|
|
|
|
|
Single Drill
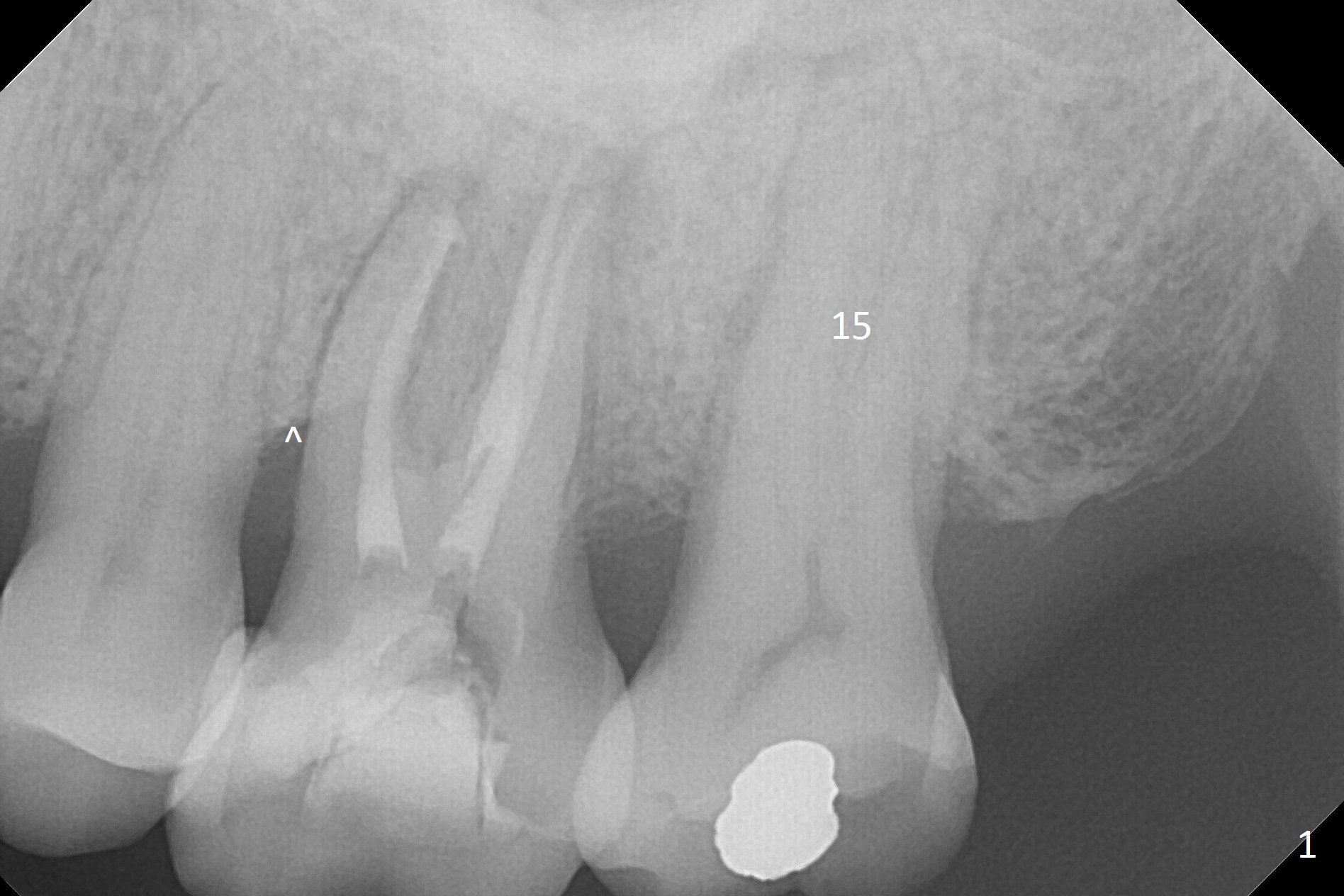
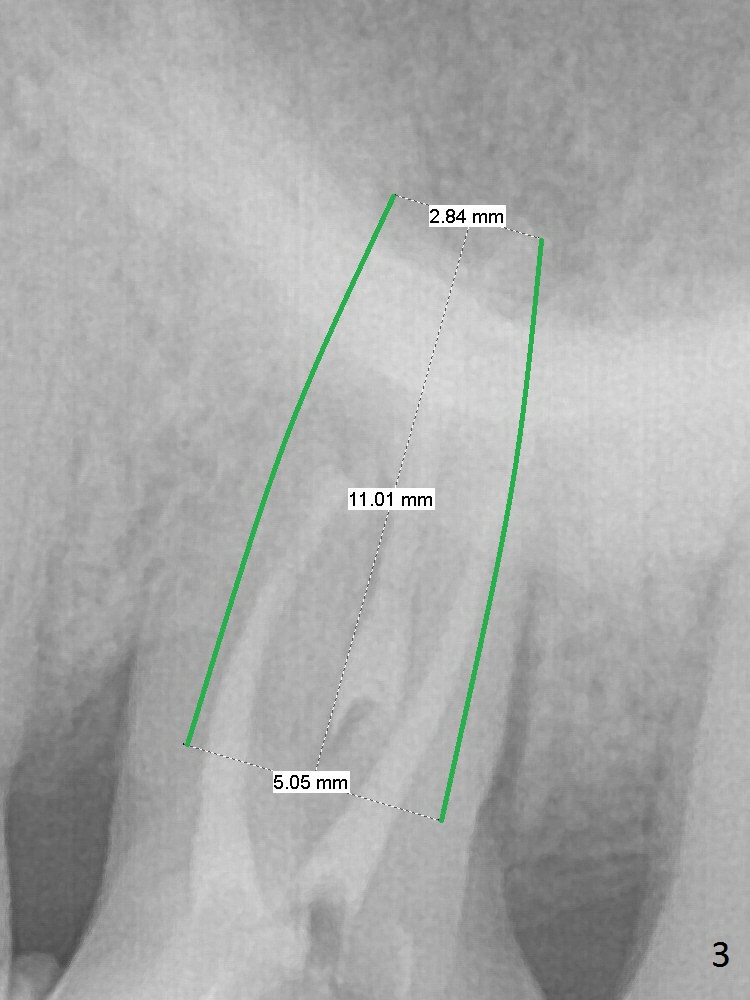
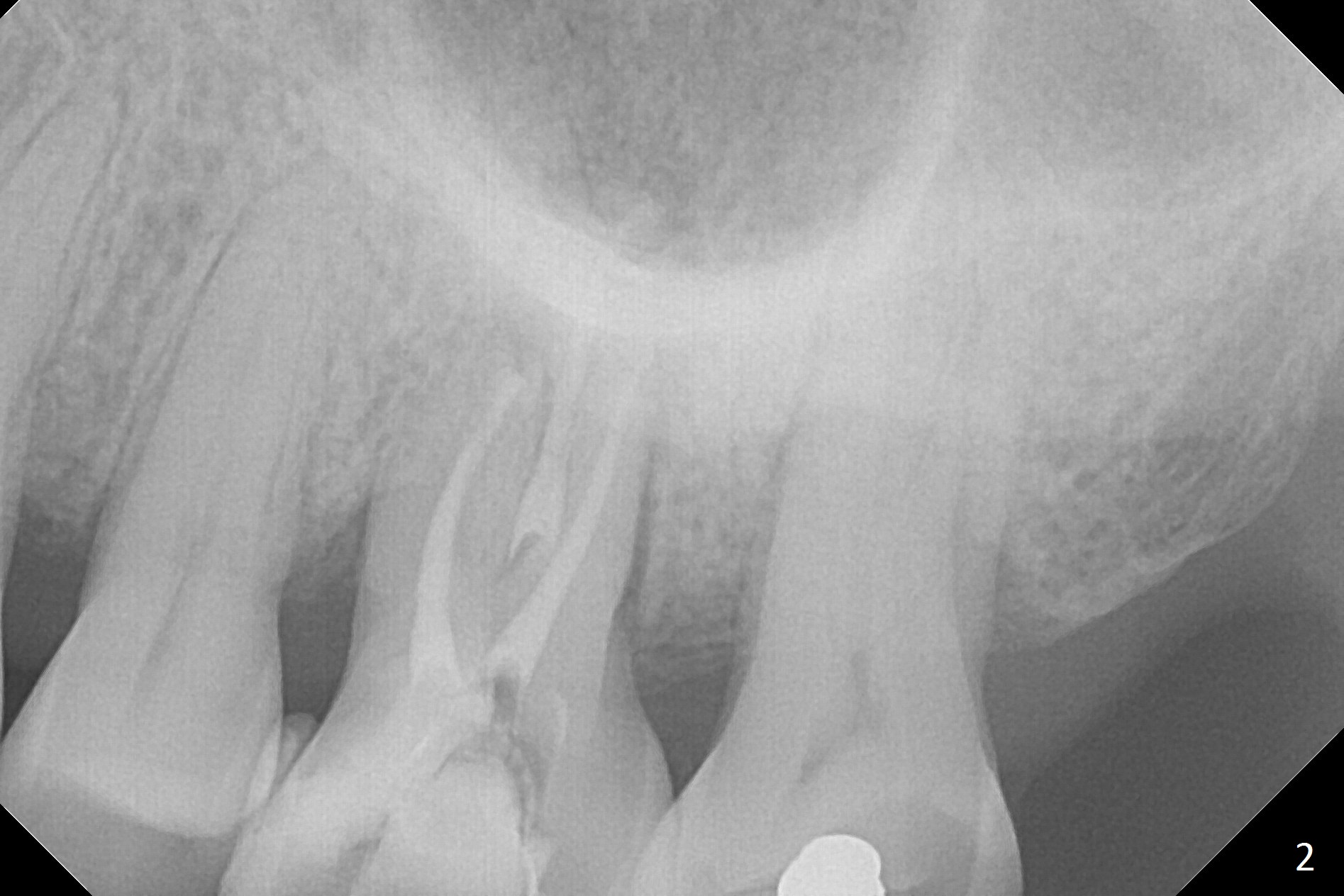
A 70-year-old woman has pain at MB root area post RCT at #14 (Fig.1,2). The tooth seems to have endo-perio disease (bone loss with gingival recession at MB) and be non-salvageable. After extraction and Metronidazole treatment, start osteotomy with 1.6 mm drill 1-2 mm shy of the sinus floor, followed by PA. Use Lindamann bur for ostetoomy position and trajectory adjustment. Use Marking Bur if necessary before Magic Drill 4.3 mm if the septum is wide. The depth of the osteotomy is 1-2 mm coronal to the sinus floor. Do not use the final drill, i.e., saving the osteotomy plug in place. Next 4.5x11 mm dummy implant is placed to push the plug upward for lifting. Place an implant as large as possible, but not violating the buccal gap (Fig.3).
The patient must be a bruxer, since the roots of the tooth #15 is long (Fig.1). The immediate provisional should have occlusal clearance.
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
IBS
Xin Wei, DDS, PhD, MS 1st edition 05/20/2017, last revision 11/25/2018