|
|
|
|
|
|
Bilateral Engagement
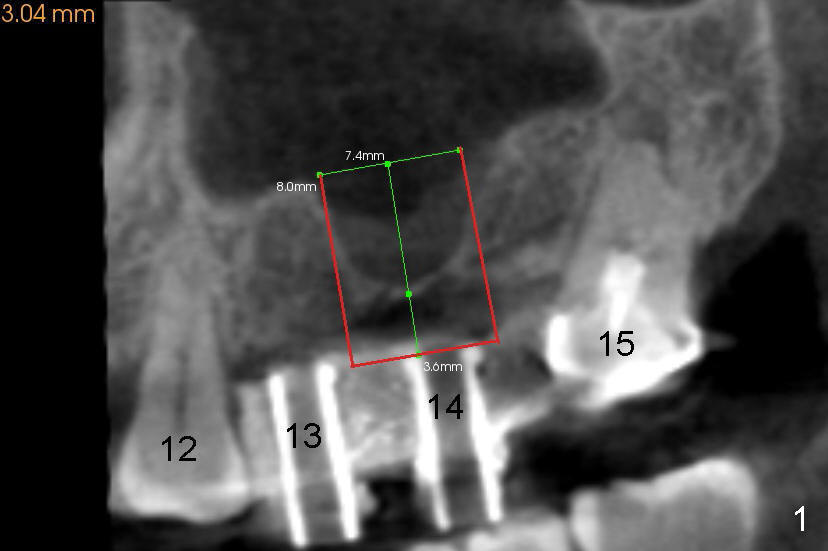
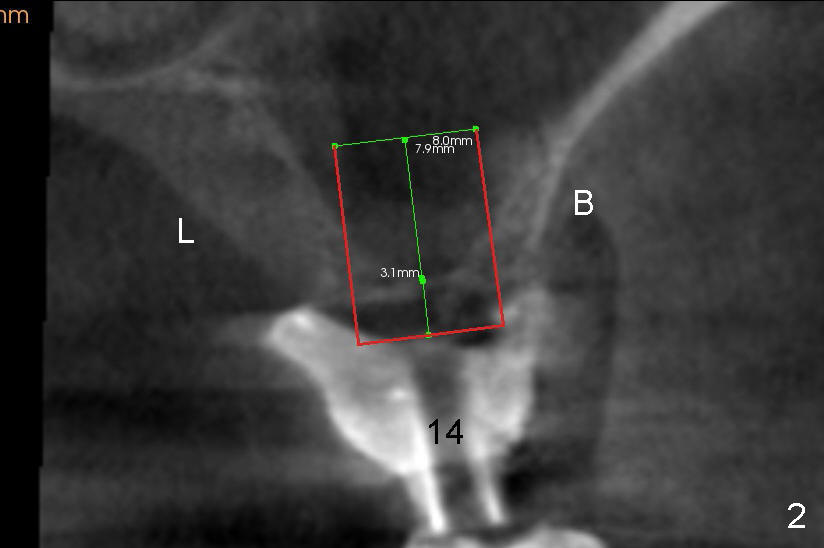
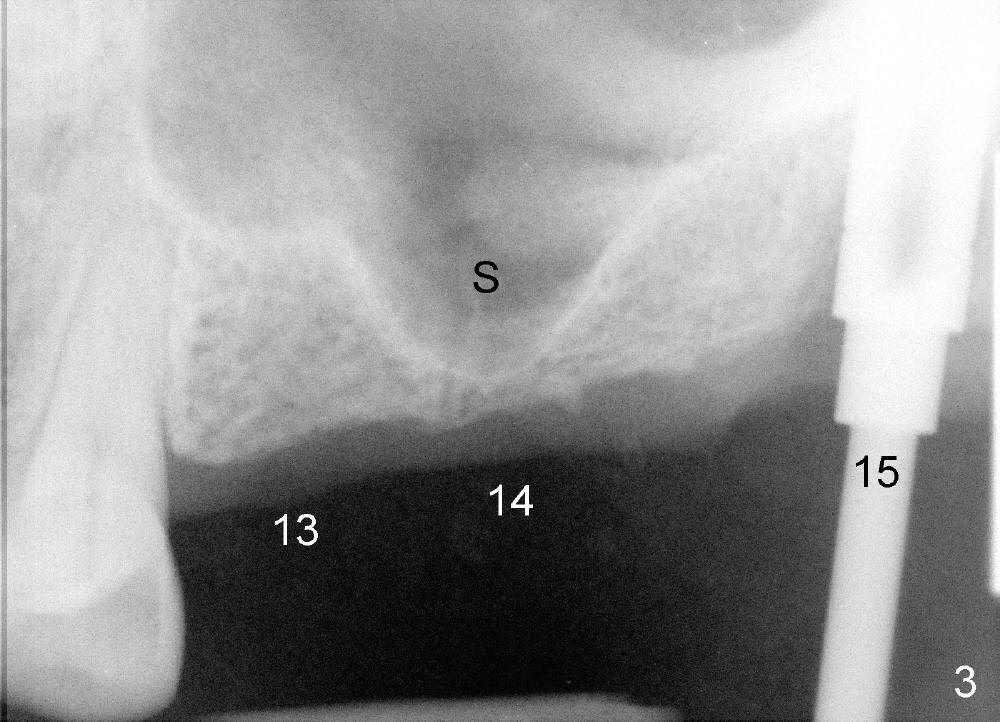
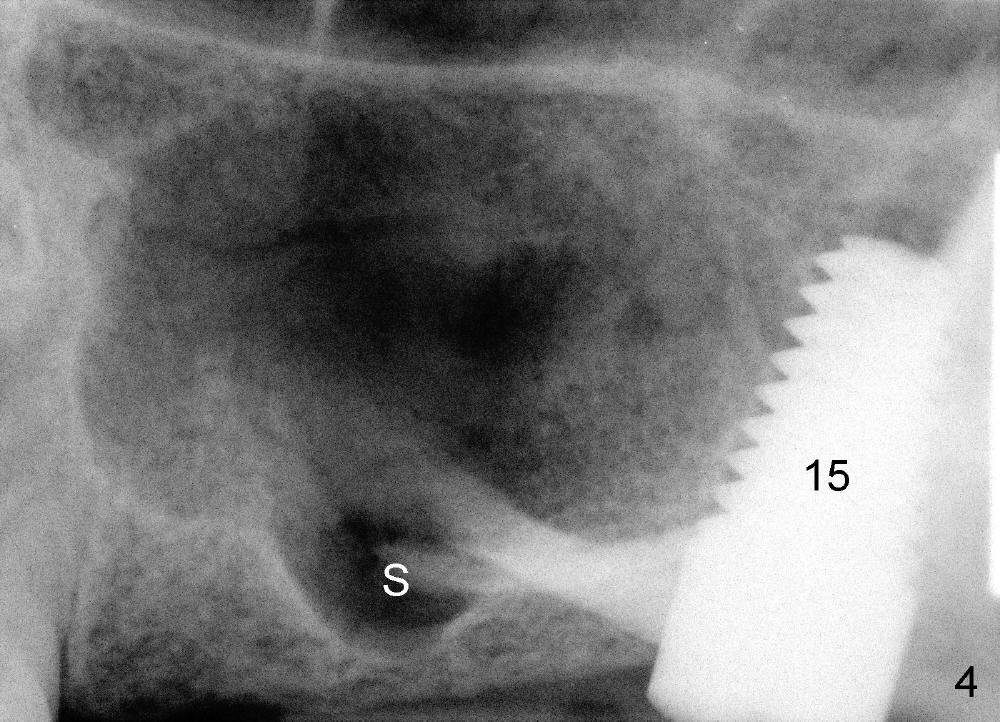
The two cases we discuss early appear to show that implants at the first molar are placed to engage in the mesial aspect of bone to have primary stability (1,2). But sometimes sinus floor may be right above the first molar (Fig.1-4). Fig.1 (CT sagittal) and 2 (coronal) were taken before #15 extraction, whereas Fig.3, 4 (PA) were taken during and immediately after extraction, respectively. A tapered 8x17 mm implant was placed at the site of #15.
In order to get primary stability, it is apparent that a large screw implant should be placed (Fig.1,2: 8x11 mm) to engage all of the lateral walls of the concave sinus floor (mesial and distal (Fig.1), buccal and lingual (Fig.2 B, L). Three millimeter shorter implant may be more appropriate (8x8 mm) in term of being less traumatic.
In fact, sinus graft has been tried without success (sinus membrane torn, buccal wall difficult to penetrate). The patient refuses to an offer to get a second trial by an expert such as Drs. Borgner and Dunson. Sinus lift appears to be more acceptable.
It is presumed that the concave sinus floor forms after extraction. In fact, it may be not completely true.
Return to Professionals
Xin Wei, DDS, PhD, MS 1st edition 04/26/2013, last revision 04/28/2013