




,%20autogenous,%20vanilla.jpg)




,%2031%205.2x4(2).jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Healing
Abutment vs. Definitive One
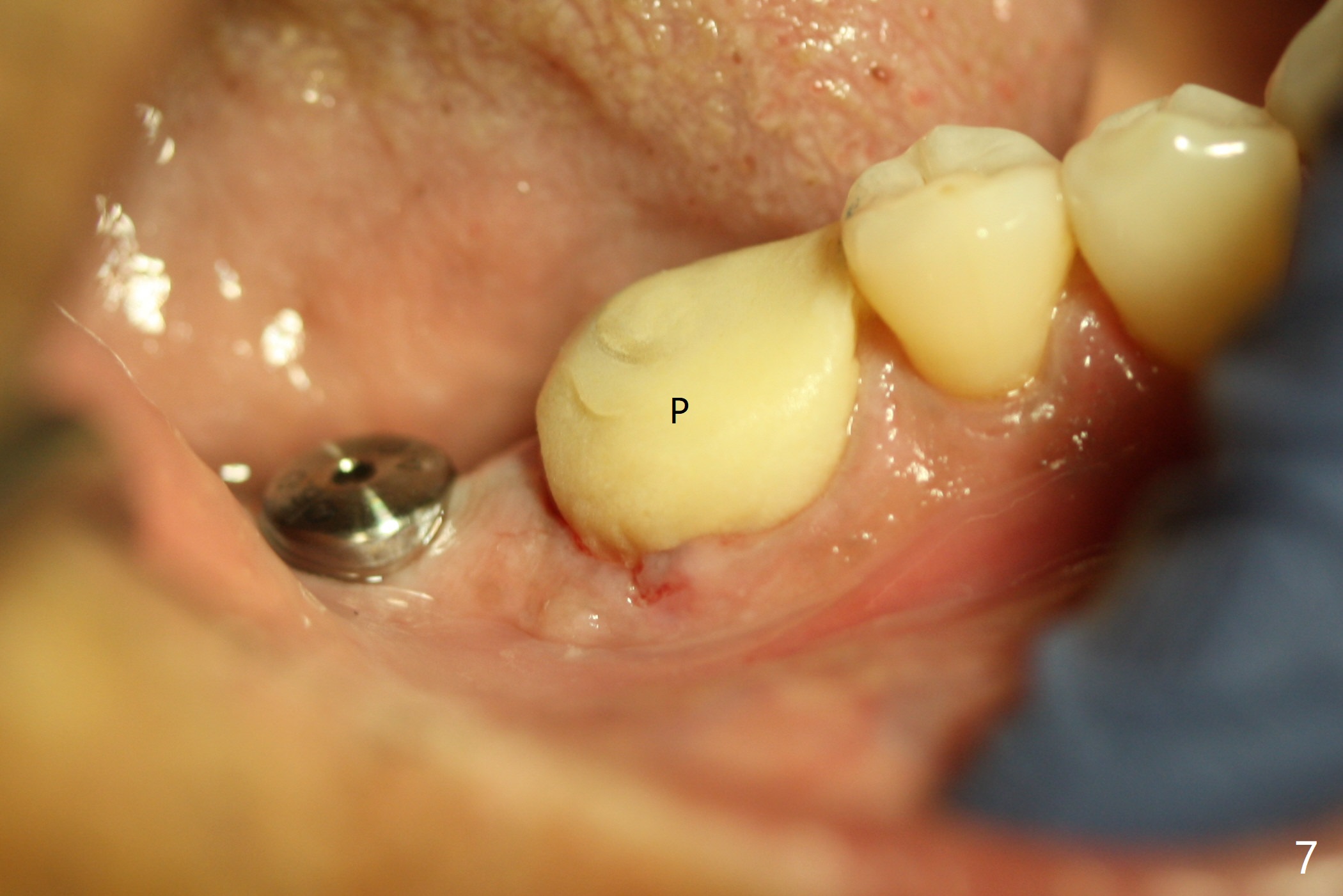
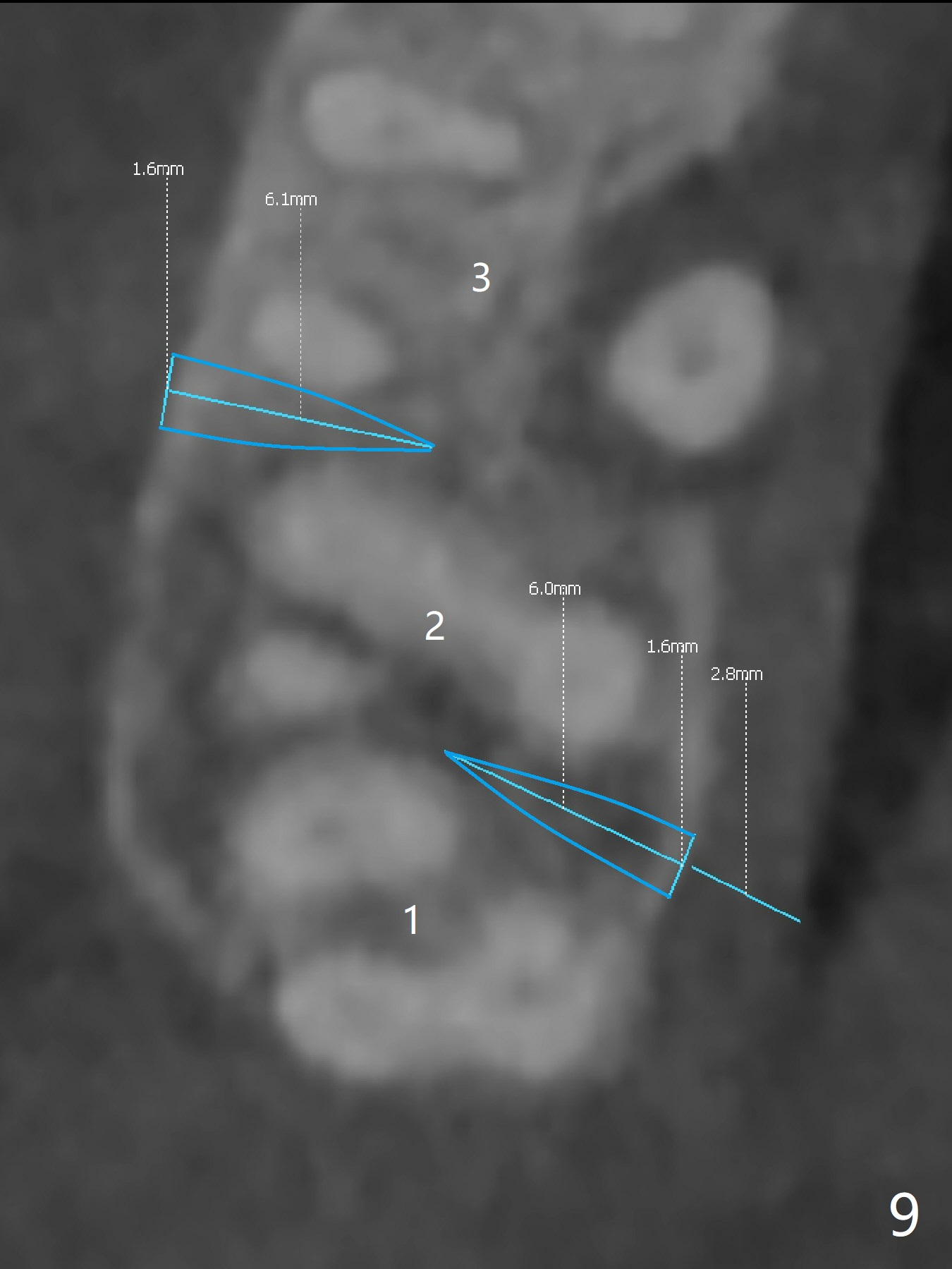
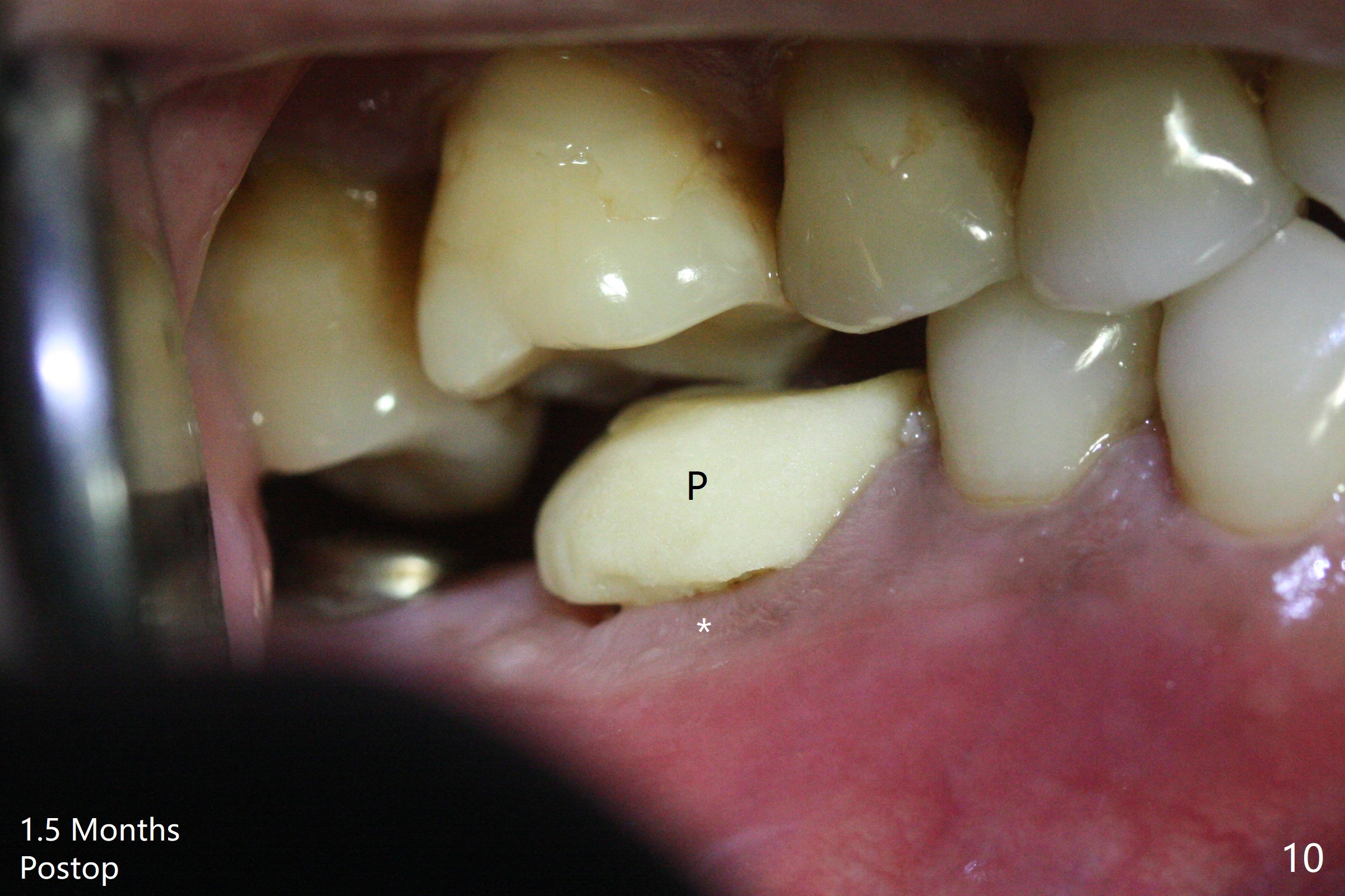
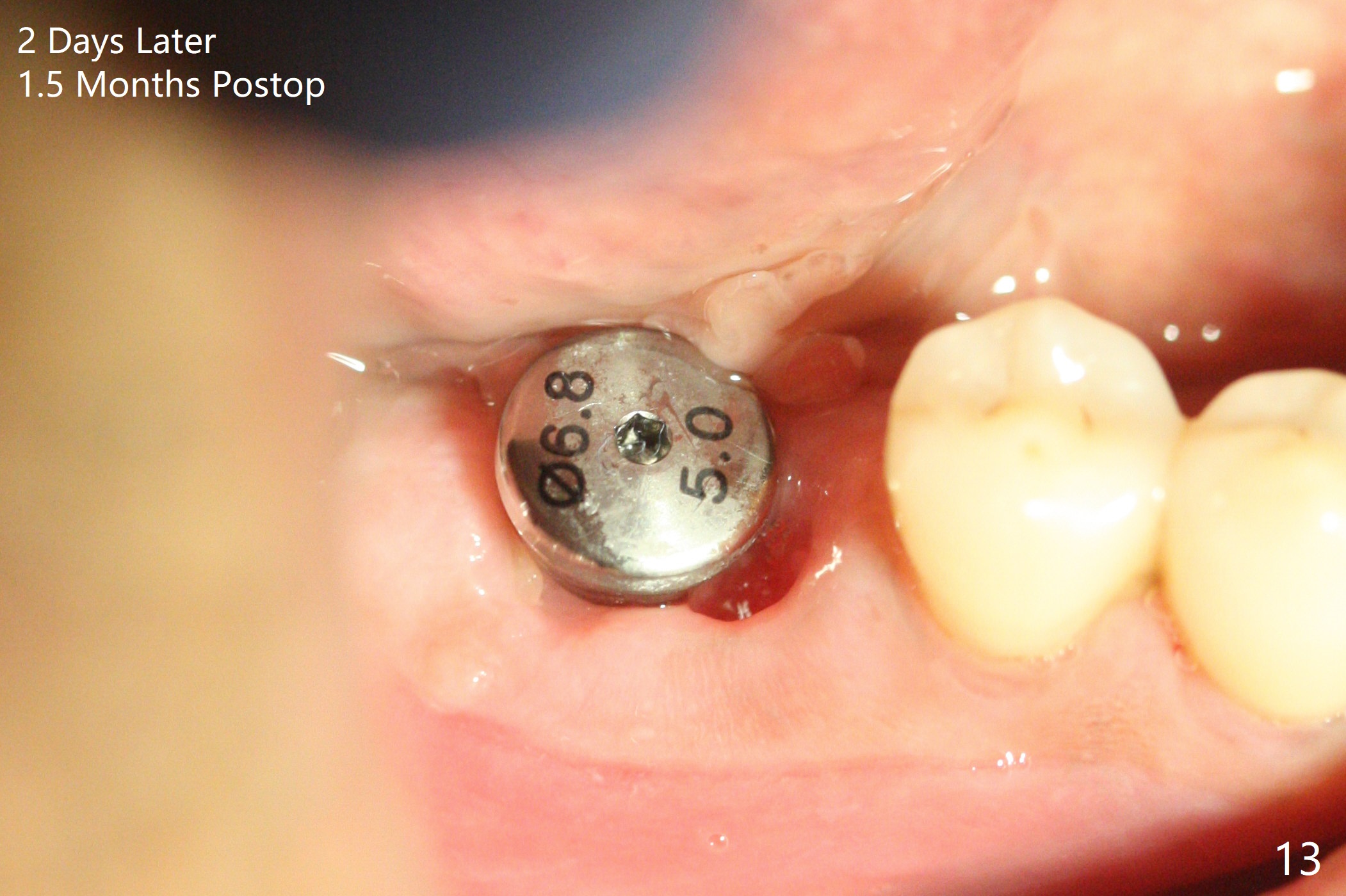
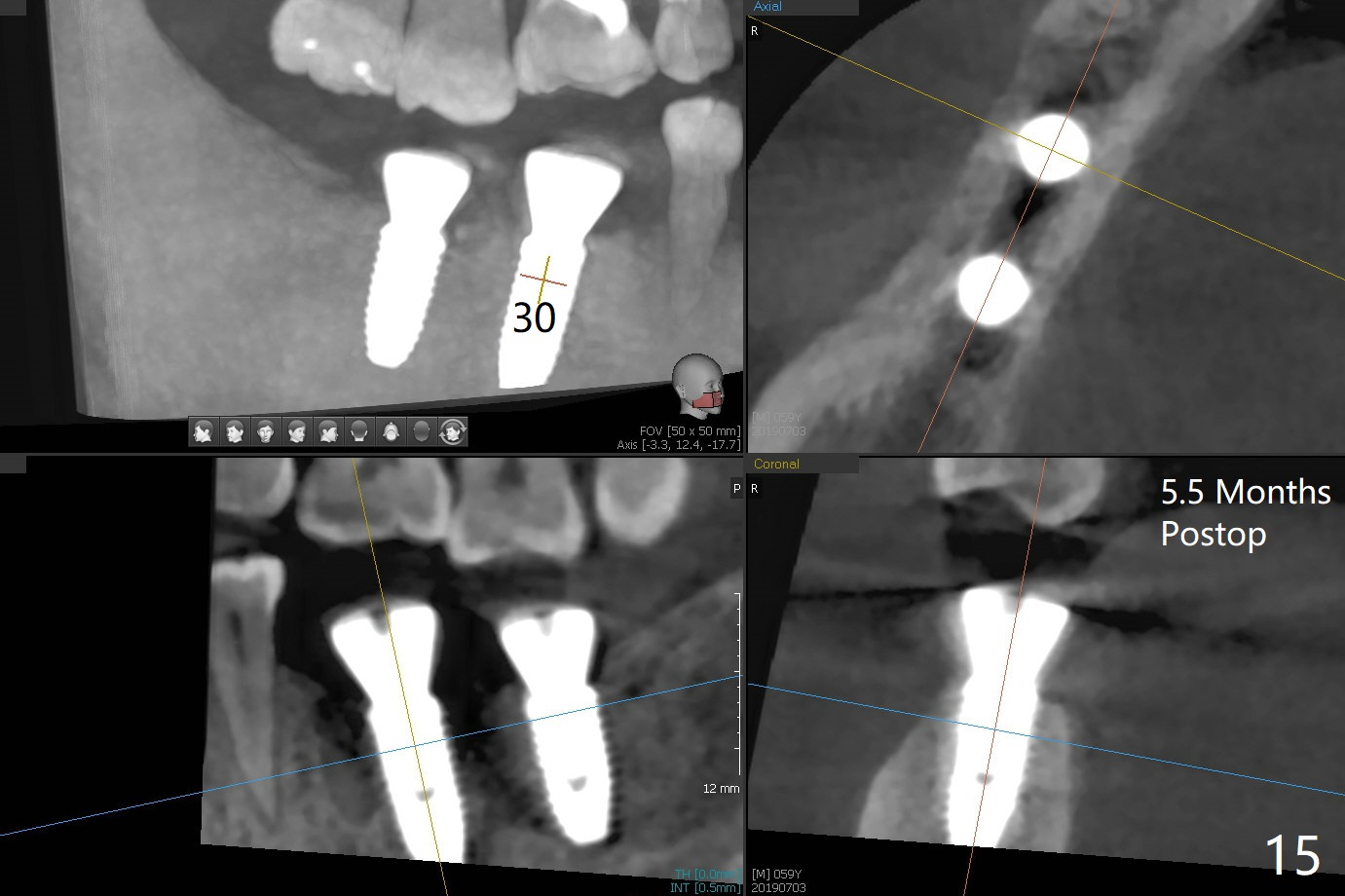
After extraction of the tooth #30 with lingual subgingival fracture (Fig.1), the septum is fairly large (Fig.2 S). A bony vertical anchor pin (Fig.3 *) is inserted in the septum following pointed drill to to stabilize the guide during osteotomy and implant placement of #31. When the latter is finished, a fixture anchor pin is used at #31 as planned. A healing abutment is placed at #31 because of supraeruption of the tooth #2 (Fig.4,5), while a cementation abutment is placed at #30 (Fig.5) with autogenous bone (from drills) and allograft placed around it (*, Fig.6). Finally an immediate nonfunctional provisional is fabricated to keep the bone graft in place (Fig.7 P). The bone graft remains in place gel-like nearly 1 month postop (Fig.8). CBCT axial section shows that there is not enough space for mini implant placement at the tooth #2 (Fig.9). Restoration-induced intrusion will be conducted using the implants at #30 and 31 three-4 months postop. The buccal gingiva (Fig.10 *) is lingual to the provisional (P) nearly 1.5 months postop. When the provisional is removed, it appears that the mesiobuccal bone graft has lost (Fig.11). Two days later, the cementation abutment is loose and removed; the gingival cuff looks healthy (Fig.12). A 6.8x5 mm healing abutment is placed (Fig.13). In 2.5 to 3 months, abutments will be placed at #30 and 31. Splinted provisional will be fabricated over supraocclusion to intrude the tooth #2 with a stop on the left side. Surprisingly the patient agrees to intrude the tooth #2 with 2 mini implants 5.5 months postop (Fig.14,15). However, the miniimplants dislodged. Due to coronavirus, the implants are restored with heavy abutment and opposing tooth trimming 1 year 9 months postop (Fig.16). Magicore should have been placed instead.
Return to
Lower
Molar Immediate Implant,
Prevent Molar Periimplantitis (Protocols,
Table),
Trajectory,
Weichat
2Xin Wei, DDS, PhD, MS 1st edition
01/14/2019, last revision
10/15/2020