



|
|
|
|
|
|
|
|
|
|
||
|
|
|
|||
Septum Placement
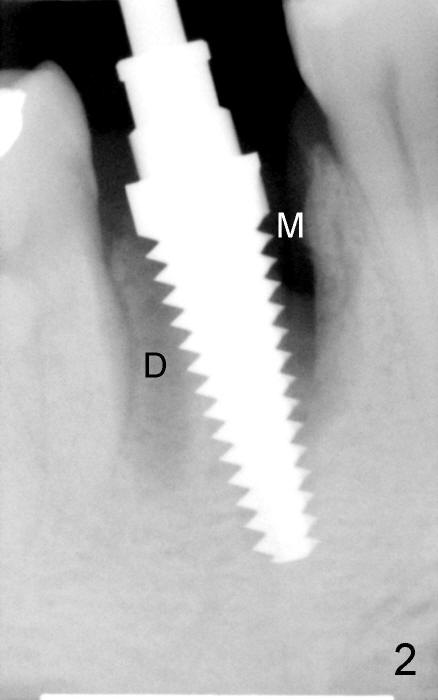
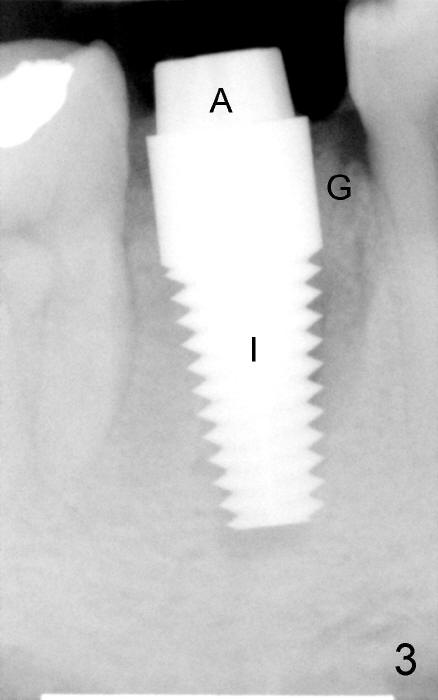
The patient returns for extraction and immediate implant after 7 days of oral Amoxicillin. There is a deep pocket mesiolingually in addition to the mesiobuccal fistula (Fig.1 <). The metal crown and then the tooth are sectioned. The crack of the mesial root is confirmed during extraction. The coronal portion of the mesiobuccal plate is defective, corresponding to the fistula. Both the mesial and distal sockets are large with a thin septum in between. Osteotomy is established at the base of the septum, slightly toward the mesial socket, as evidenced by a 5x20 mm tap in place (Fig.2). Finally, a 7x17 mm implant is placed (Fig.3 I; A: abutment; G: bone graft). The insertion torque is more than 60 Ncm.
In this case, the root fracture is associated with dense bone (type II). Primary stability is easily achieved. In addition, apical to the original sockets, the implant has five of bony walls, whereas the rest portion two (buccal and lingual). Therefore, do not miss the opportunity of immediate implant.
Due to the presence of the abutment (Fig.4 arrowheads), the perio dressing remains in place 7 days postop.
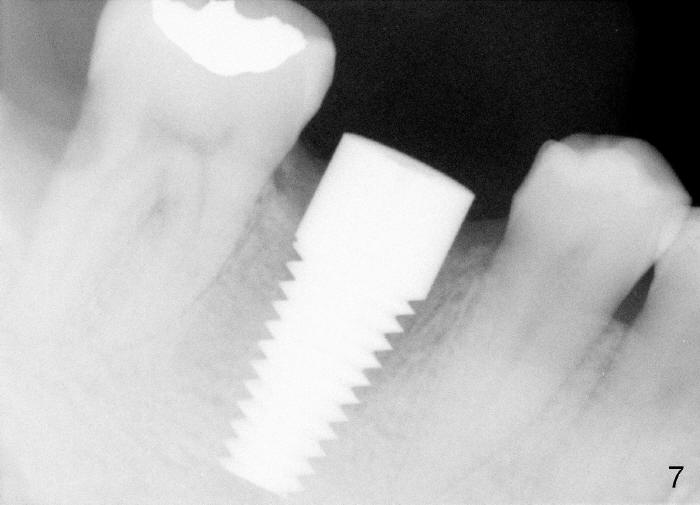
Three weeks postop, the gingiva is healthy around the implant (Fig.5 I). There is no symptom or sign of the infection (>, as compared to Fig.1). The abutment has accomplished its transient function (A, the perio dressing having dislodged) and is subsequently removed (Fig.6, to reduce micromovement of the implant and cheek and tongue bite). The 7 mm implant (I) does not look too big in its new home (alveolus). Four months postop, the mesial socket appears to have normal bony trabecular patterns (Fig.7, as compared to Fig.3).
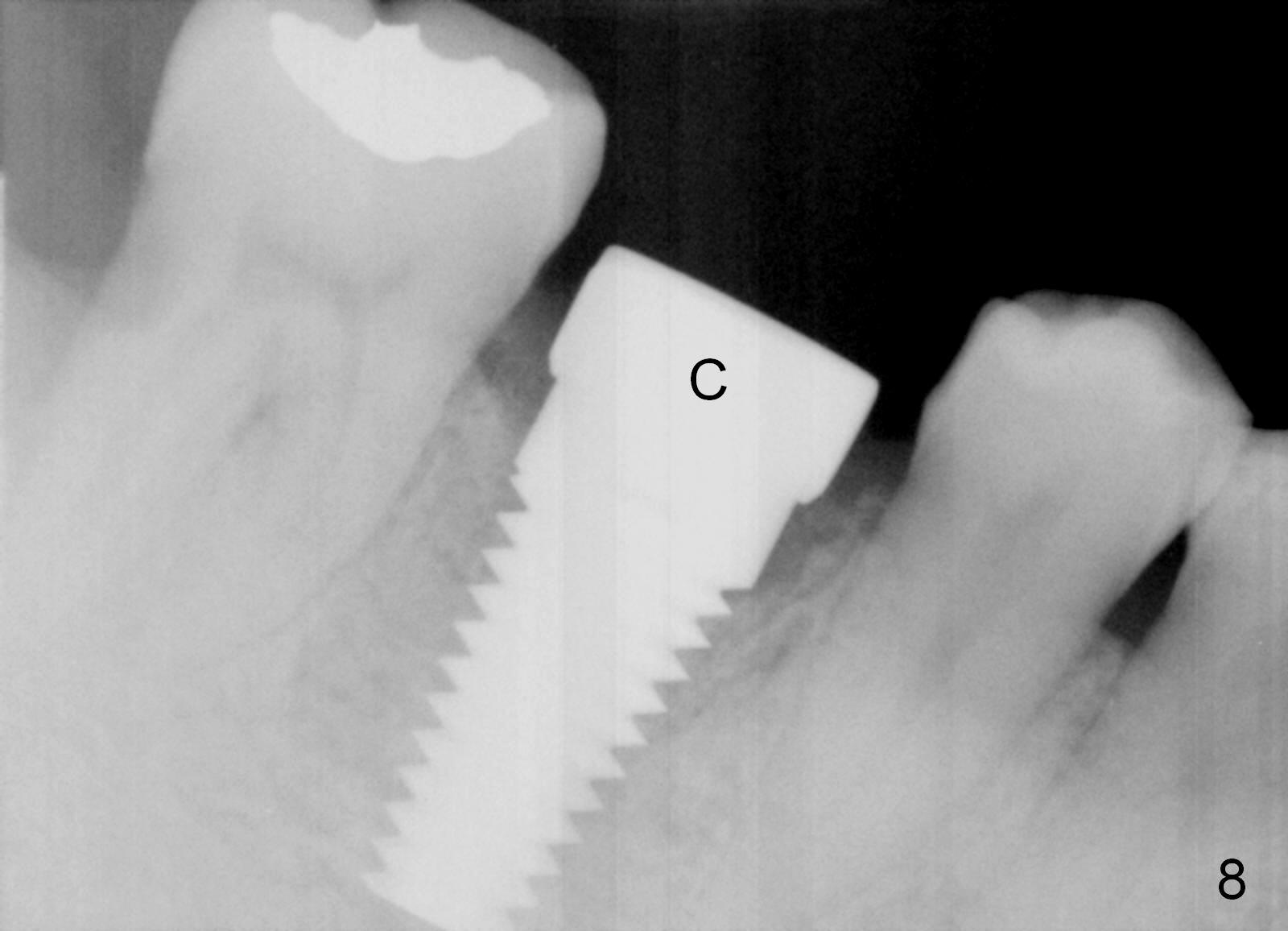
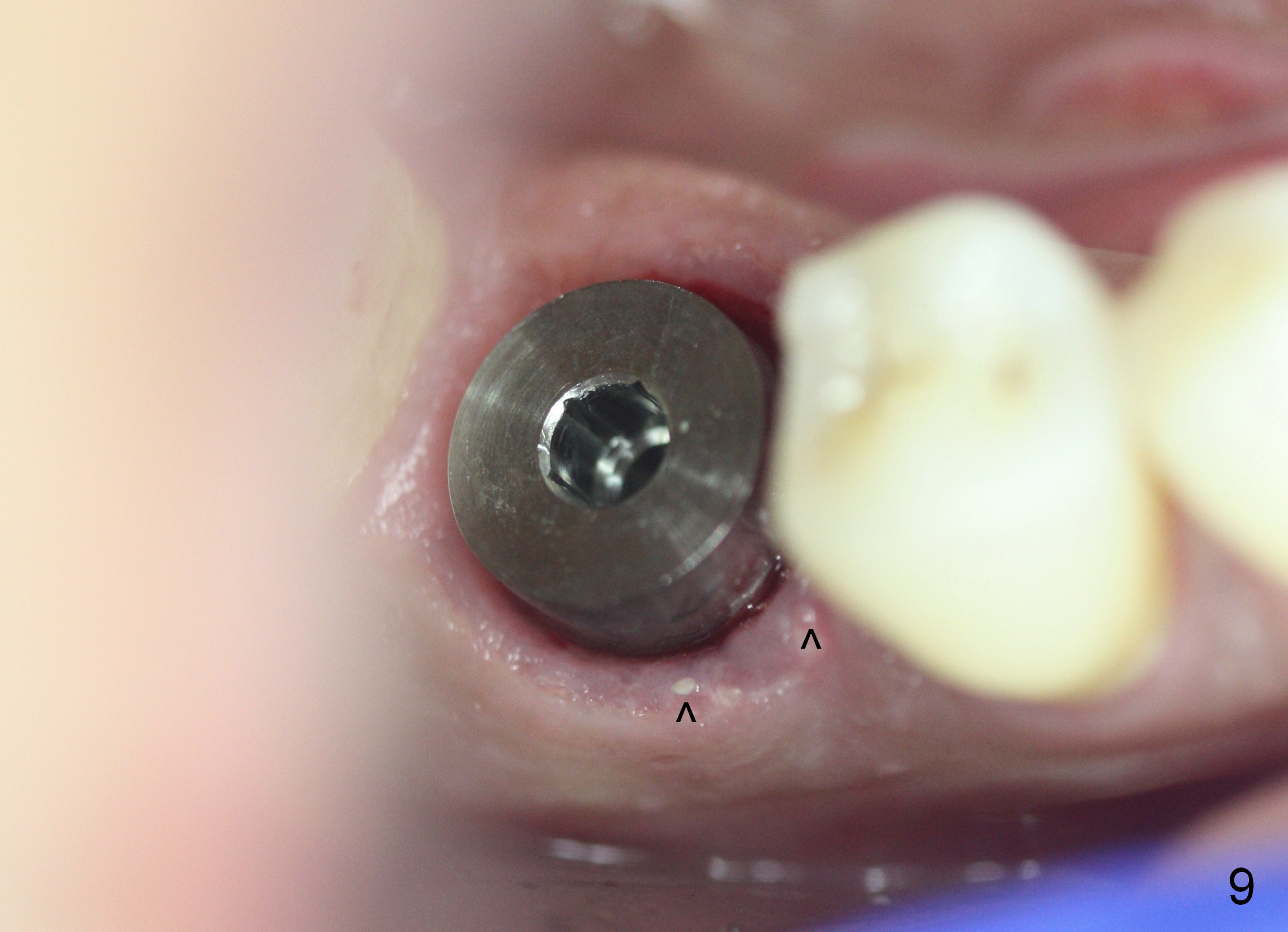
The next time the patient returns is 8.5 months postop (Fig.8,9). When an immediate provisional is not provided, the patient tends not to return early. In fact, retention of an immediate provisional and confidence in it by the patient promotes early finish of treatment (permanent crown).
Return to Lower Molar Immediate Implant,
Immediate Posterior Provisional
Xin Wei, DDS, PhD, MS 1st edition 07/19/2014, last revision 01/01/2017