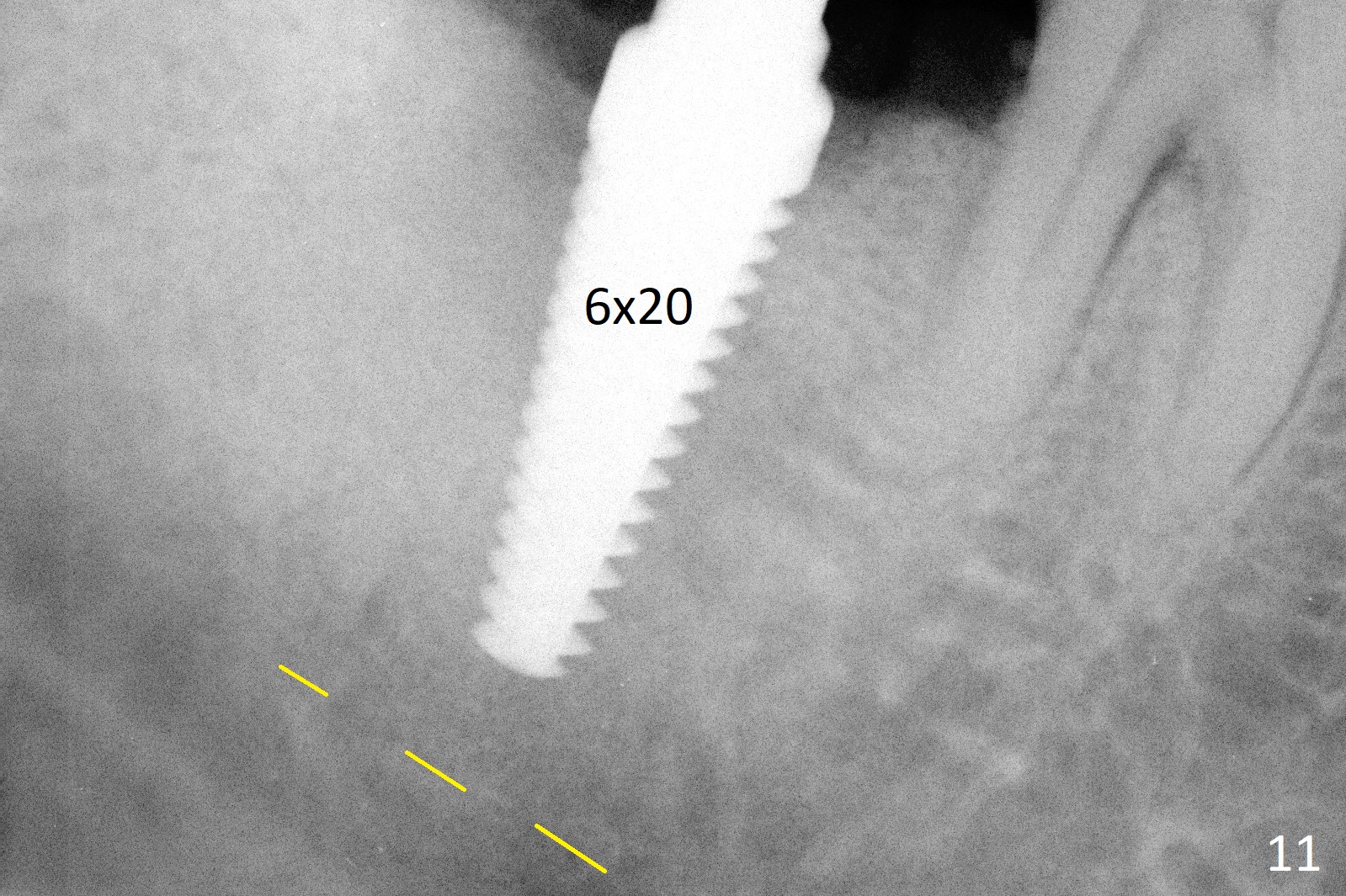
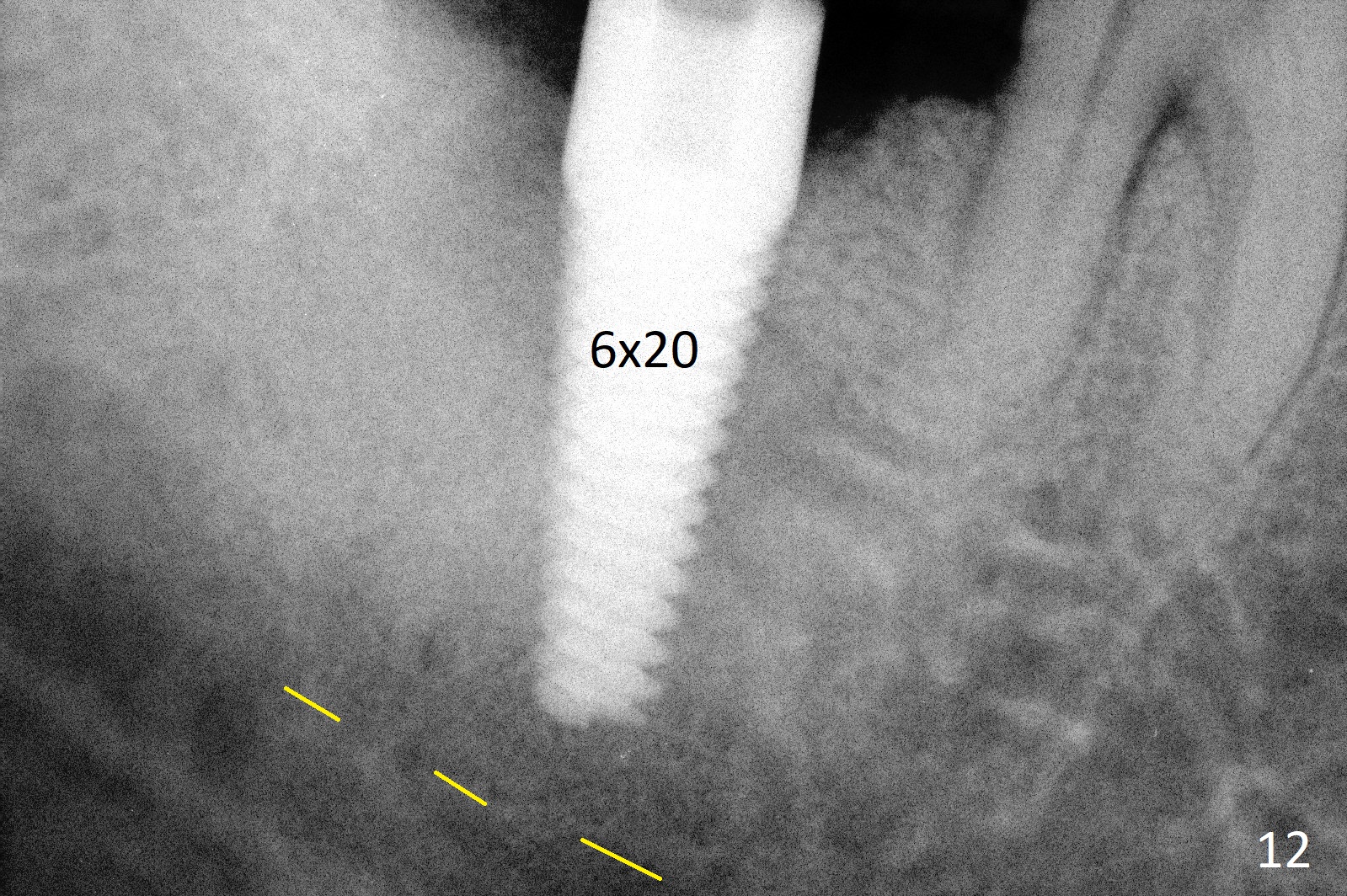
A 50-year-old man, a smoker, presents to clinic with pain of the tooth #15 with apparently occlusal trauma (Fig.1). Two years and three months after #15 extraction, he returns for #31 extraction (Fig.2) and socket preservation (Fig.3). The socket depth is 17 mm along the long axis of the socket 2.5 months post extraction (Fig.4, gingival level). Initial osteotomy is created in the mesial slope of the socket for 14 mm (Fig.5). After sequential osteotomy, a 6x17 mm tap is seated shallower (Fig.6) than the 2 mm drill (Fig.5). Following further osteotomy, a 7x14 mm implant is seated incompletely (Fig.7), which was not found intraop. The implant becomes loose with purulent discharge 19 days postop. The patient returns for 2nd placement 2 months post implant removal (Fig.8). Osteotomy is created probably in the mesial slope with 17 mm (bone level, Fig.9). After insertion of 5 (Fig.10) and 6 (Fig.11) x20 mm taps (tissue level), a 6x20 mm tissue-level implant is placed with clearance from the Inferior Alveolar Canal (Fig.12 yellow dashed line). The implant is restored 8.5 months postop (Fig.13) without bonding 5 mm 0 degree unipost. The crown dislodges 4 months post permanent cementation. Still the patient complains of small crown without occlusal contact. Impression is taken for a new normal-sized crown. The new crown becomes loose 1 year 9 months post cementation (Fig.14). The teeth #14 and 15 remain unrestored.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/10/2014, last revision 12/09/2017