|
|
|
Tripod Septum
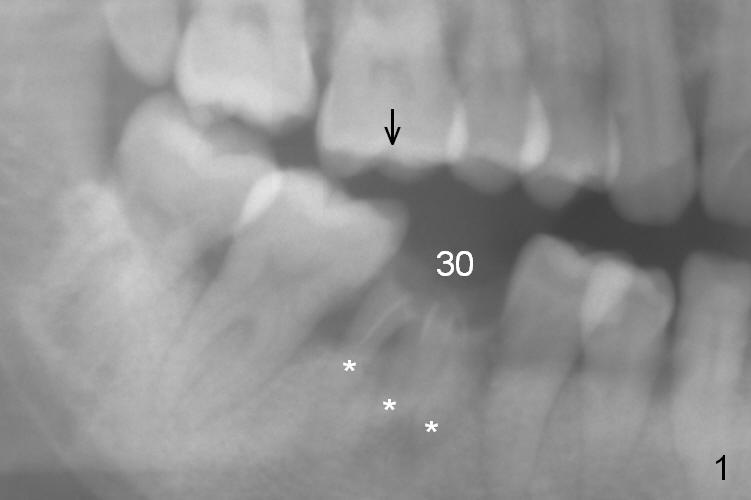
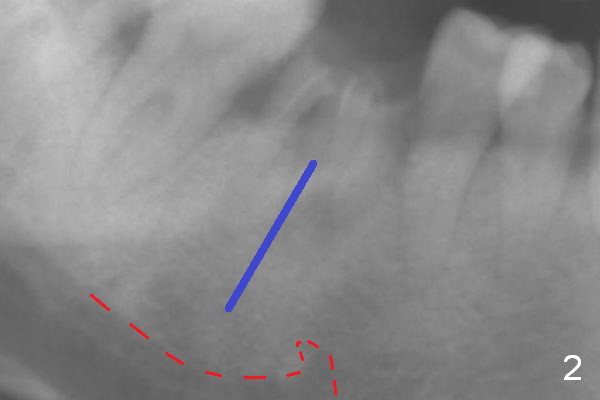
A 37-year-old woman is afraid of dentistry and procrastinates implant restoration at #30 (Fig.1). The opposing tooth is supraerupted (arrow) and warrants occlusal adjustment for #30 immediate provisional. Since there are 3 roots associated with #30 (*), the septum should be tripod, where osteotomy will be established after Clindamycin socket application. Primary stability of the immediate implant is further enhanced by the bone height. It is expected to gain ~ 6 mm in the native bone (Fig.2 blue line). As long as the osteotomy is slightly longer than the 2nd molar, there is minimal chance to involve the superior border of the Inferior Alveolar Canal (red dashed line). Magic Split and Expanders are to be used in combination with drills if necessary. Photograph the septum before and after osteotomy.
The 2nd method of osteotomy is to use 3.8 or 4.3 mm drill (after marking drill) in the middle of the septum at the depth determined by preop PA after removal of the coronal portion of the residual roots with high speed handpiece. Keep the drill in place for intraop PA. Remove the roots. A 4.5x13 mm implant will be placed. Either way, prepare PRF.
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), IBS Xin Wei, DDS, PhD, MS 1st edition 07/31/2016, last revision 06/03/2018