








|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|||
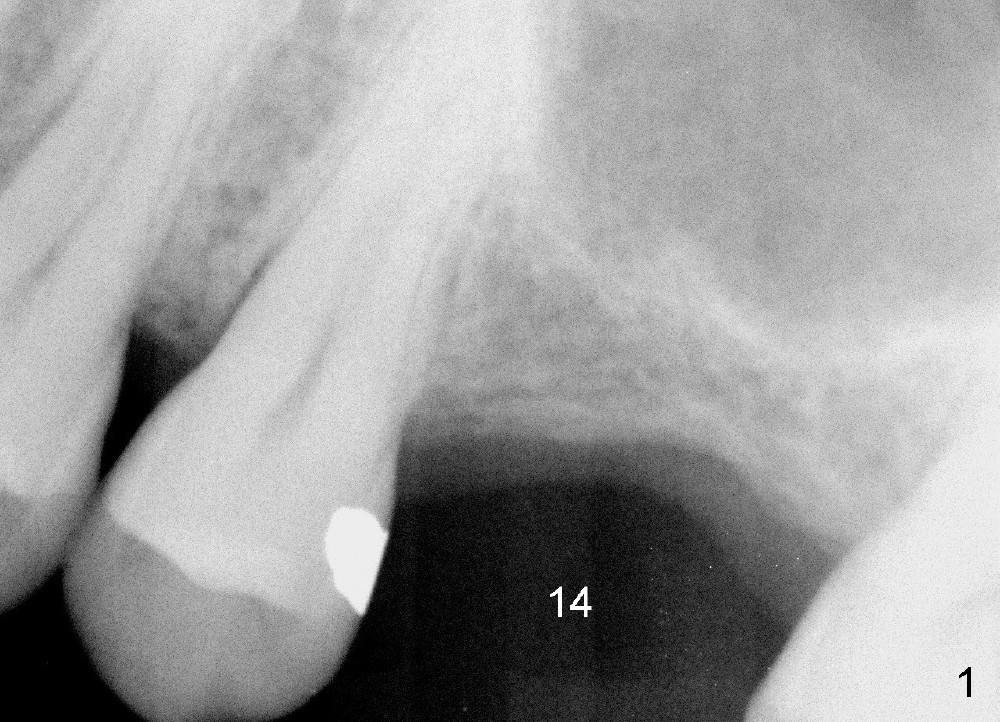
Extra wide Implant for Limited Height
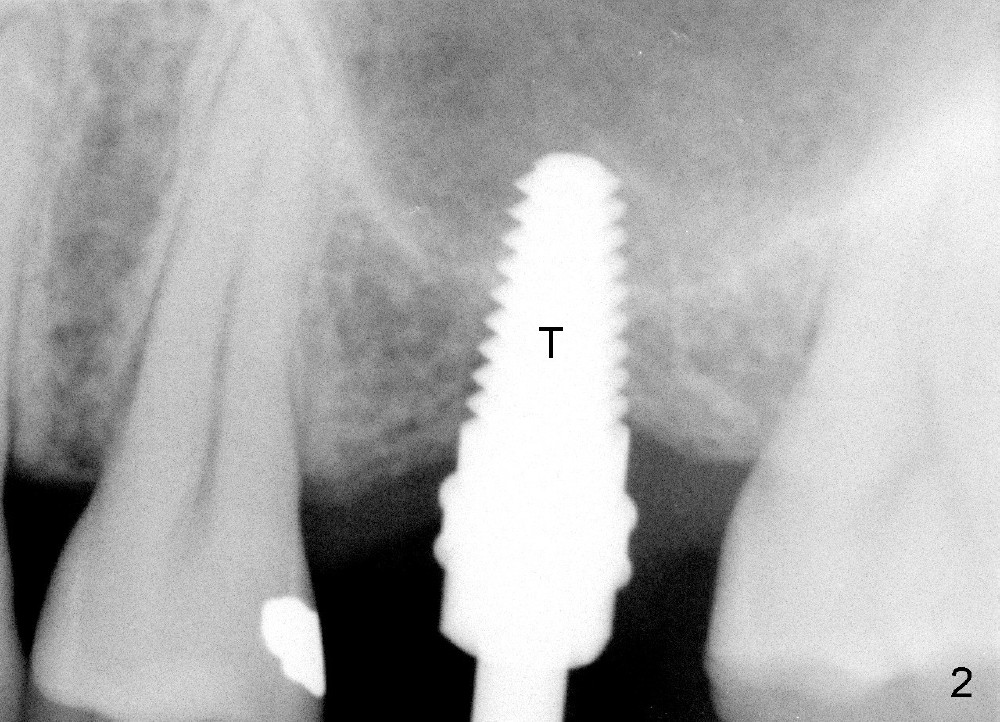
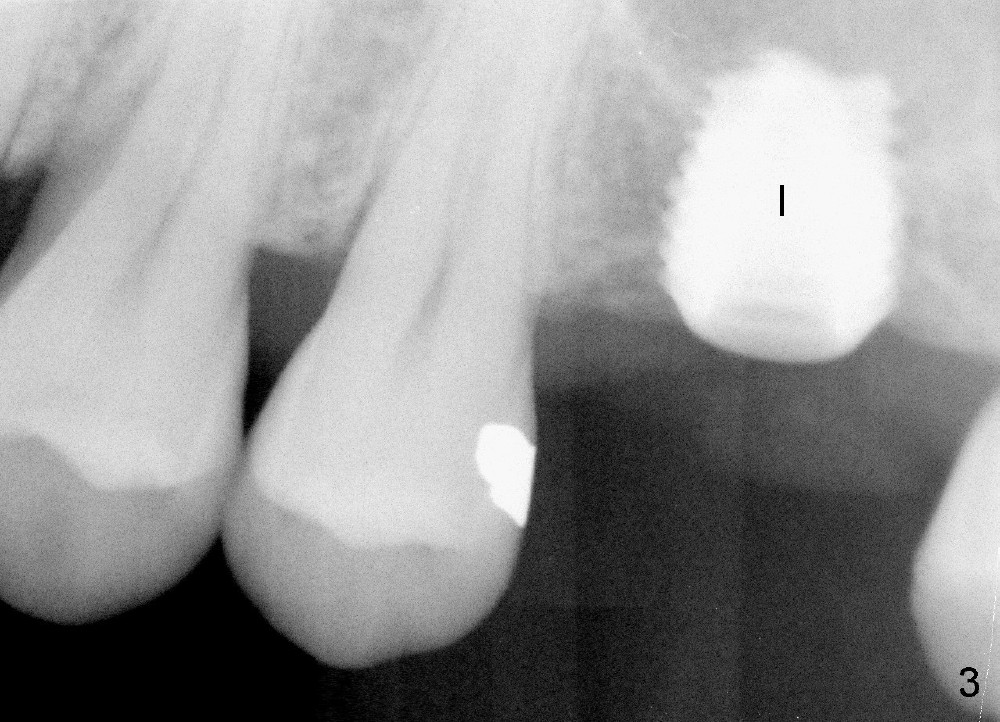
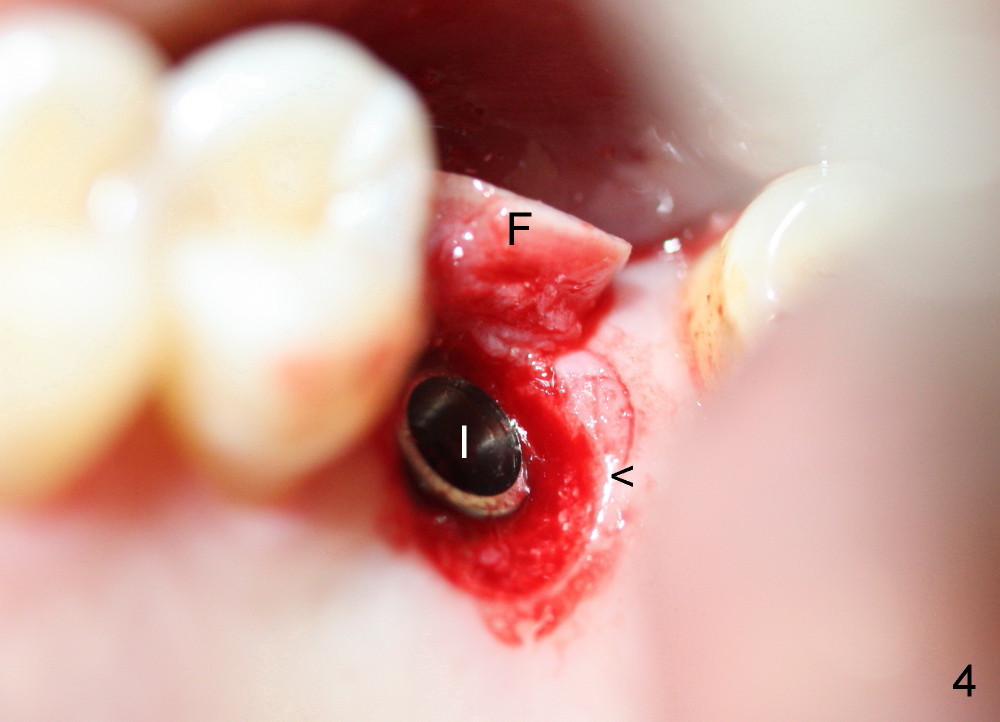
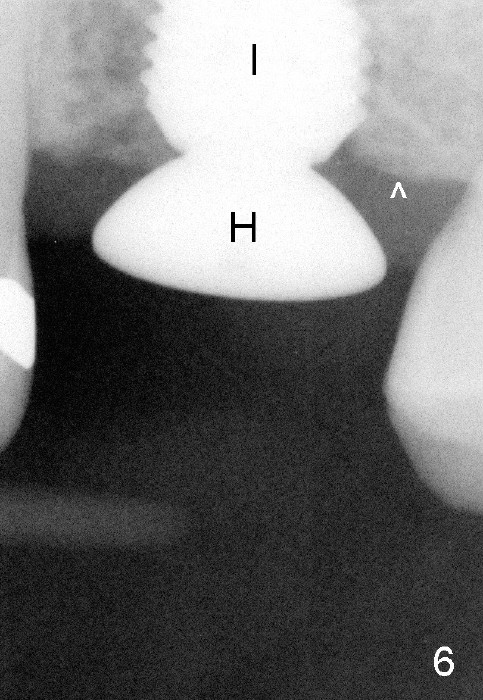
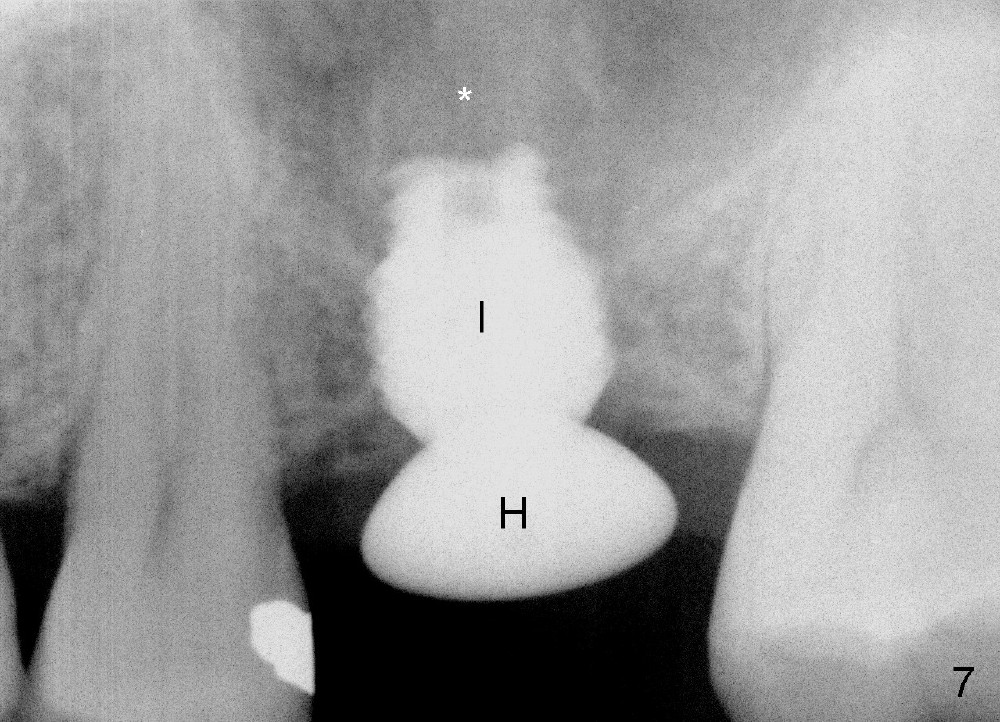
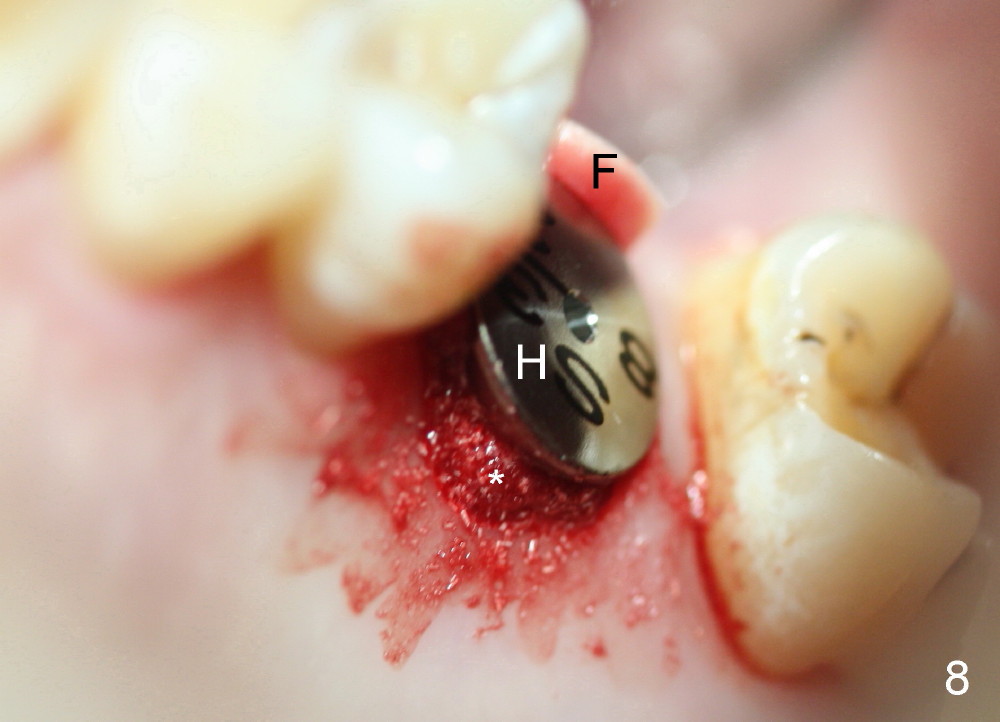
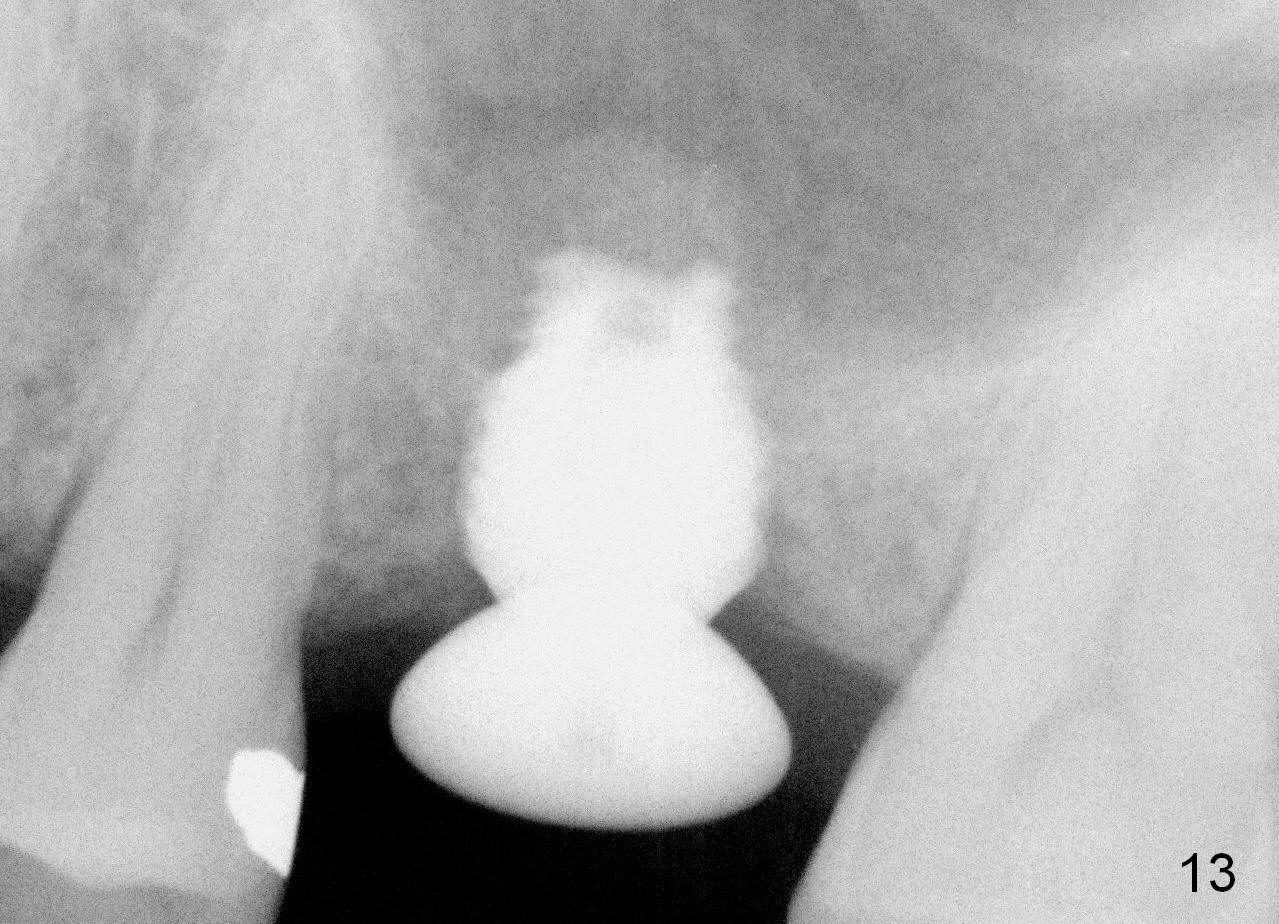
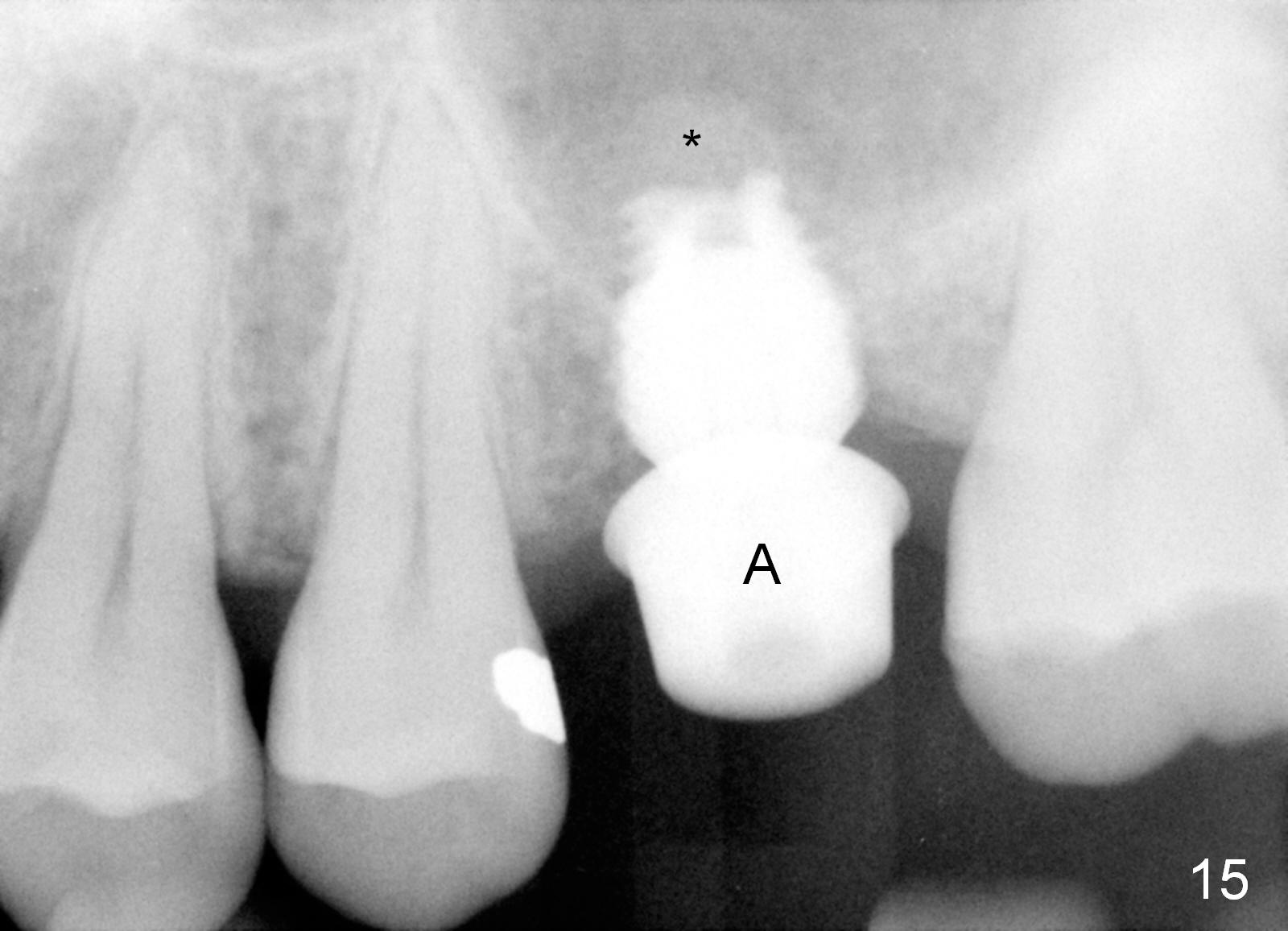
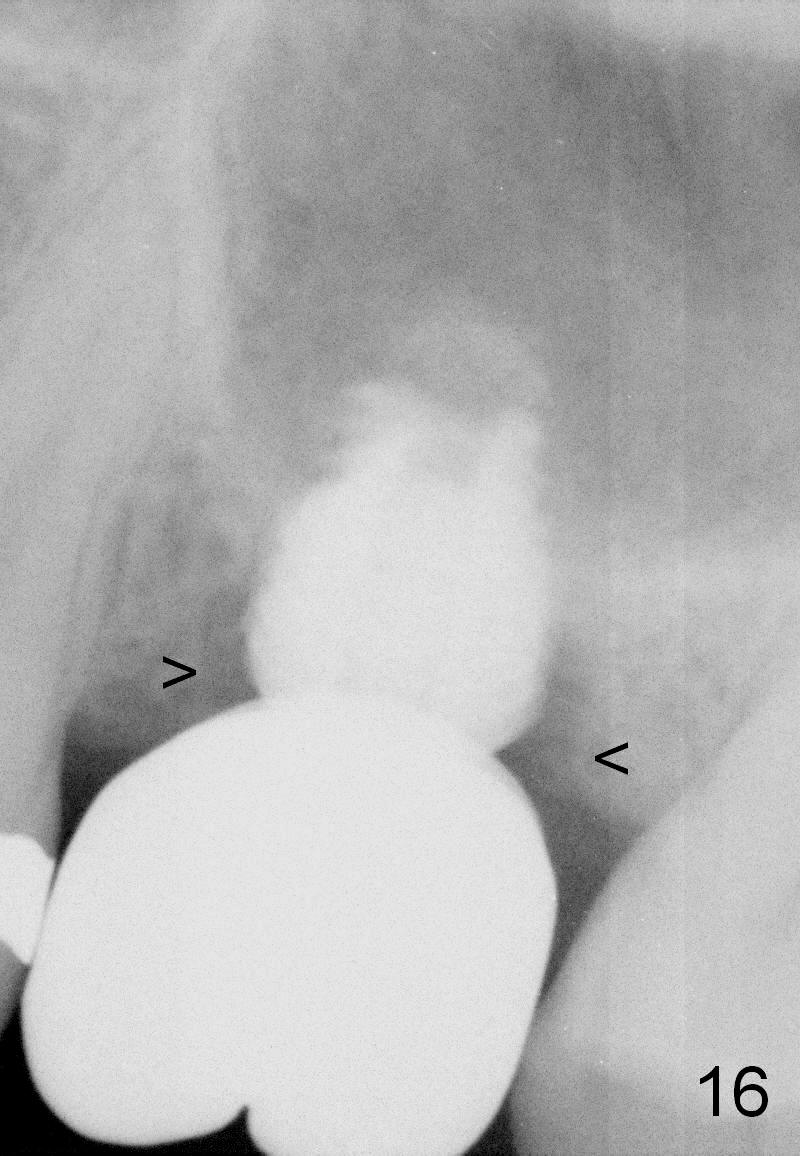
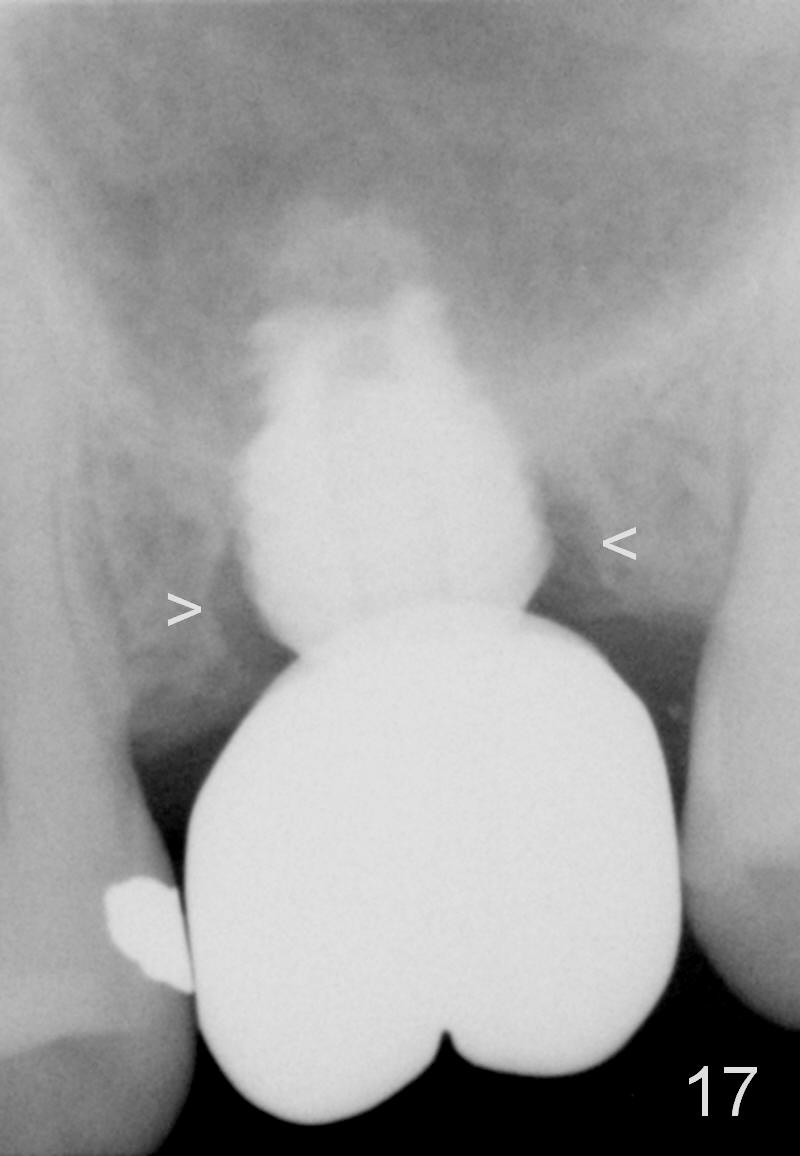
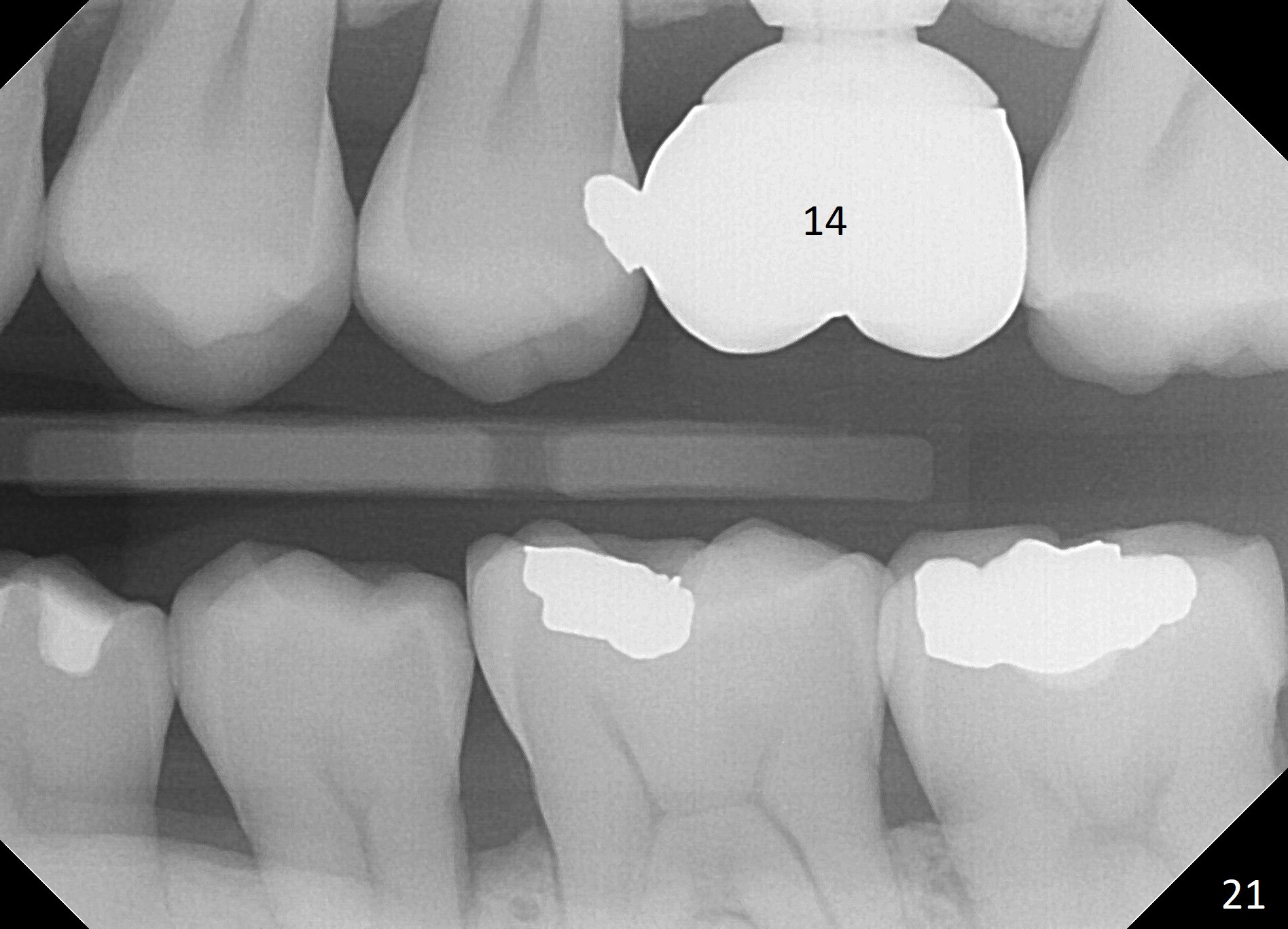
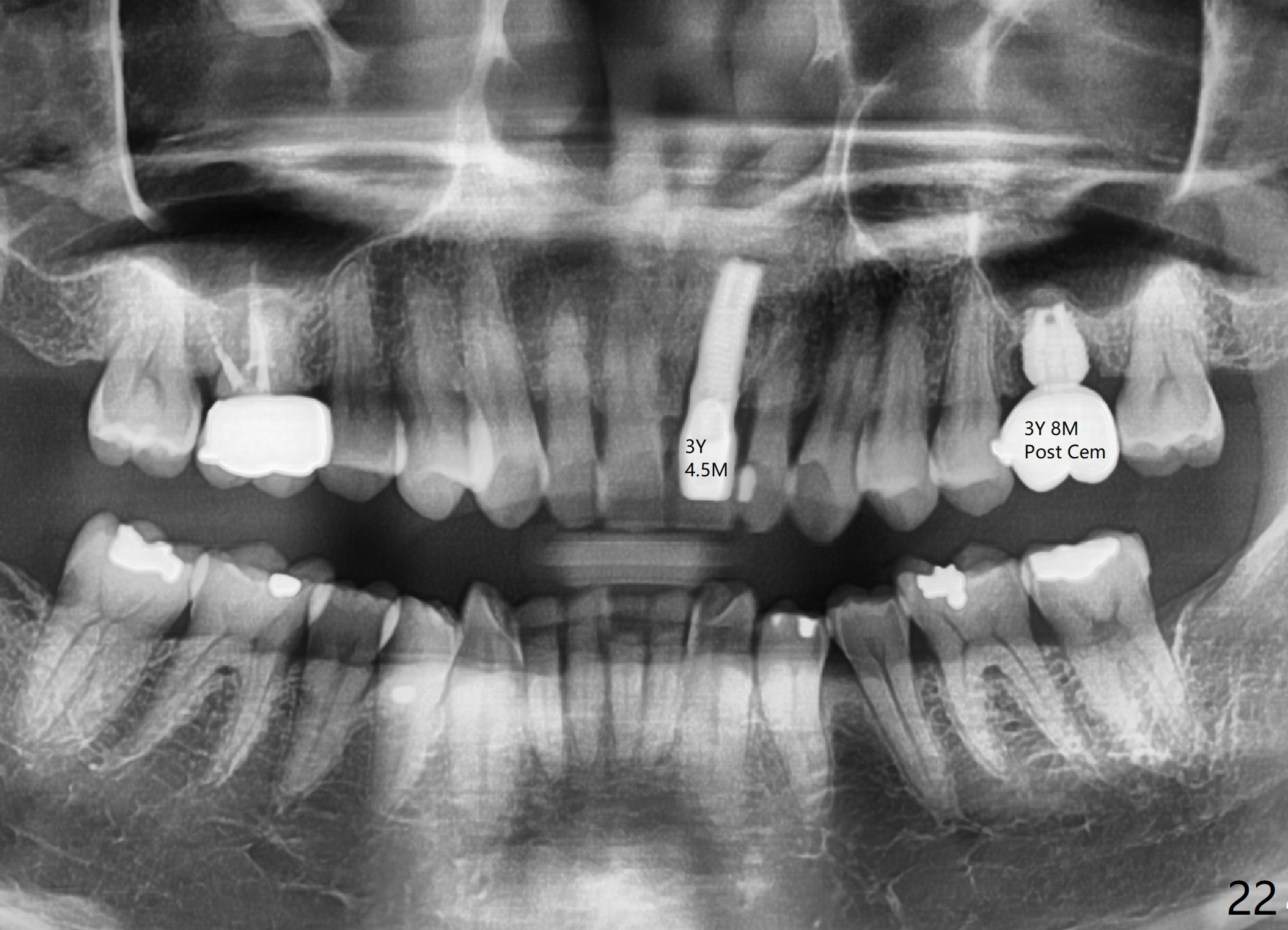
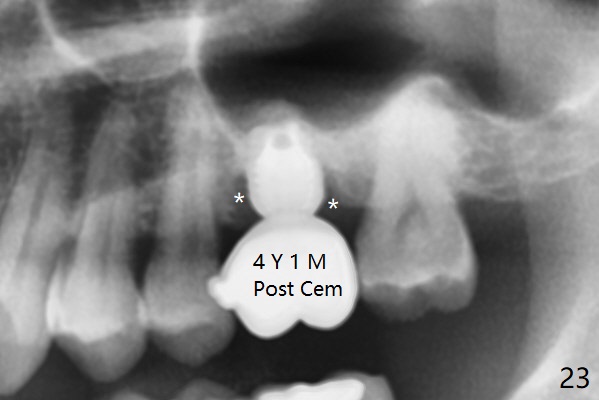
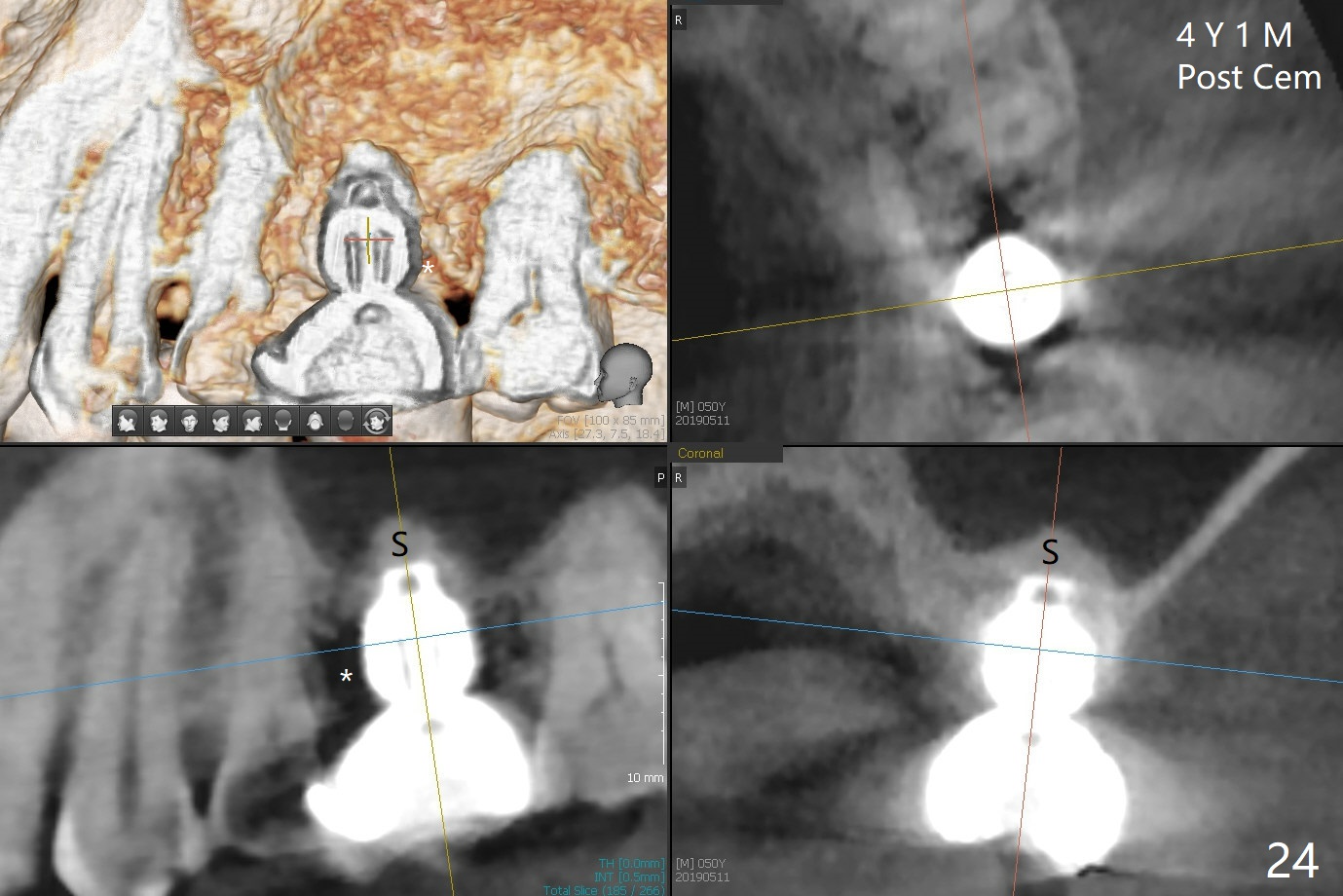
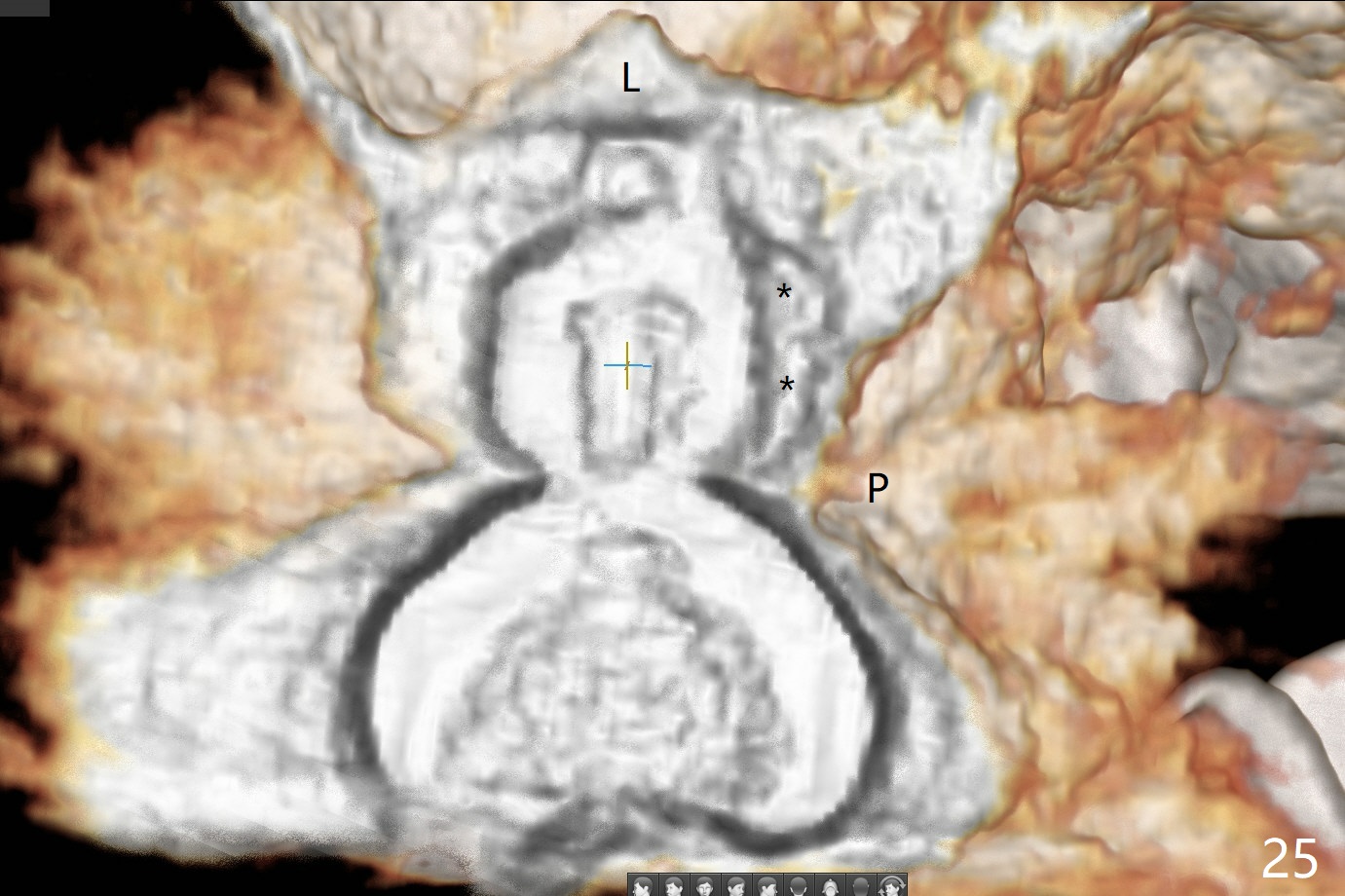
A 45-year-old man has lost the tooth #14 for a while (Fig.1); bone height is 5.4 mm. An extra wide and short implant is planned. Torus palatinus is large, suggesting that bone density should be high. A 6 mm tissue punch is chosen, but it is placed more palatal. If it were placed in the middle of the ridge, there would be no buccal keratinized gingiva (incision may avoid this issue). Additionally, the buccal portion of punch is made incomplete so that there is pedicle on the buccal side when the flap is raised (Fig.4,8: F). It is expected that the excess portion of keratinized tissue will form thick gingiva buccally. Osteotomy proves that bone is dense (Fig.2 (4.5x11 mm tap). Typical sinus lift is finished with placement of 6.4x6 mm (extra wide) bone-level implant (Fig.3, >55 Ncm). Following further torque, Fig.4 shows that the implant (I) is sub-gingival (<). Bitewings are taken to confirm that the implant plateau is at the crestal level (Fig.5,6 ^). PA shows sinus lift (Fig.7 *). The lingual aspect of the implant and healing abutment (H) is further bone grafted and covered by collagen dressing (Fig.8 *). The wound is protected with perio dressing. When the latter dislodges 7 days postop, the collagen dressing and bone graft are lost as well (Fig.10), while the buccal flap remains vital (Fig.9). The lingual exposed plateau should be able to heal normal. The collagen dressing should have been fixed in place by suture or as simple as a dental floss. There is mild nasal hemorrhage 1-2 days postop, possibly related to sinus membrane perforation and inability of Collagen Dressing to cover the perforation and contain the bone graft. When the patient returns for #9 implant placement in 3 weeks postop, the buccal flap reduces in size (Fig.11 *), while the palatal wound has healed with minimal exposure of the implant (Fig.12). Sinus graft remains in place 3 months postop (Fig.13); the buccal flap appears to have incorporated into a part of the gingiva (Fig.14). The bone density of the sinus lift appears to increase 10 days later when an abutment is placed (Fig.15 *). Although oral hygiene is pristine, there is apparent crestal bone resorption 12 months (Fig.16) and 20 months (Fig.17) post cementation, probably due to unfavorable crown/implant ratio and bruxism as well as pre-implantation bone loss (Fig.18,19). In contrast, an immediate implant in the same patient avoids pre- or post-implantation bone loss. In fact both the soft (Fig.20) and hard (Fig.21) tissues remain healthy 2 years 8 months post cementation. The sinus lift remains 3 years 8 months post cementation (Fig.22), while the crestal bone loss persists. The patients keeps complains of food impaction distal associated with bad smell 4 years 1 month post cementation. In fact the distal proximal contact is within normal limit. The bad smell is probably due to crestal bone loss (Fig.23 (pan), 24 (CT) *) and periimplantitis. Bone graft, PRF and Cytoplast membrane will be needed and fixed in place with long healing screw. When the patient returns for crown redo, he also reveals floss related gingival hemorrhage. There is pain associated with palatal sulcus probing with light gingiva erythema. Review of CT coronal section shows possible palatal (Fig.25 P) bone loss (*).
Return to Professionals,
Sinus Lift,
Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 11/18/2014, last revision 05/21/2019