
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
||||
Why is One of Implants not Appropriate?
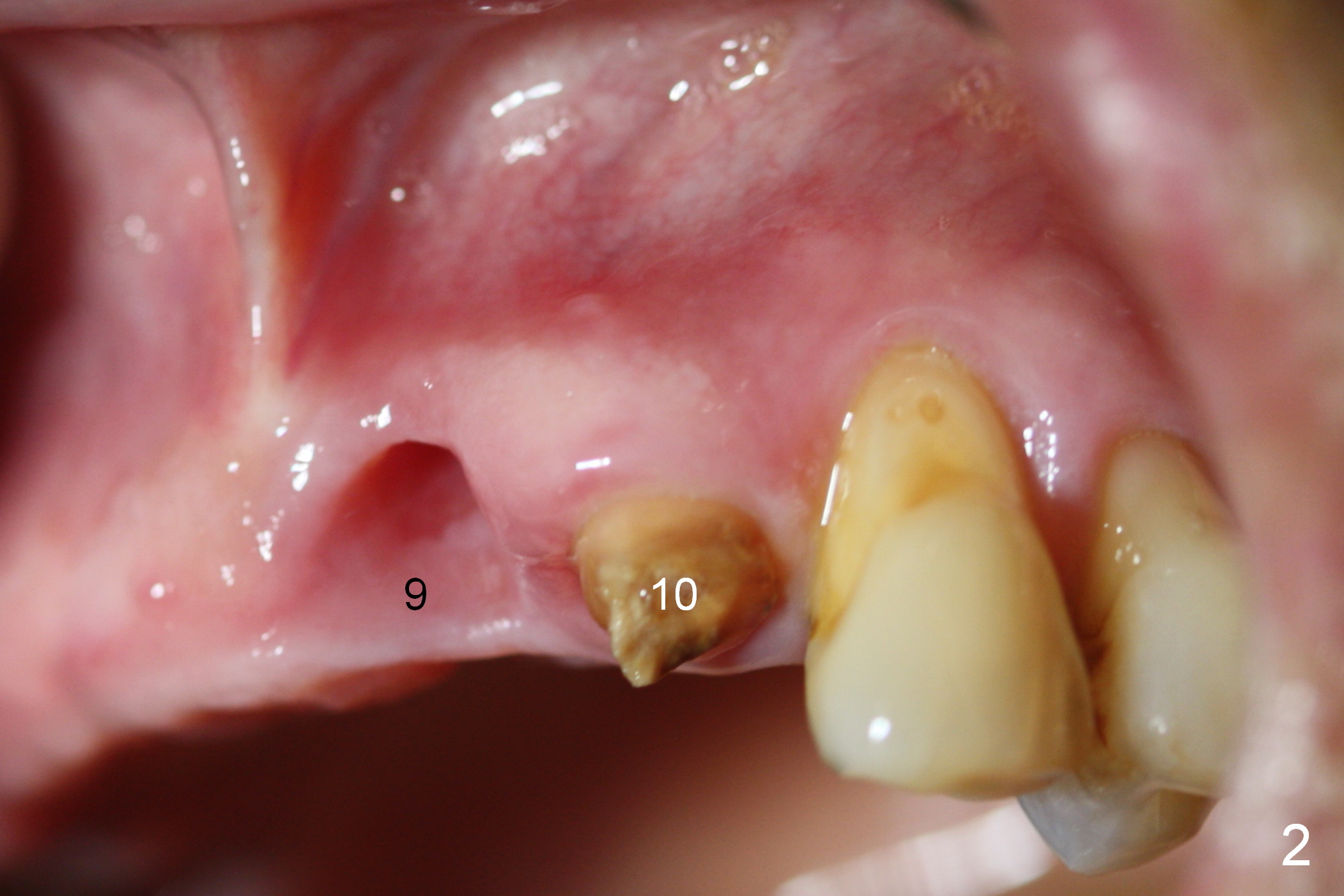
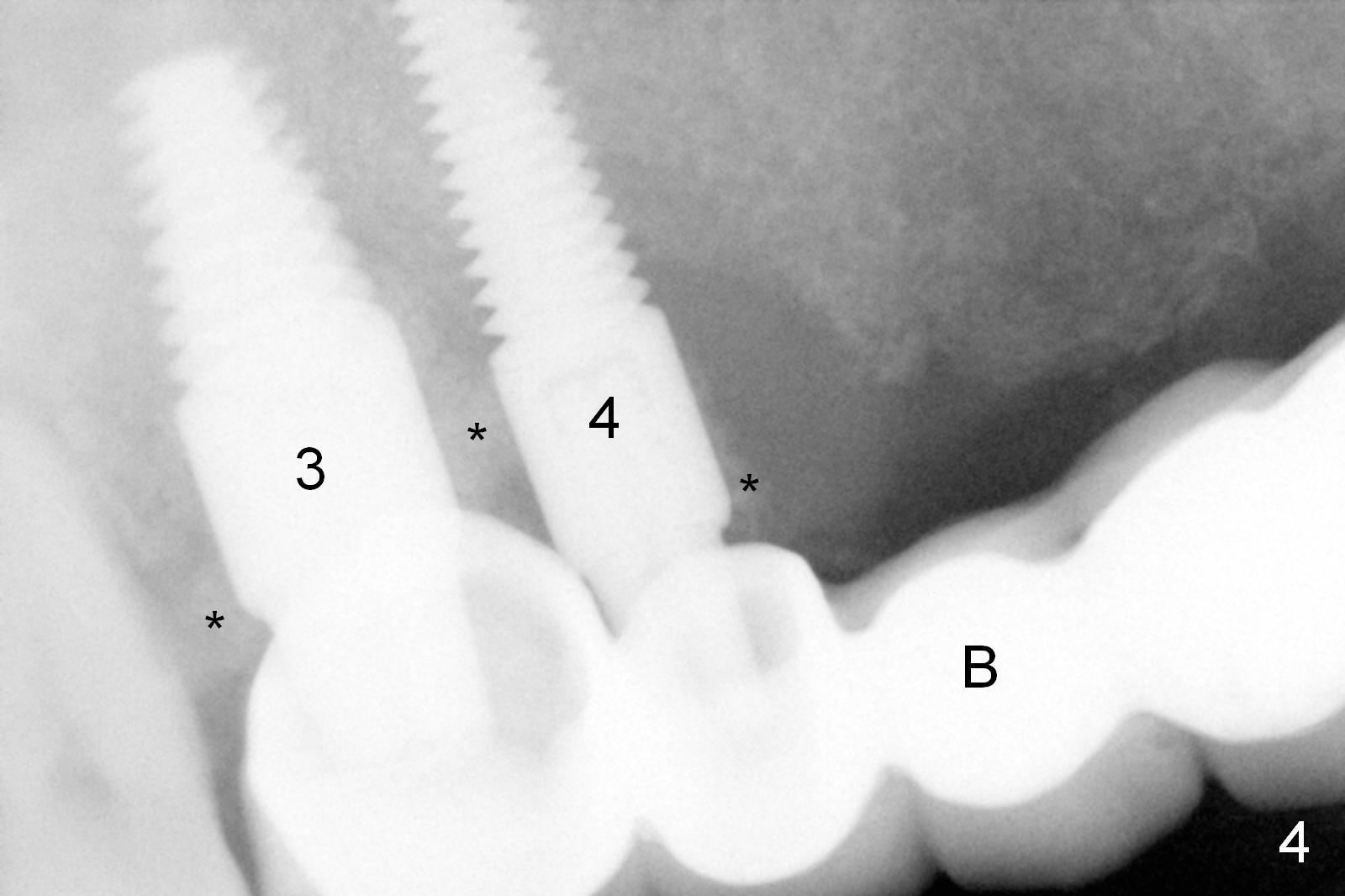
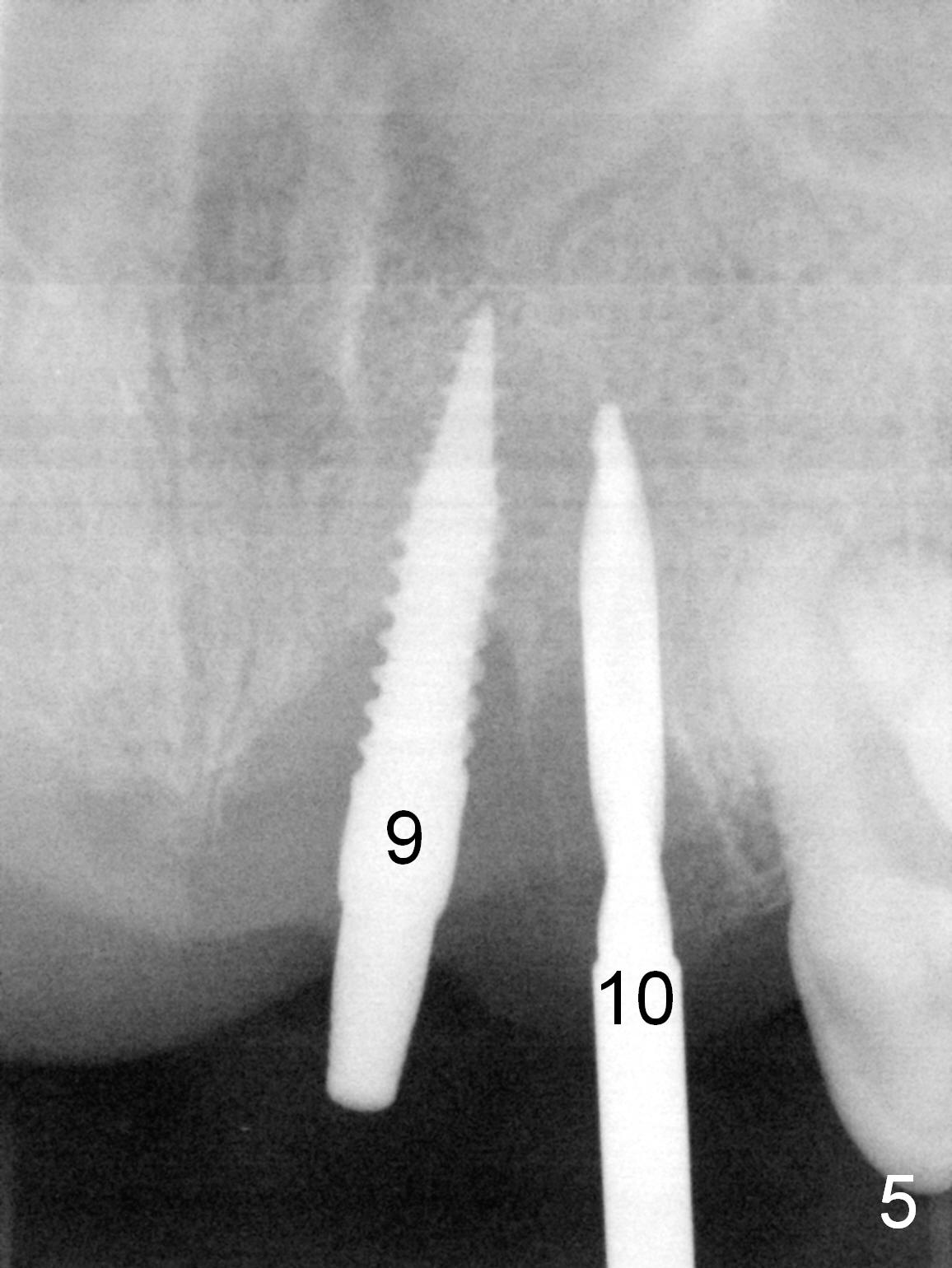
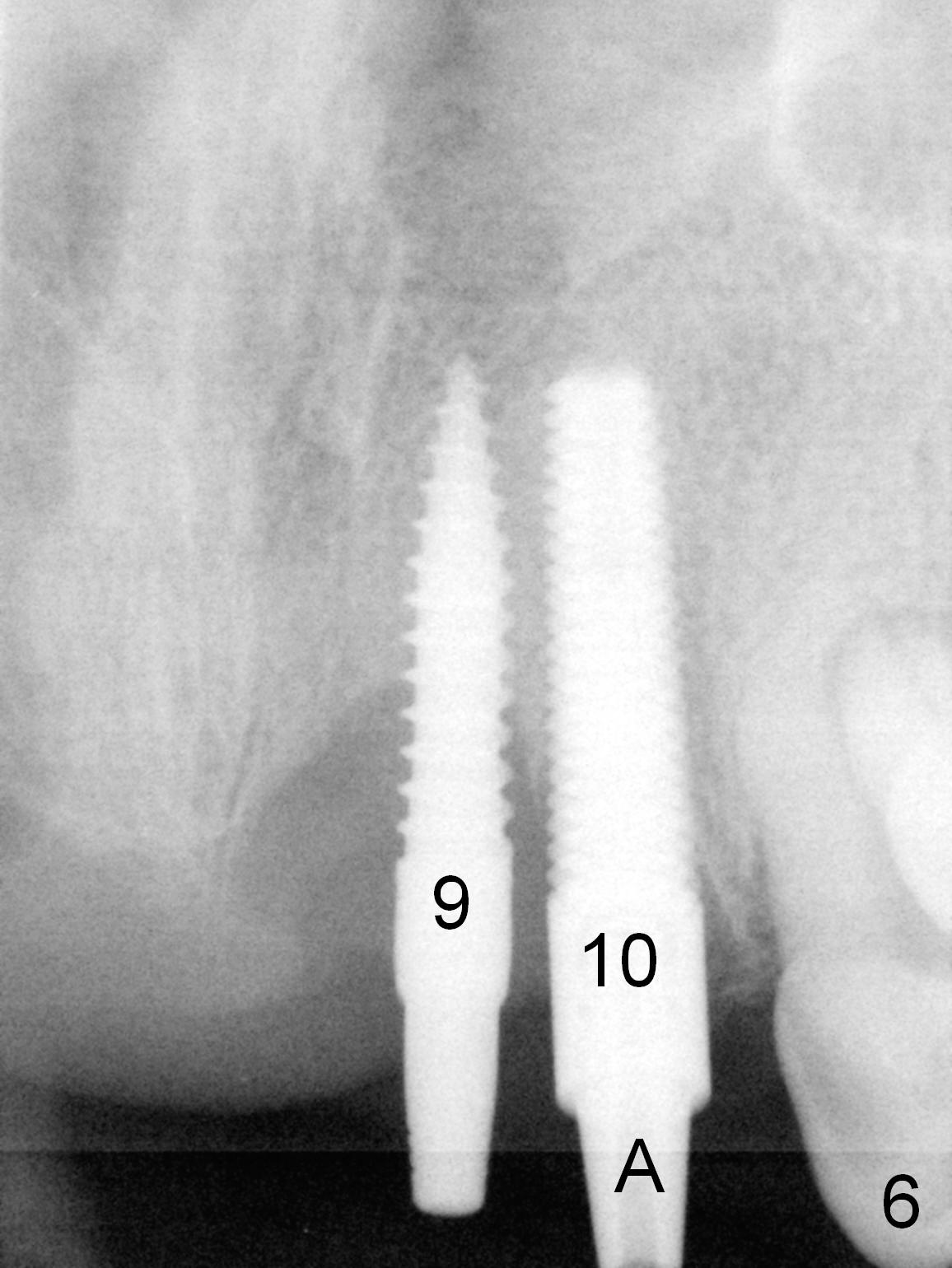
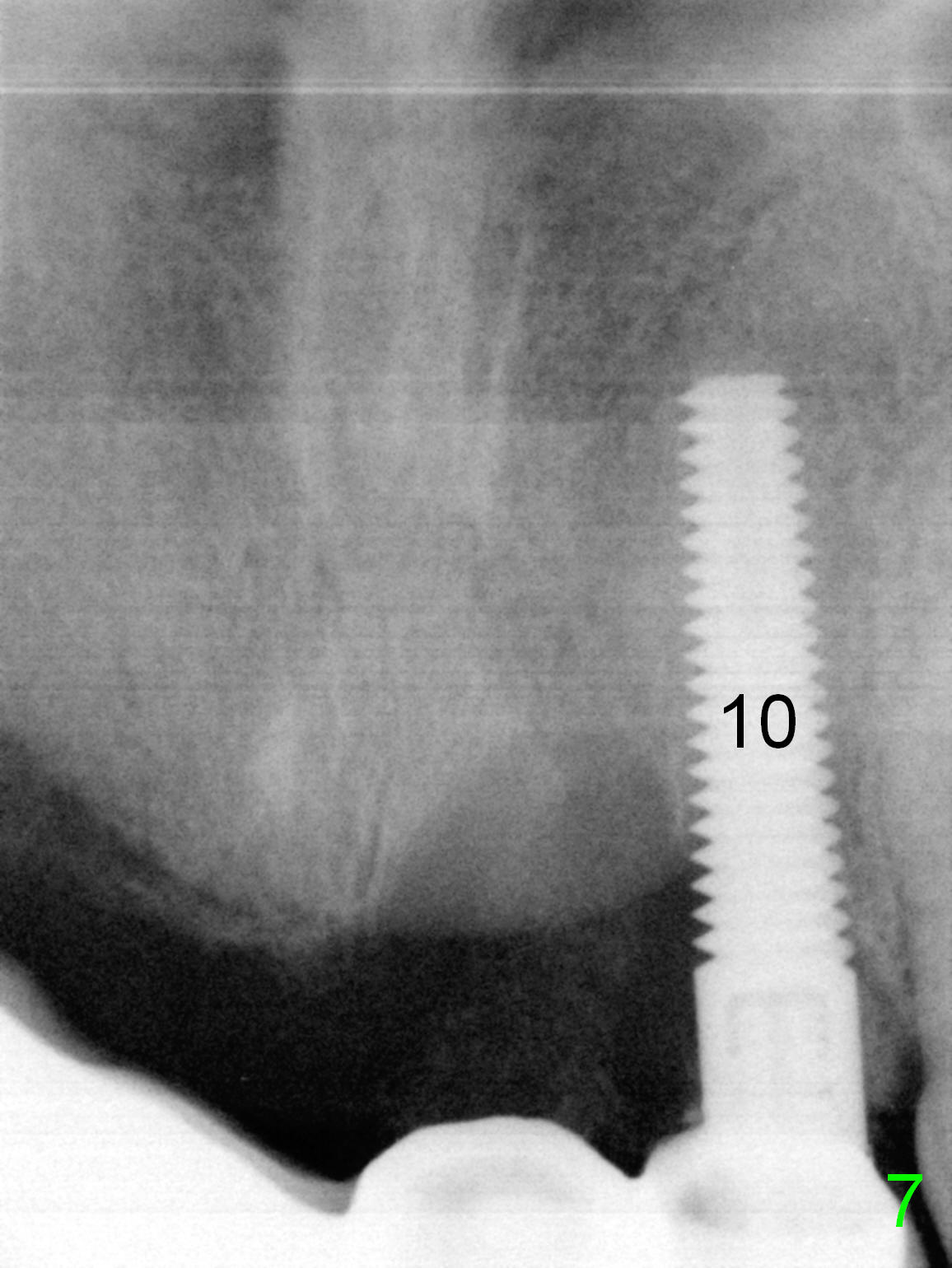
When the patient for implant placement, the existing bridge has been dislodged (Fig.1,2); the roots of the teeth #4 and 9 have also luxated from the sockets. The buccal plate at #9 appears to be atrophic. After Clindamycin treatment in the socket, a 3x14 mm 1-piece (dummy) implant is placed at #9, but found to be off in trajectory (Fig.5). After adjustment, it is found to be close to the neighboring implant (4x20 mm tissue-level, Fig.6). The 1-piece implant is later removed (with insertion of Osteoplug); the implant at #10 is used as an anterior abutment to retain the existing bridge (Fig.4 B) after reline (Fig.7).
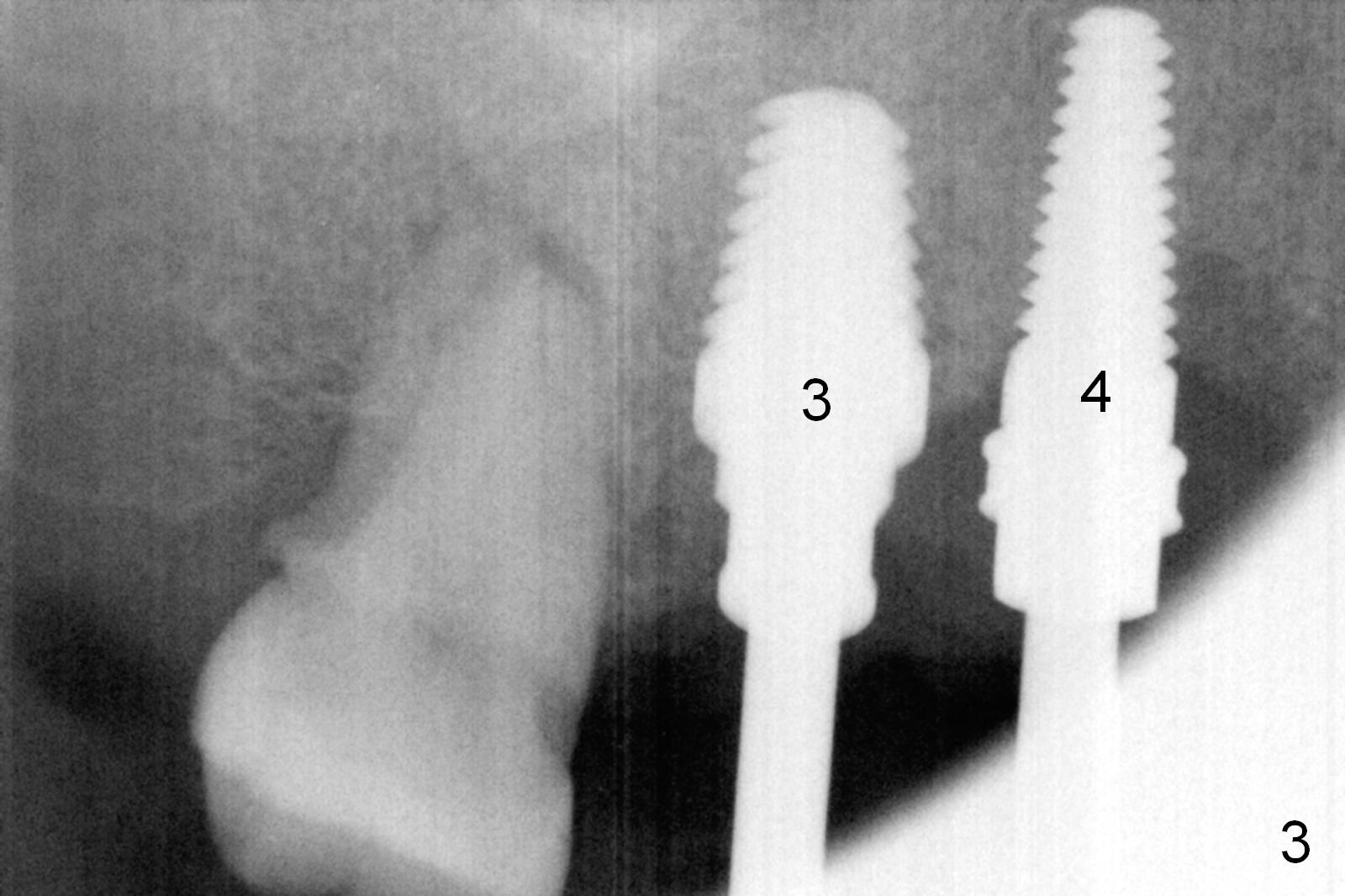
Since there is gingival hyperplasia between the residual roots at #3 (Fig.1), implant placement at #3 and 4 needs incision and raising of the flaps. There is minimal bone loss posteriorly; taps (Fig.3) and implants (Fig.4 (*: bone graft)) are larger than the anterior one (Fig.7).
At the 2nd stage, implants will be placed at #6 and 7. Bridges will be fabricated between #4 and 6 and between #7 and 10. The crown at #3 will be single unit.
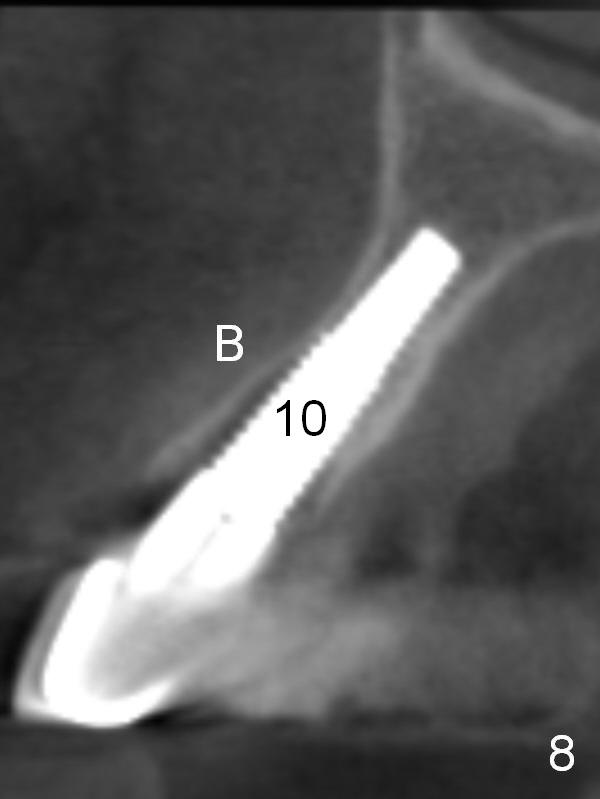
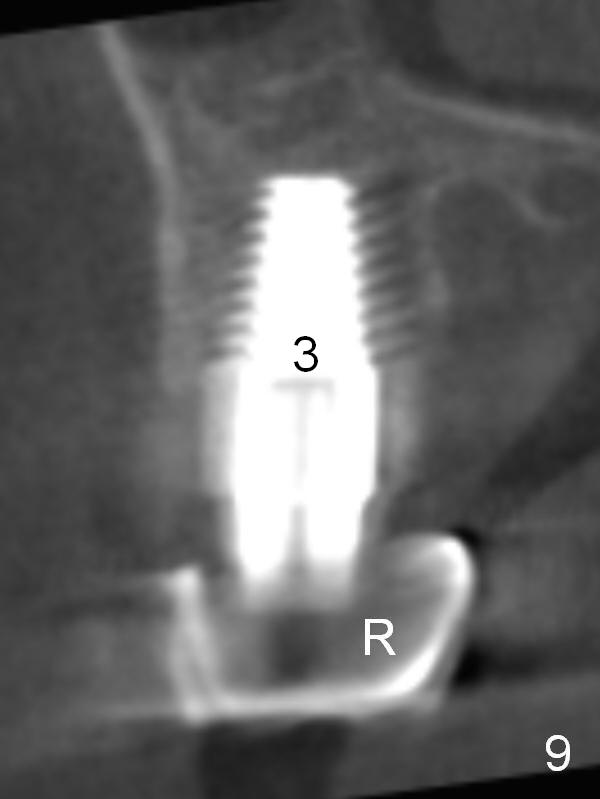
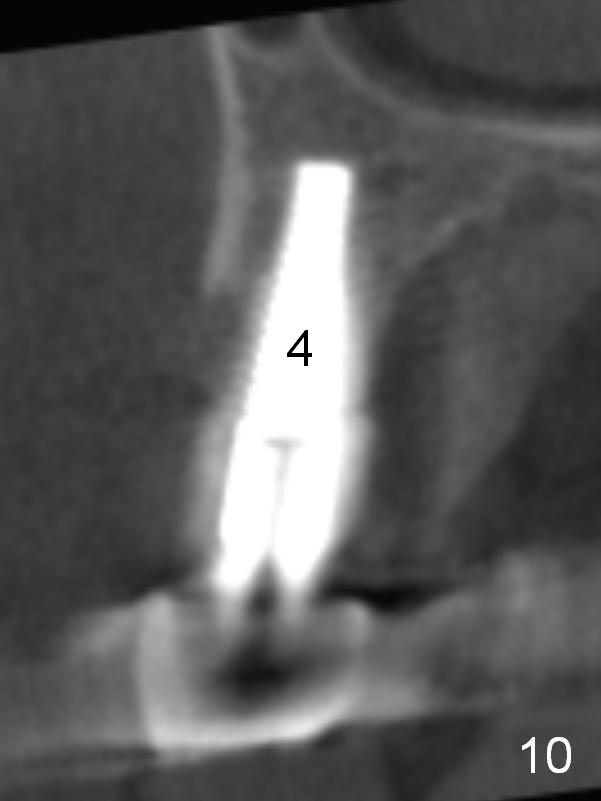
CT scan taken 10 days postop shows that the three implants are placed in the middle of the alveolus (Fig.8-10 (coronal sections); B: buccal; R: retainer of the bridge). CT scan changes the treatment plan of the 2nd stage of implant placement.
Return to Upper Arch Immediate Implant,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 10/27/2015, last revision 08/05/2018