

,%20Vanilla.jpg)
,%20Vanilla.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Push Septal Gingiva Palatal
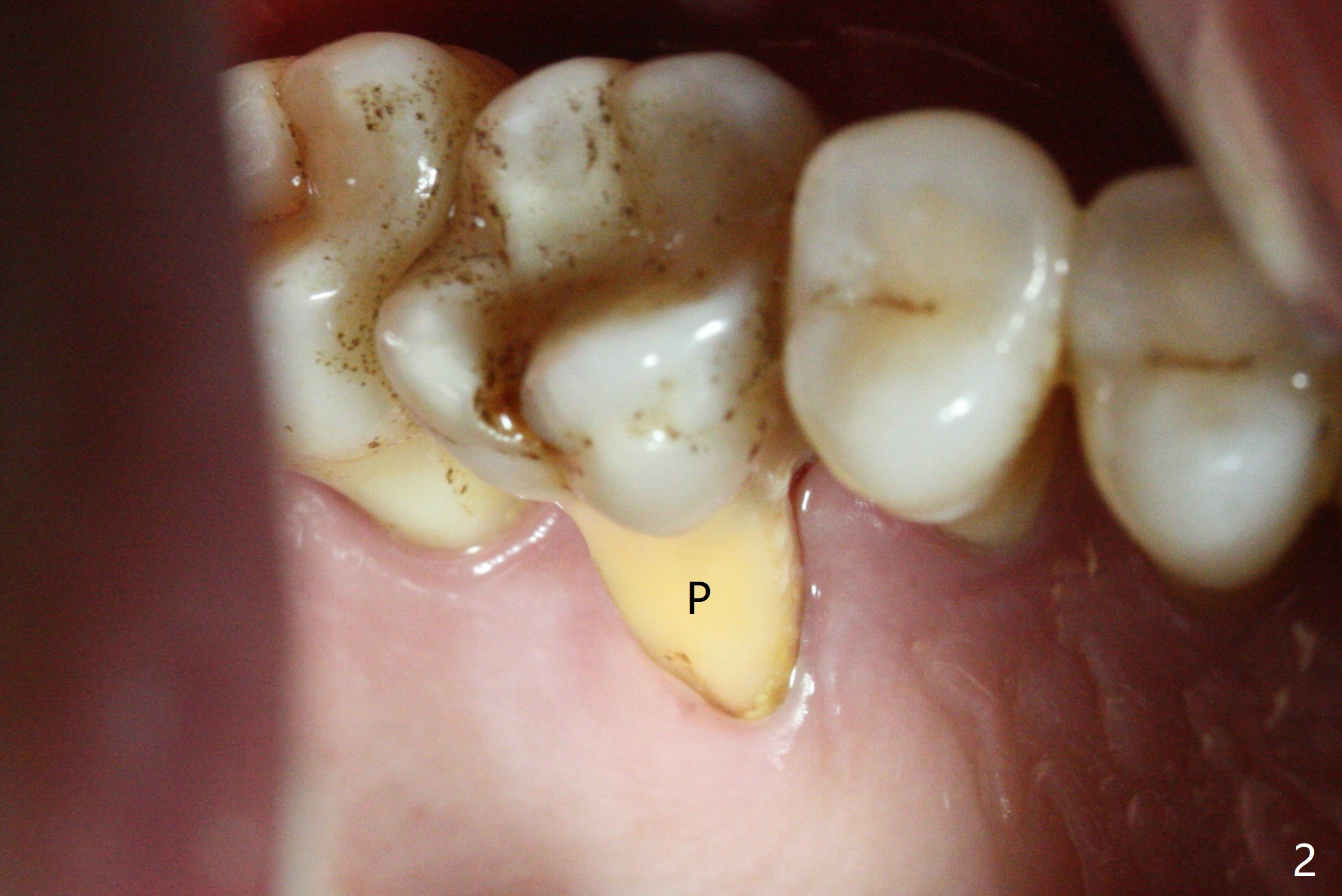
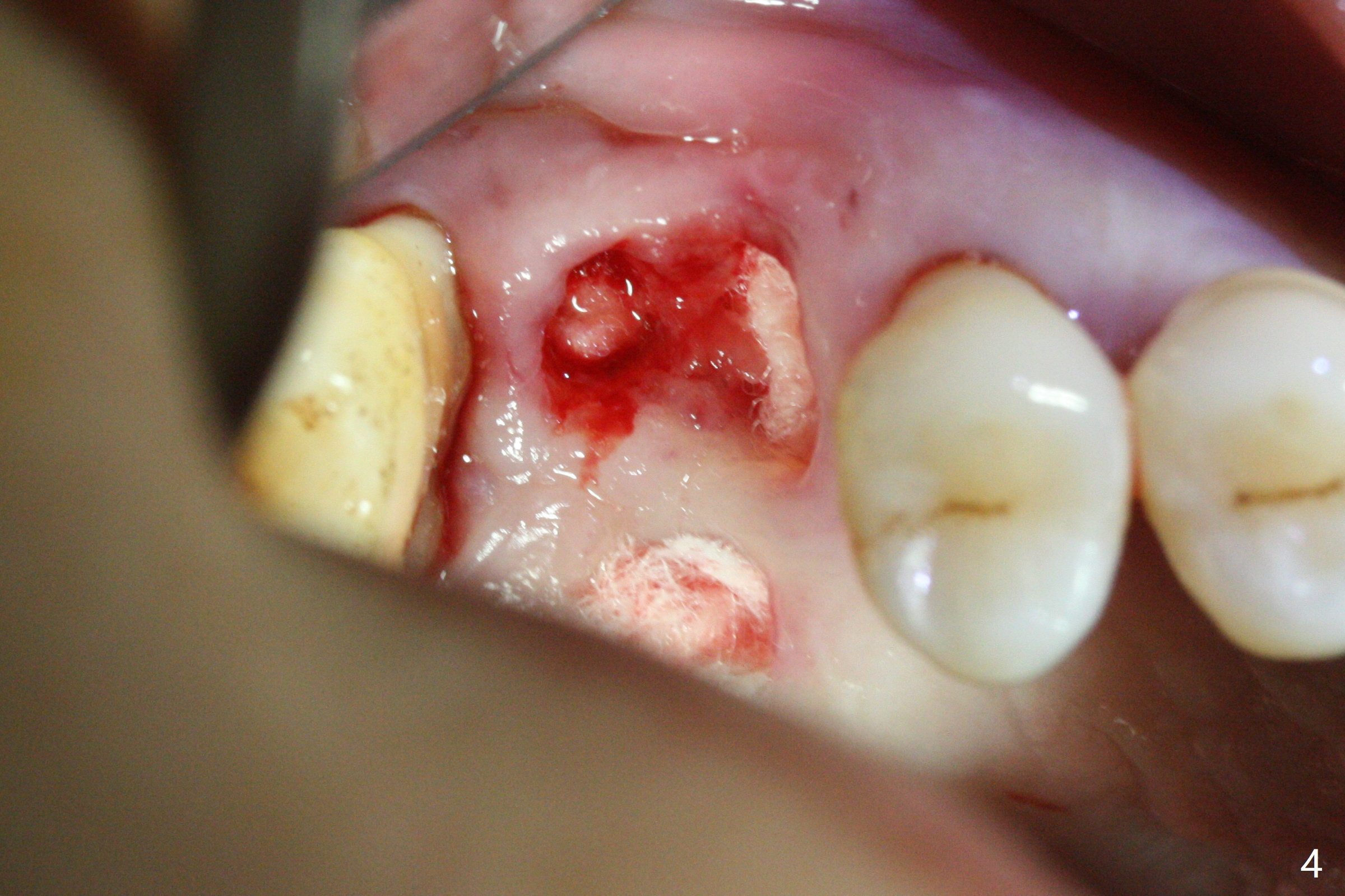
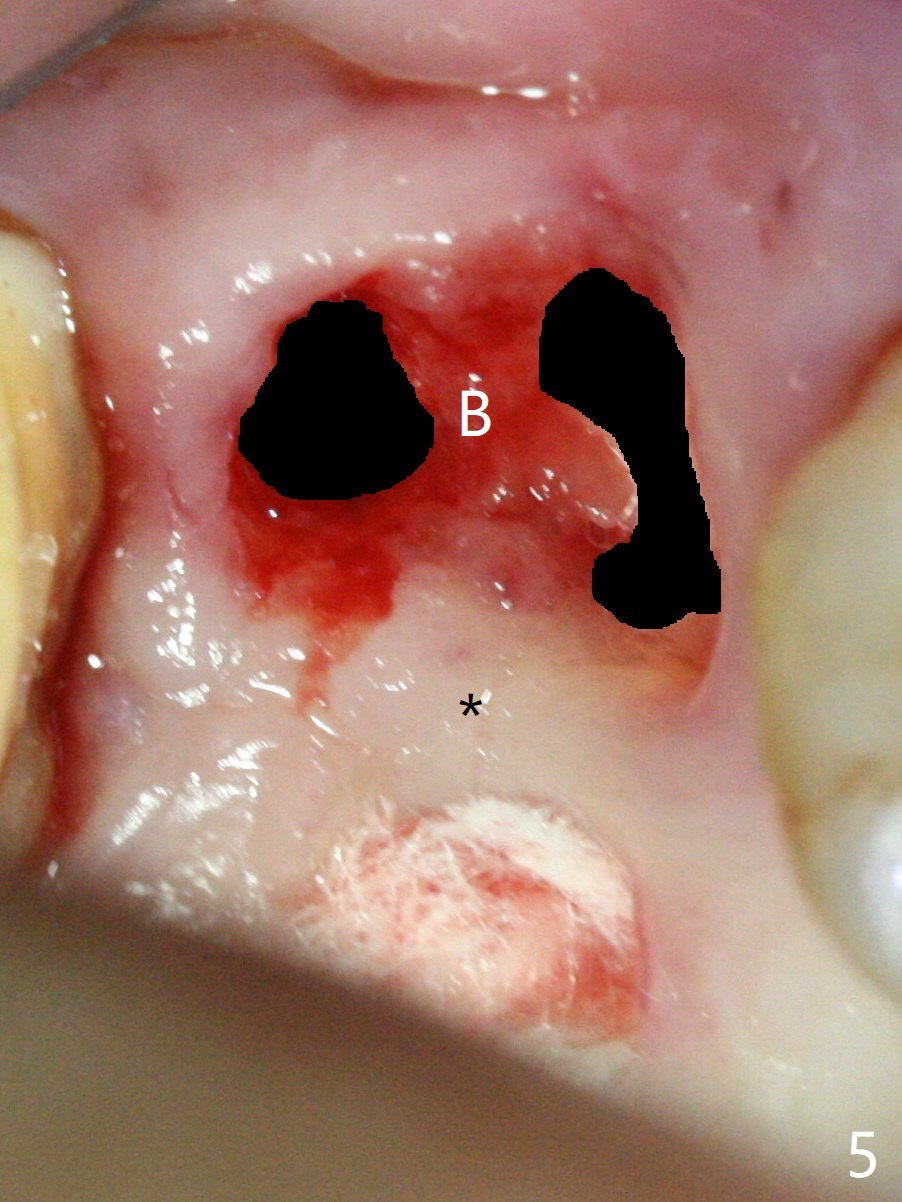
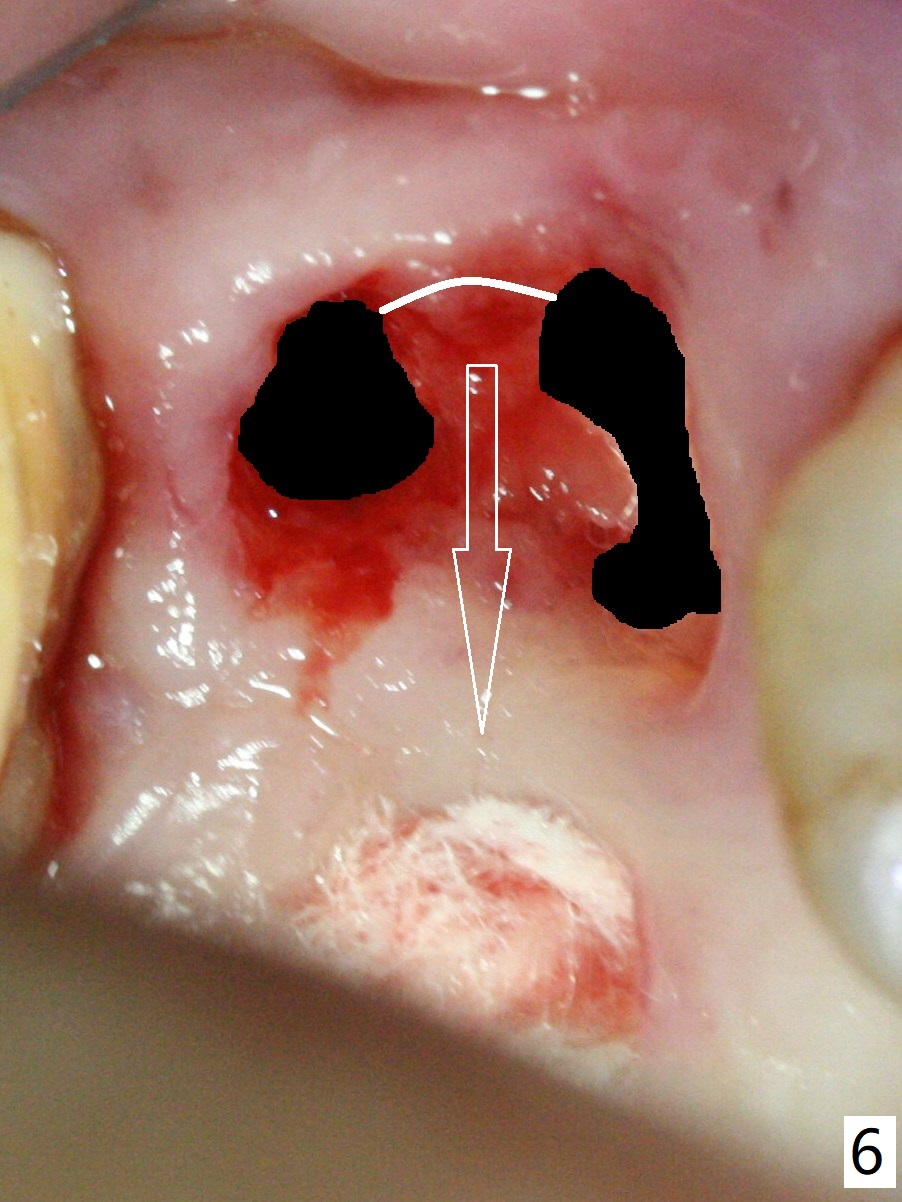
The tooth #3 has gingival recession moderate buccally (Fig.1) and severe palatally (Fig.2 P). The remaining bone height is estimated 4 mm (Fig.3). After extraction and debridement, the 3 sockets are packed with 2% Lidocaine 1:50,000 Epinephrine saturated gauze (Fig.4). When the gauze is removed from the buccal sockets (Fig.5 black area), the buccal portion (B) of the septal gingiva (*) is sectioned from the buccal gingiva (Fig.6 curved white line) and elevated from the underlying septal bone and pushed palatally (arrow). The septal gingiva (including the buccal portion) will be the palatal soft tissue wall of the subsequent osteotomy, providing blood supply to allograft to be placed. In short, the septum (through the buccal socket) will be the osteotomy site.
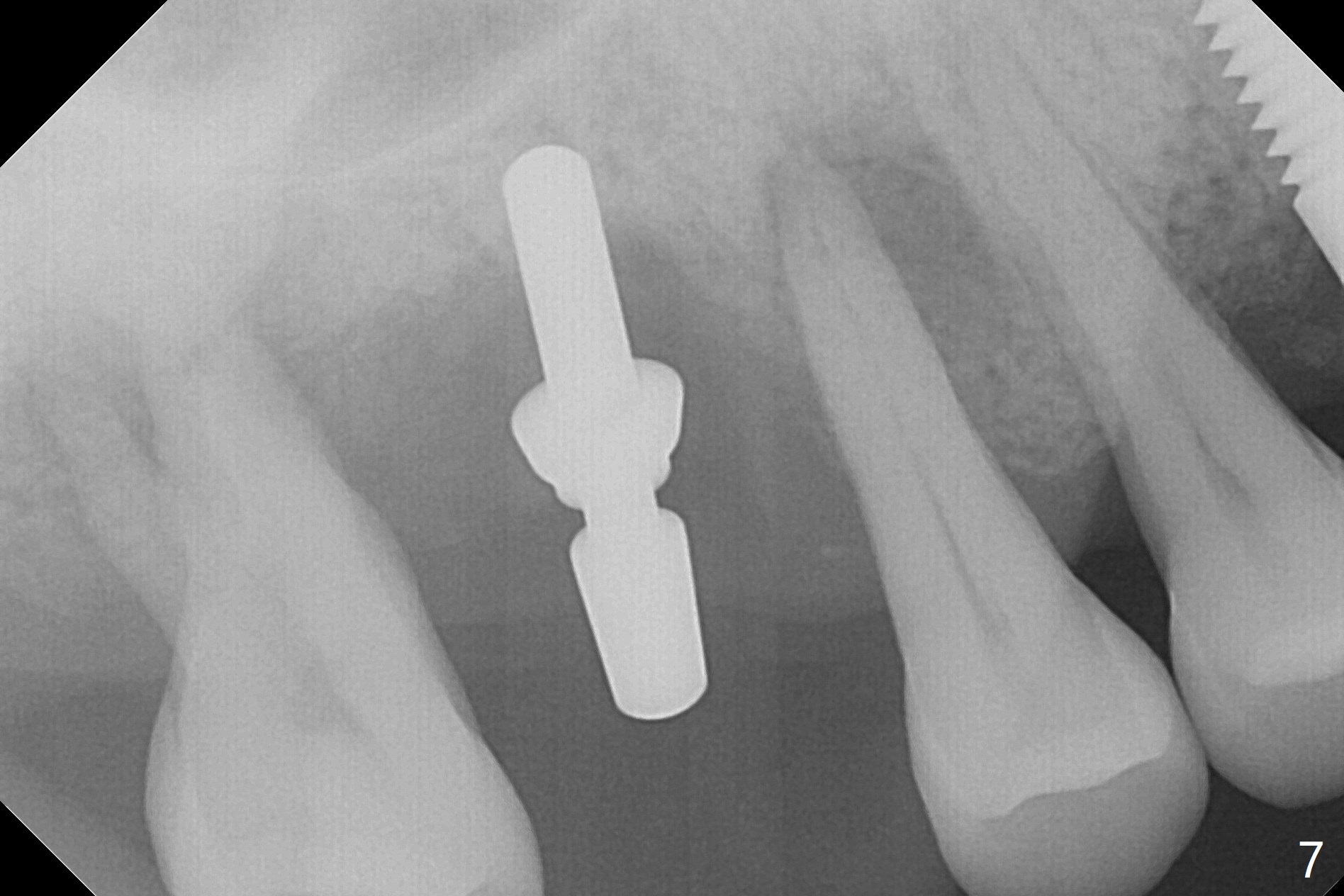
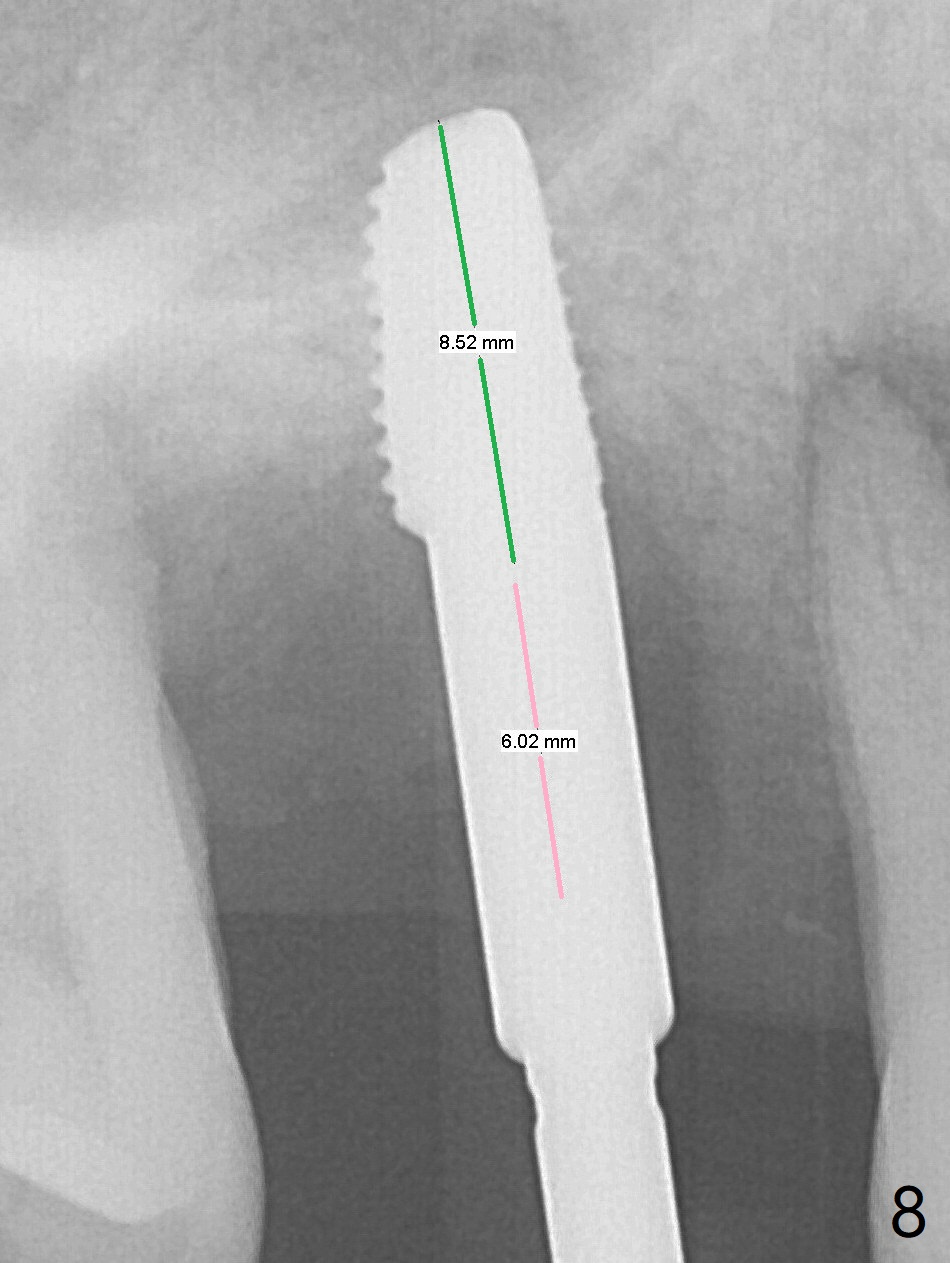
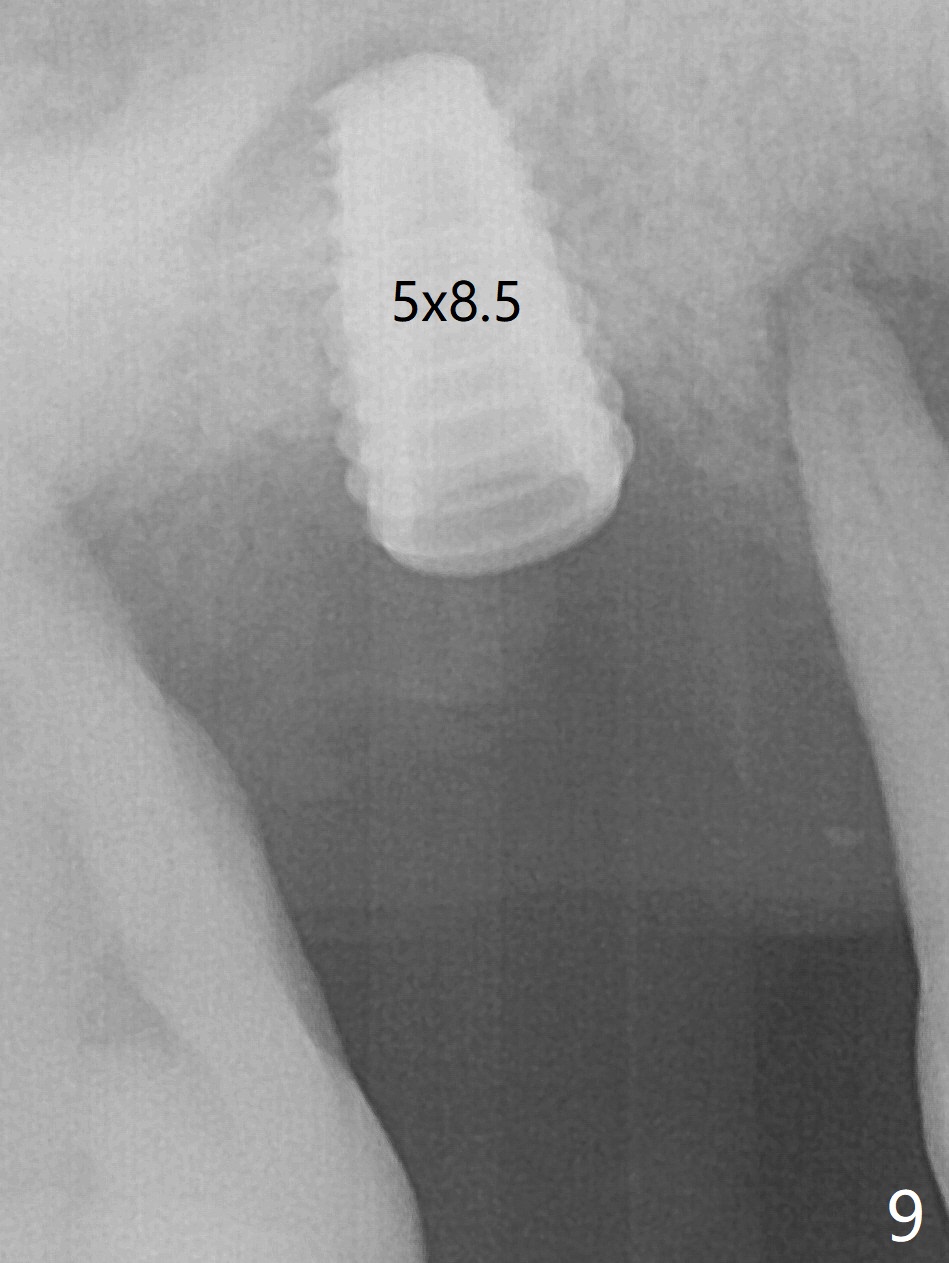
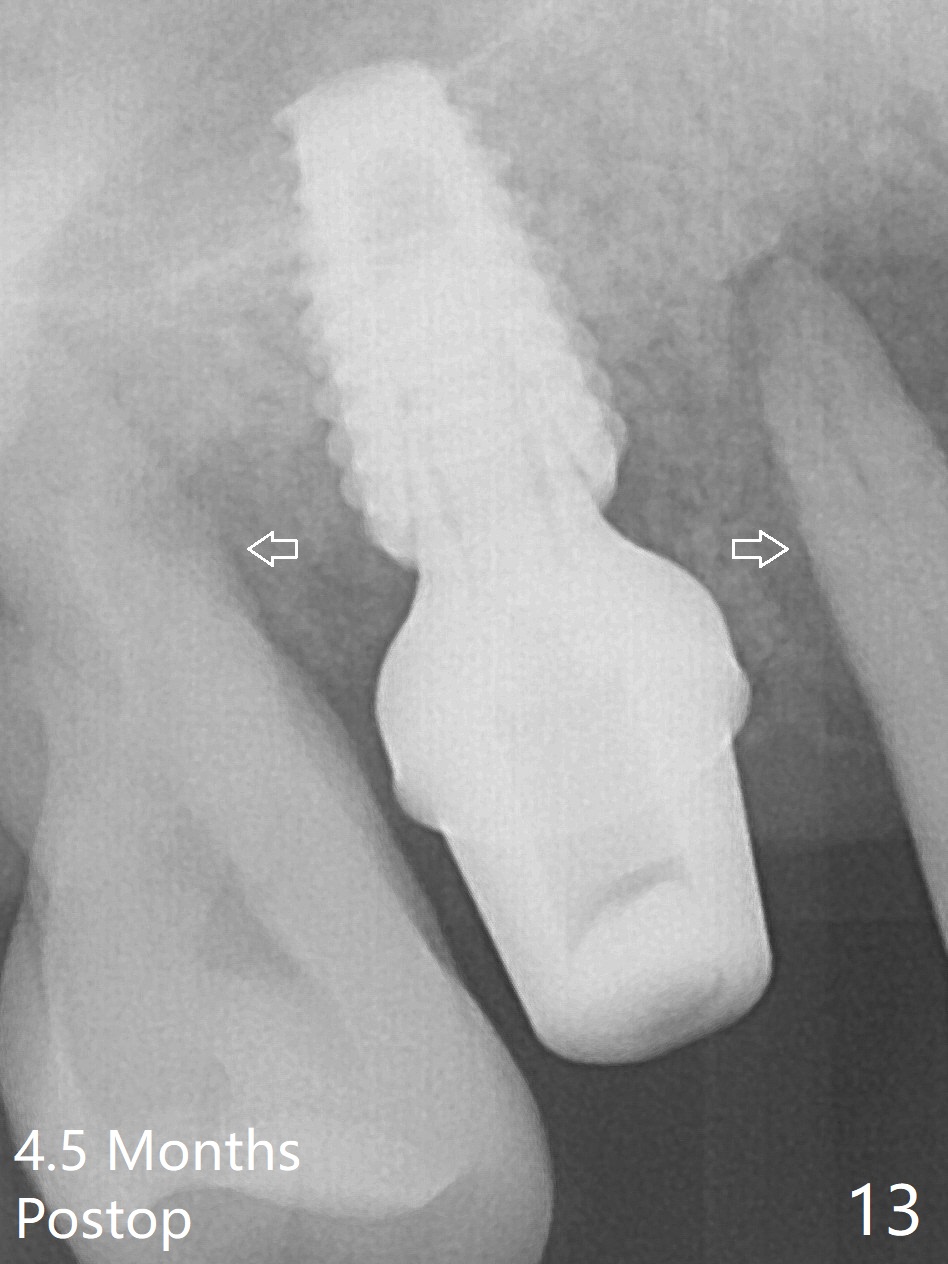
Initial osteotomy depth is 4 mm (Fig.7). The sinus membrane is found to be perforated when the depth increases to 8 mm. The latter could be prevented by taking CT and/or using osteotome. The subsequent osteotomy depth is 5 mm until 4.0 mm in diameter. When the 4.5 mm tap is inserted with initial stability, the shortest implant (8.5 mm, Fig.8 green) will be partially protruded into the sinus and partially exposed in the socket and the cuff of the abutment is expected to be around 6 mm (pink). Since the 5 mm tap achieves primary stability, a 5x8.5 mm implant (following placement of Osteogen plug to repair the perforated sinus membrane) is placed at the level just mentioned (Fig.9). Vanilla Graft mixed with minimal autogenous bone is packed (Fig.10.11 *) before and after insertion of a 6.5x5(4) mm abutment. An immediate provisional as well as a piece of Osteogen plug is fabricated to close the socket gap. The provisional and the abutment are dislodged 1 month postop (Fig.12). The wound has healed. The abutment is reloaded without the provisional. The implant appears to osteointegrate 4.5 months postop (Fig.13); in addition the bone graft seems to have migrated toward the roots of the neighboring teeth (arrows).
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
Armaments,
6
14
2
Xin Wei, DDS, PhD, MS 1st edition 03/05/2018, last revision 03/10/2019