

|
|
|
|
|
|
||
Hemorrhage In Socket Preservation
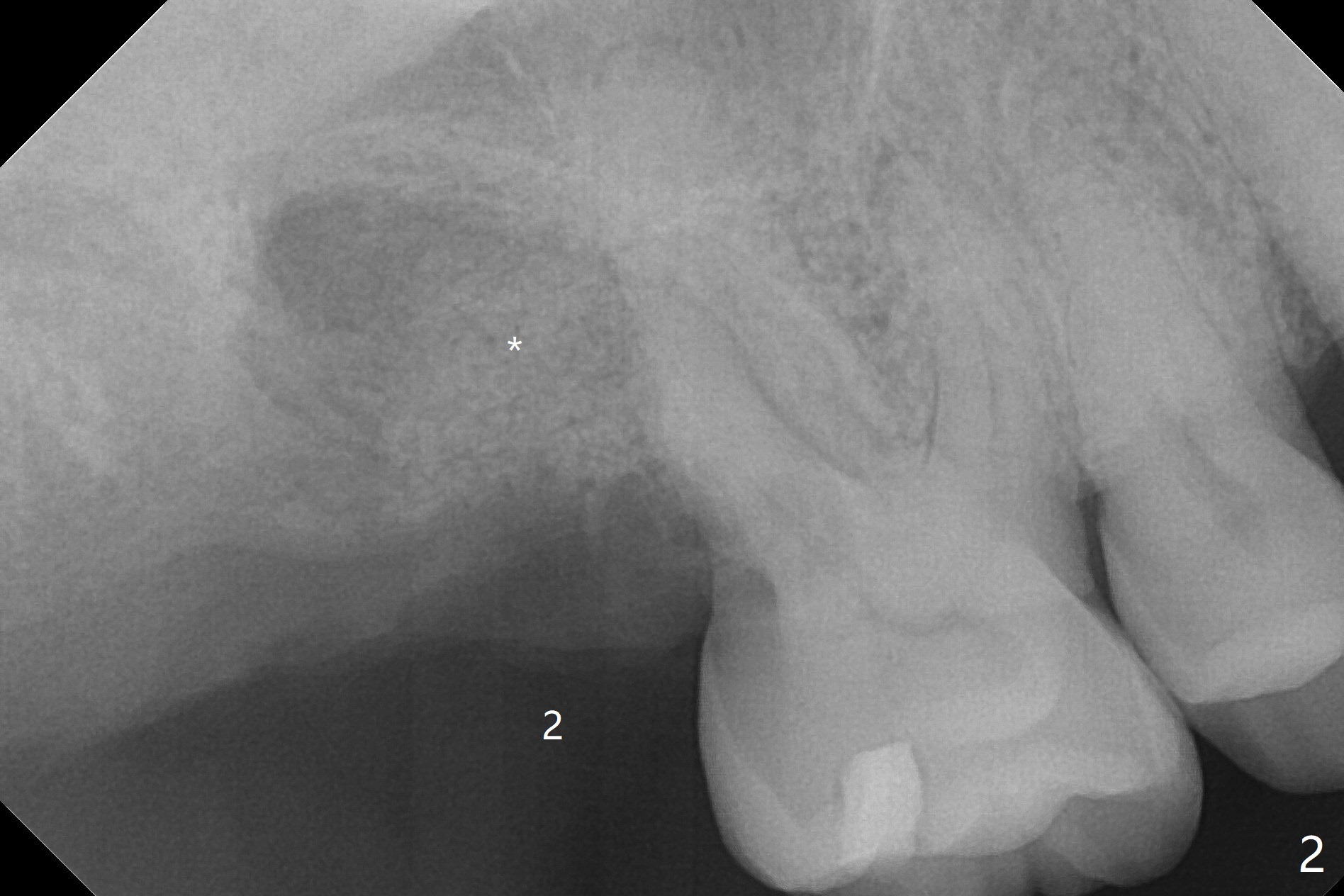
A 55-year-old man agrees to have the tooth #1 extraction immediately post SRP. Pre-extraction panoramic X-ray shows severe bone loss at #2 (Fig.1). Possible extraction of #2 is mentioned considering pending implant at #14. Extraction of #1 turns out to be difficult, requiring sectioning. The tooth #2 blocks the access. The patient readily accepts #2 extraction. Removal of abundant granulation tissue at #2 is associated with severe hemorrhage from the Greater Palatine Vessels. After pressure hemostasis, a piece of Osteogen Plug is placed at #1, the other palatal of #2 to control hemorrhage. With hemostasis, Vanilla graft is placed at #2 securely (without being washed out, Fig.2 *), followed by placement of a third Osteogen Plug on the top of the graft. The last surgical challenge is to close these two large wide sockets with 4-0 Chromic gut and PGA. While the socket #1 remains closed, the one at #2 is open 13 days postop (Fig.3). It appears that a stiffer membrane (6-month) should be sutured in place to keep the Osteogen plug underneath in place. The latter seems to be easily fragmented.
Return to Upper Molar Immediate Implant, Trajectory II Xin Wei, DDS, PhD, MS 1st edition 10/23/2019, last revision 04/14/2020