





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
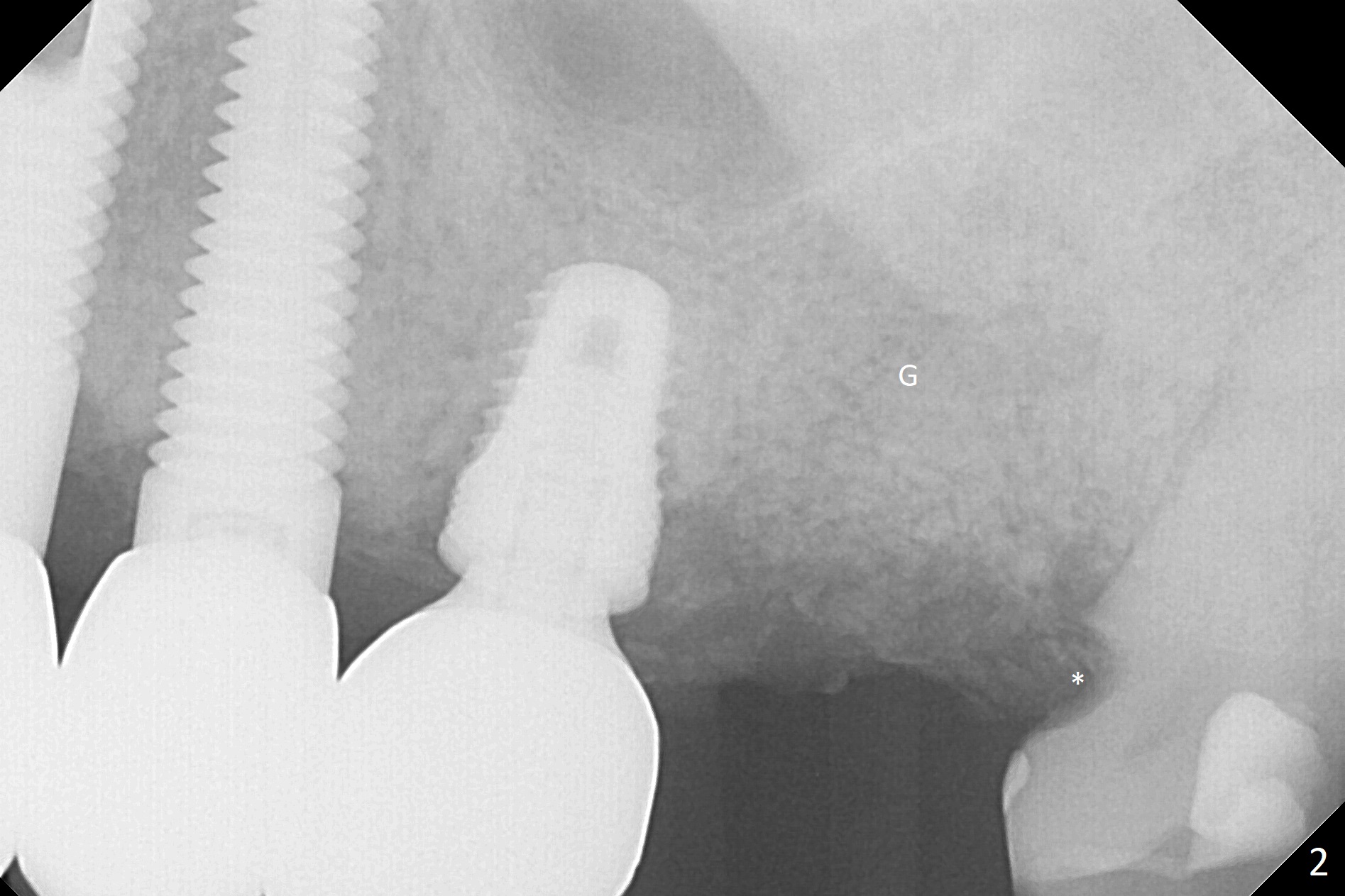
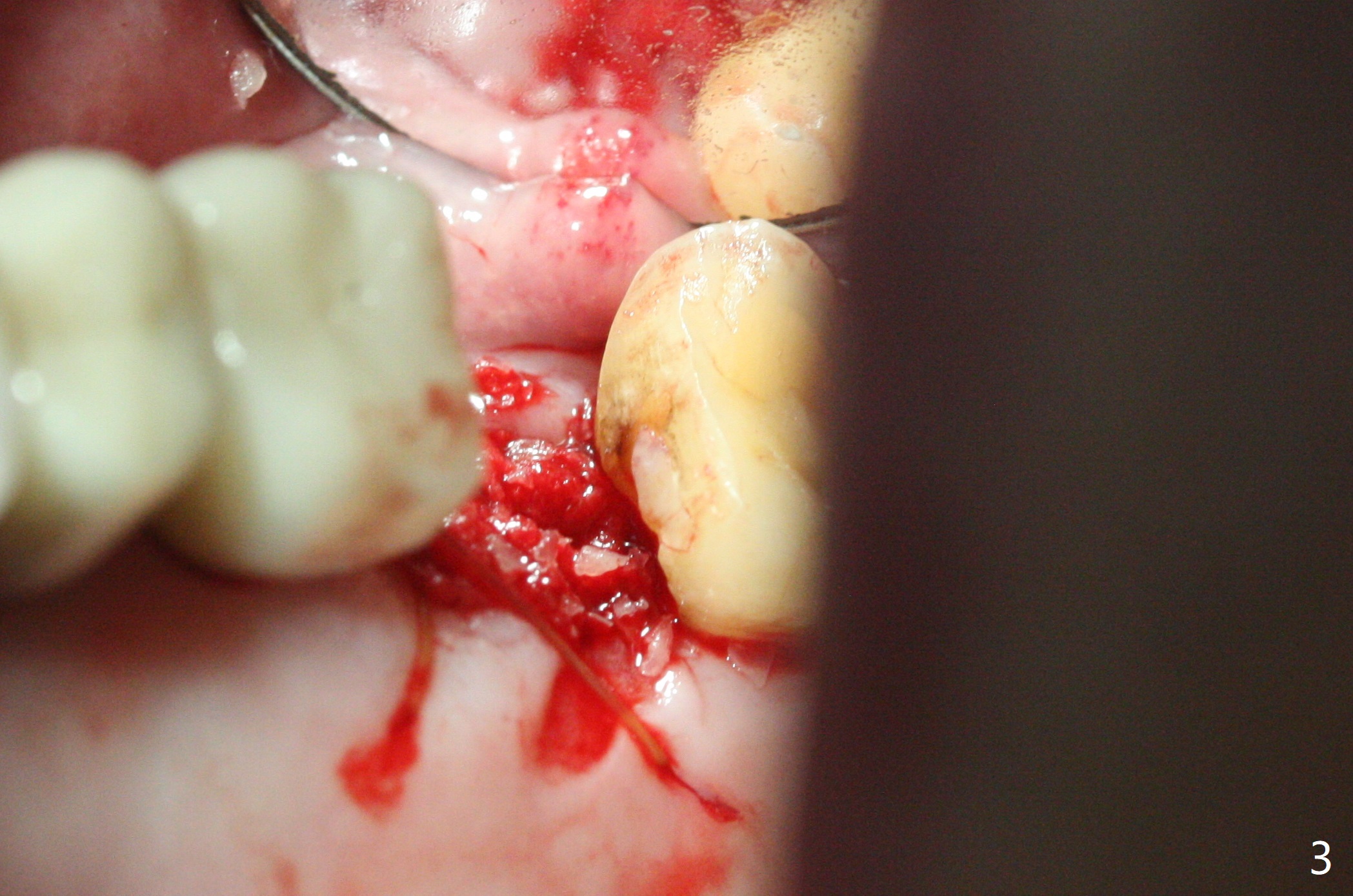
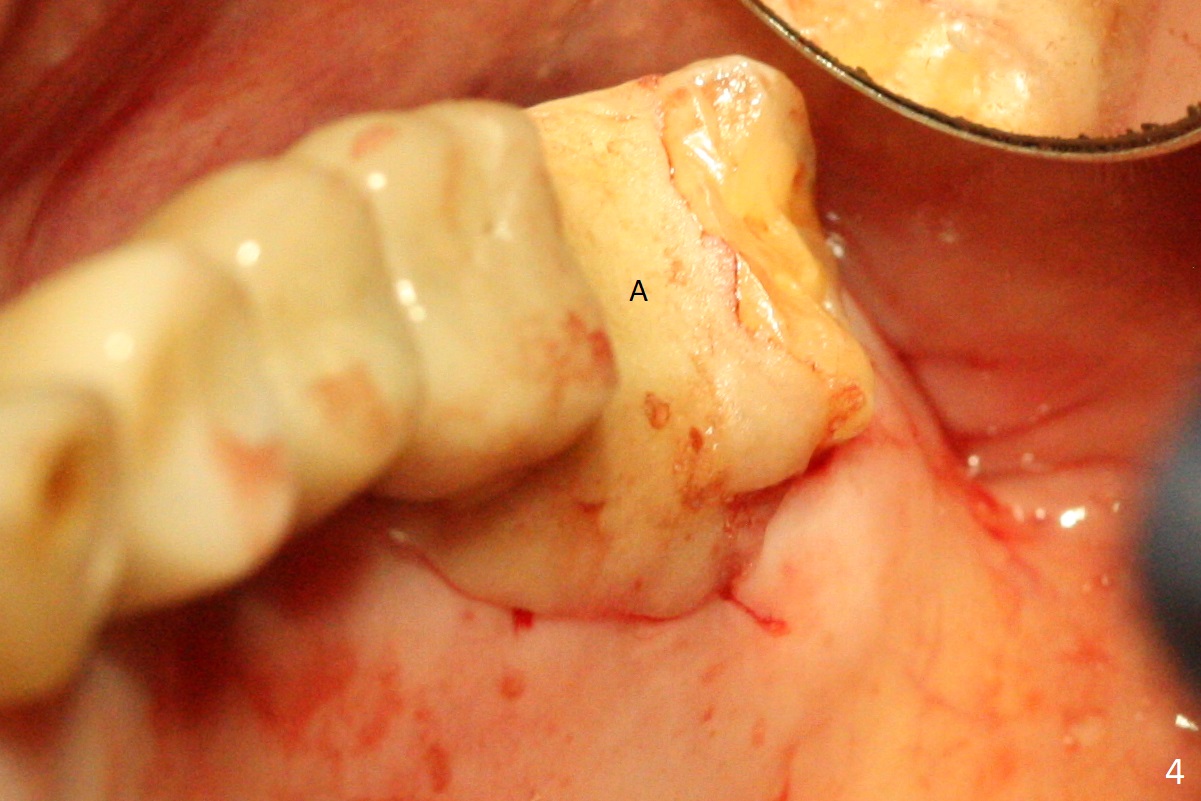
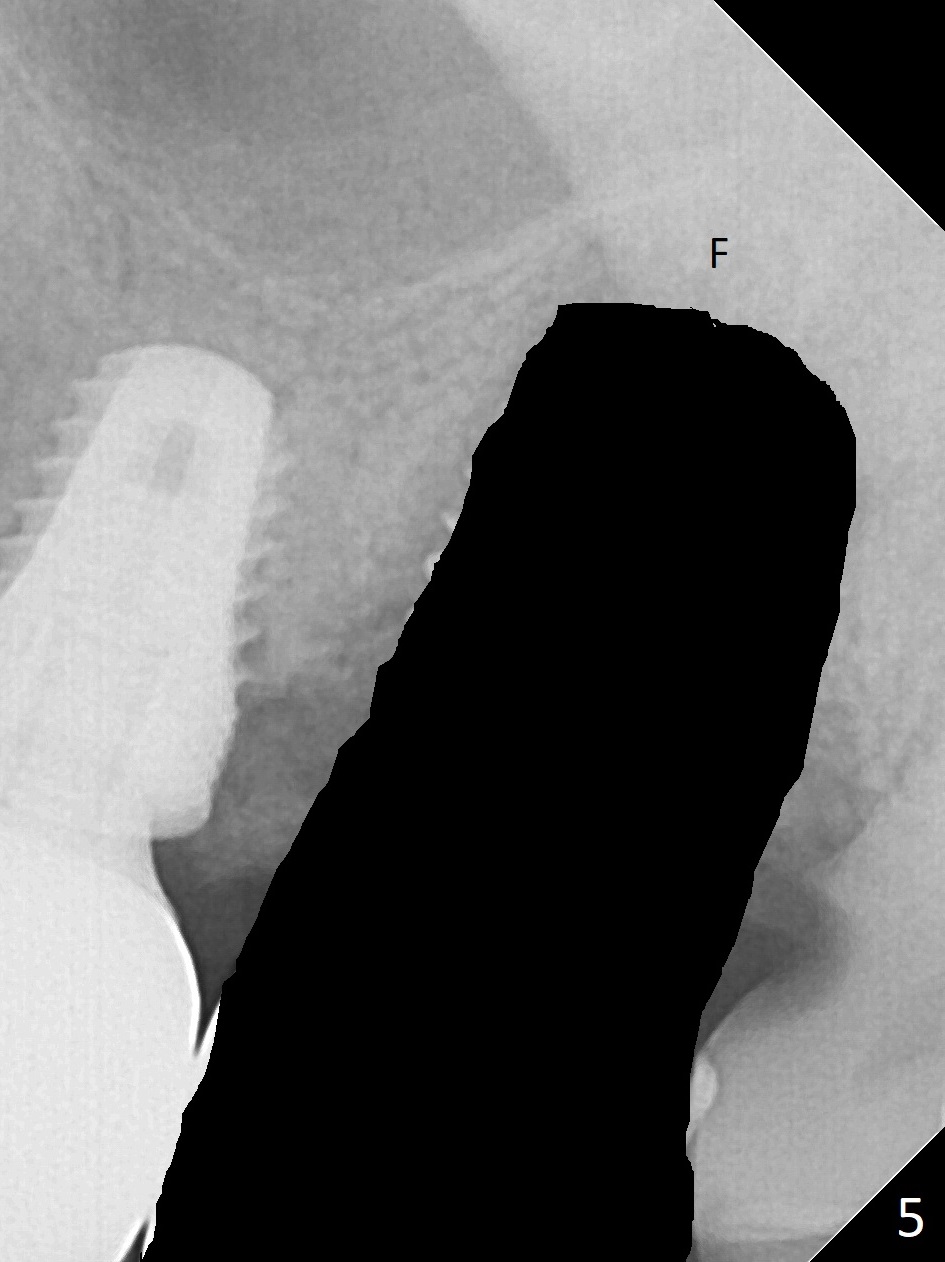
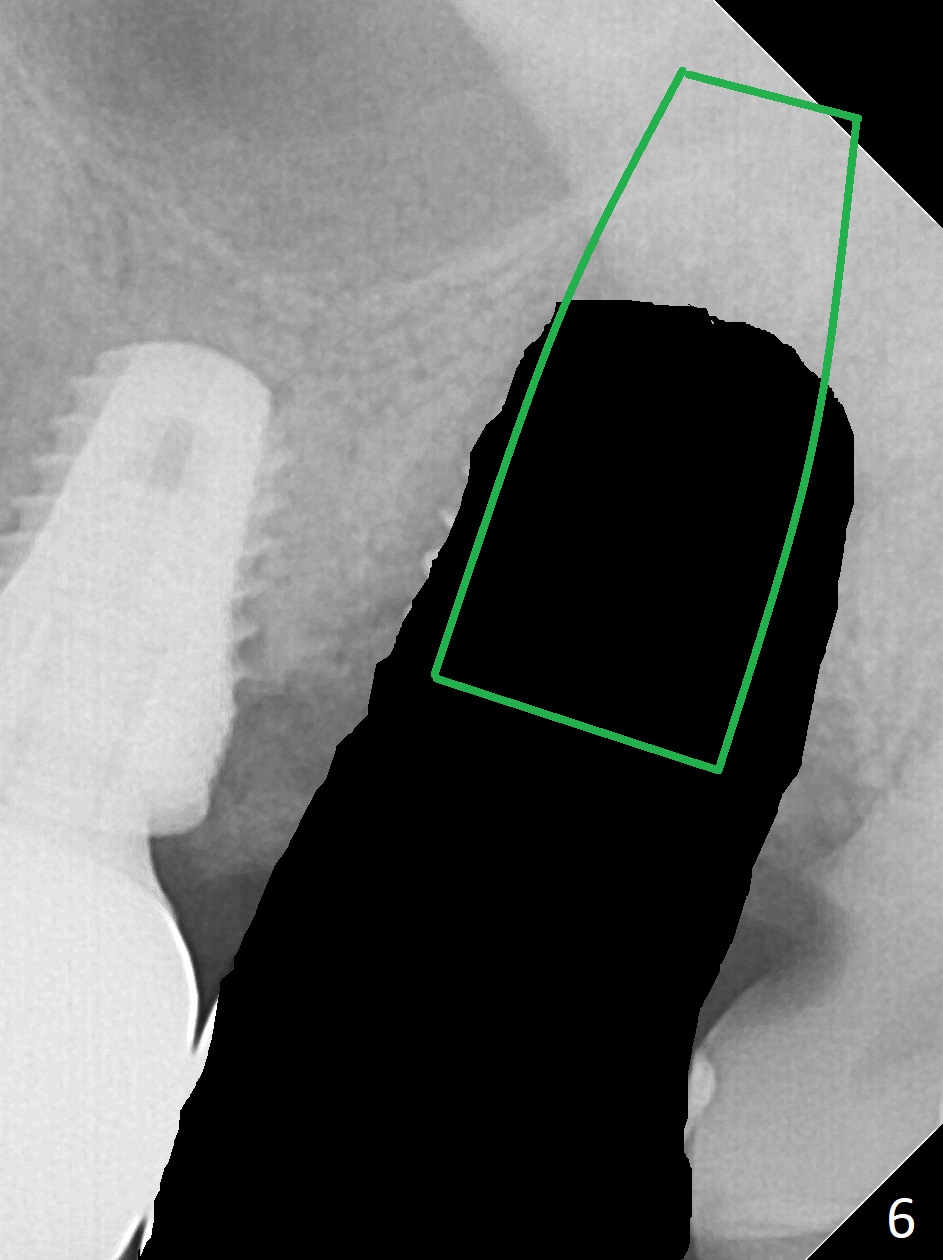
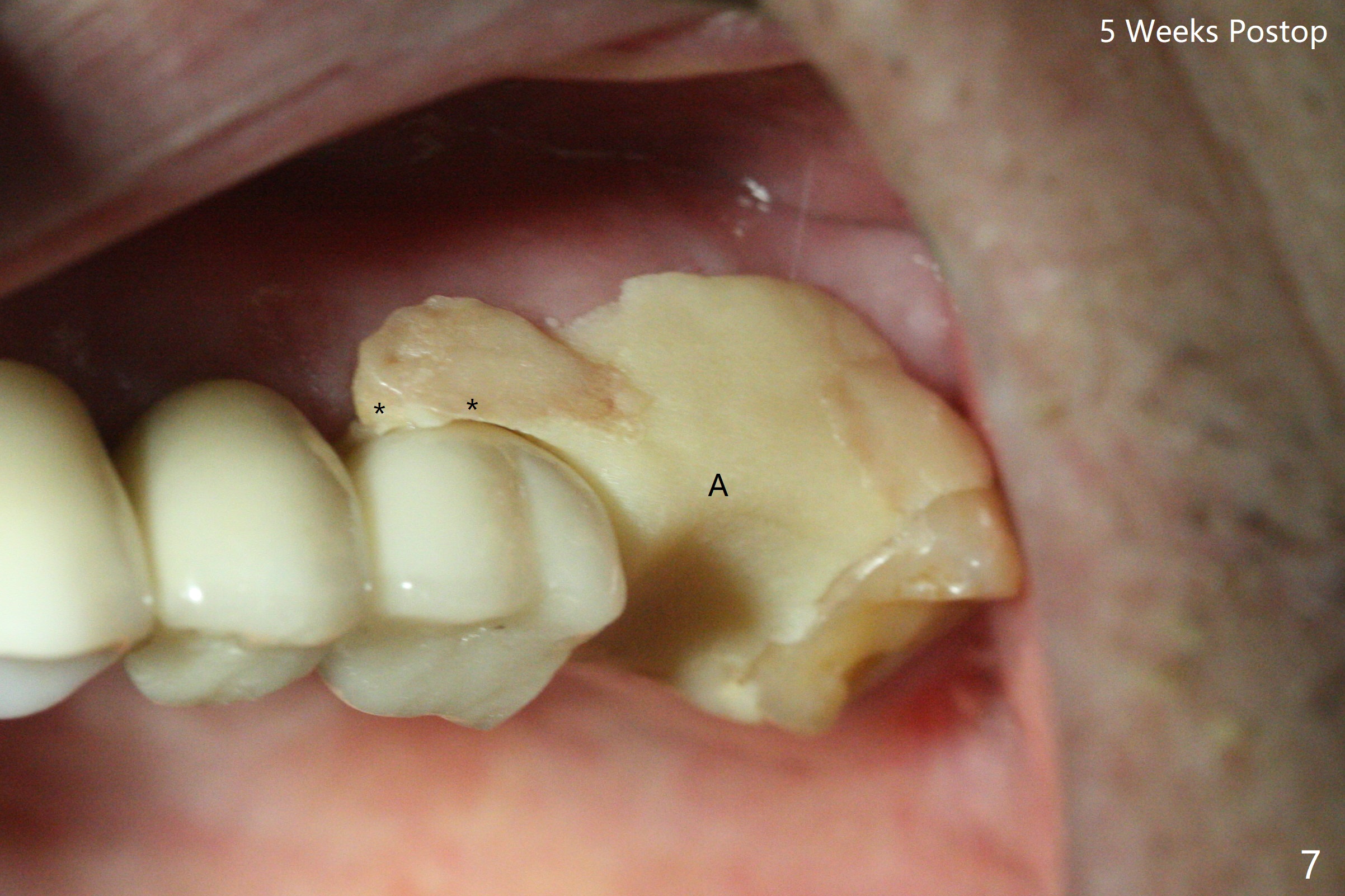
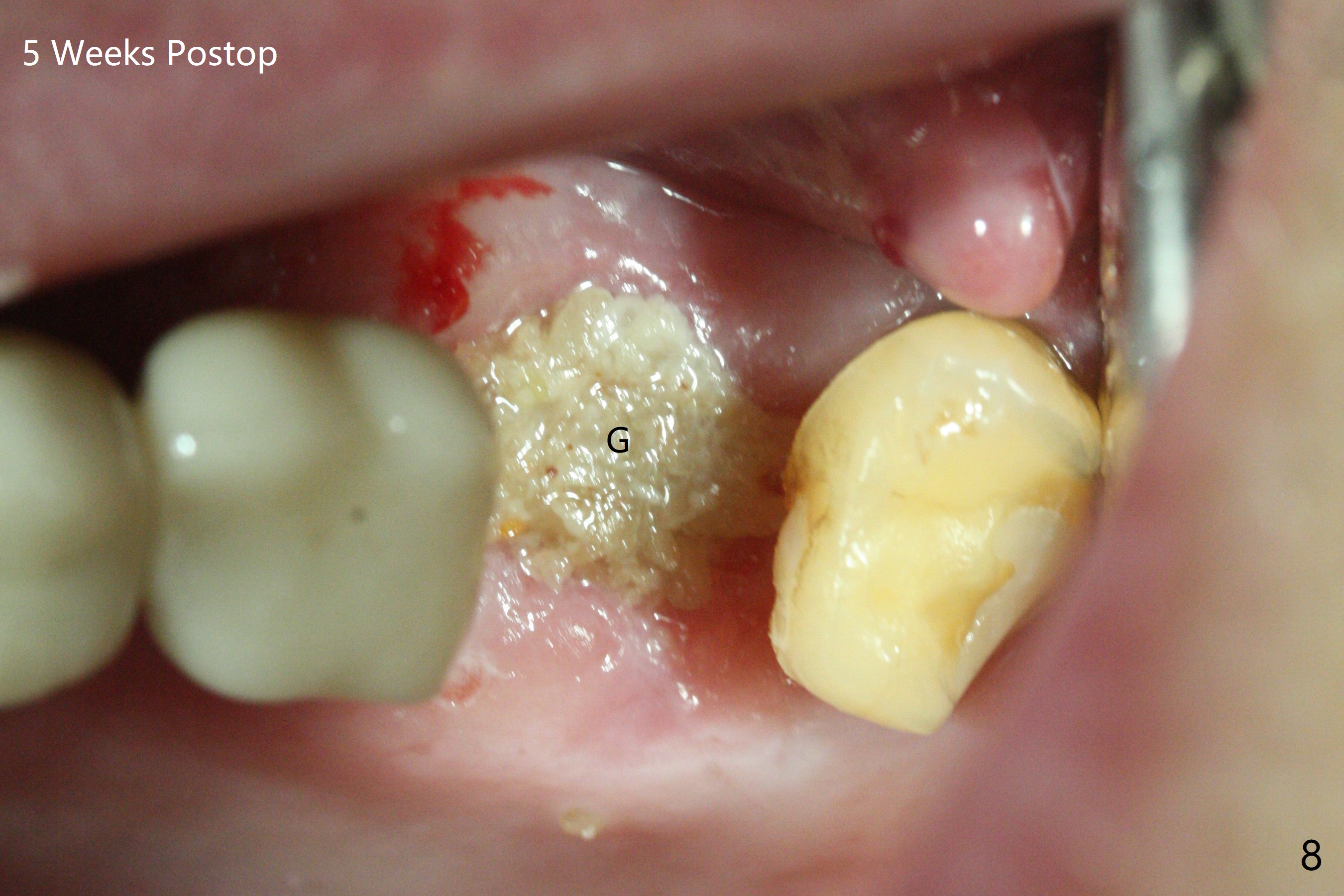
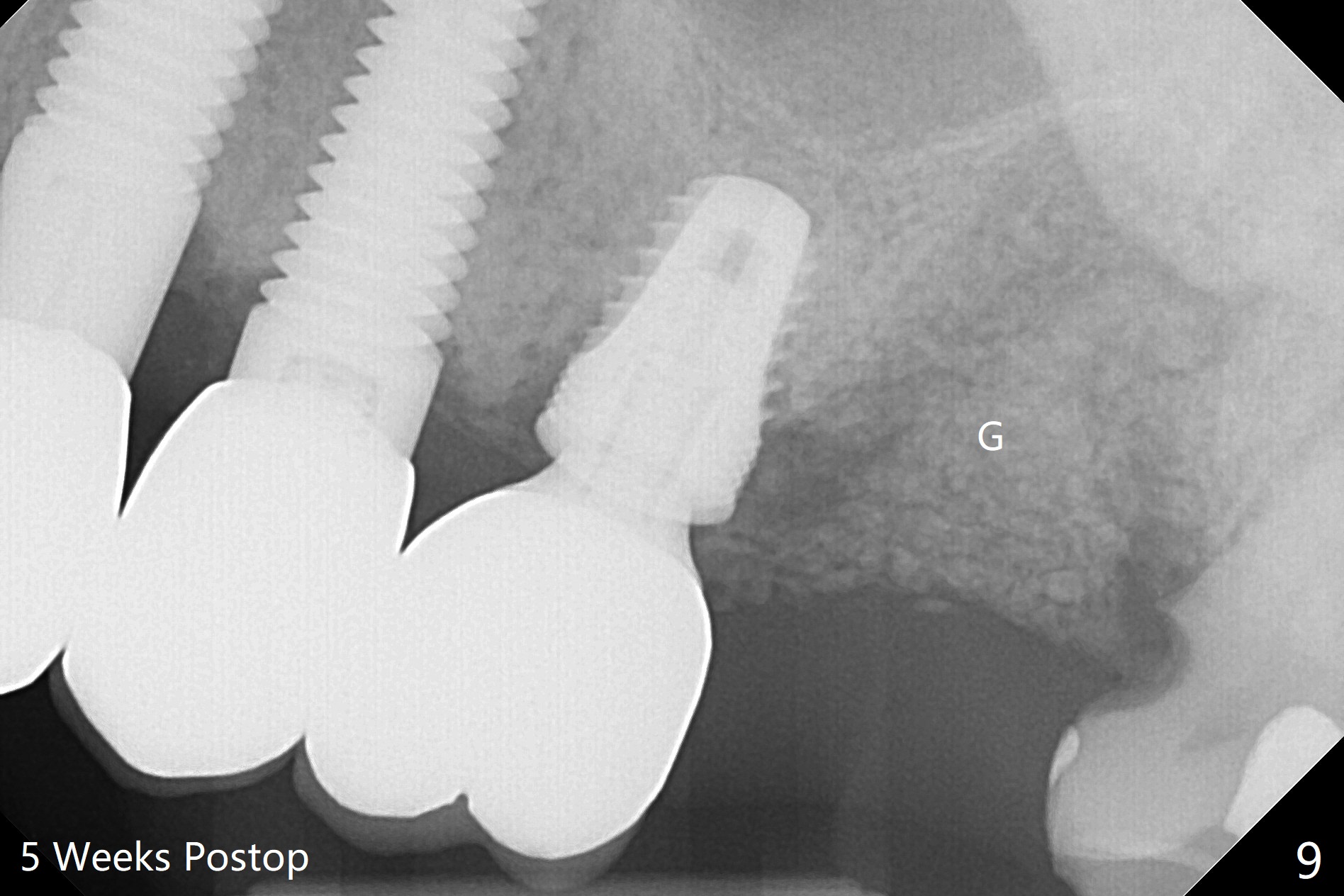
Acrylic Dressing
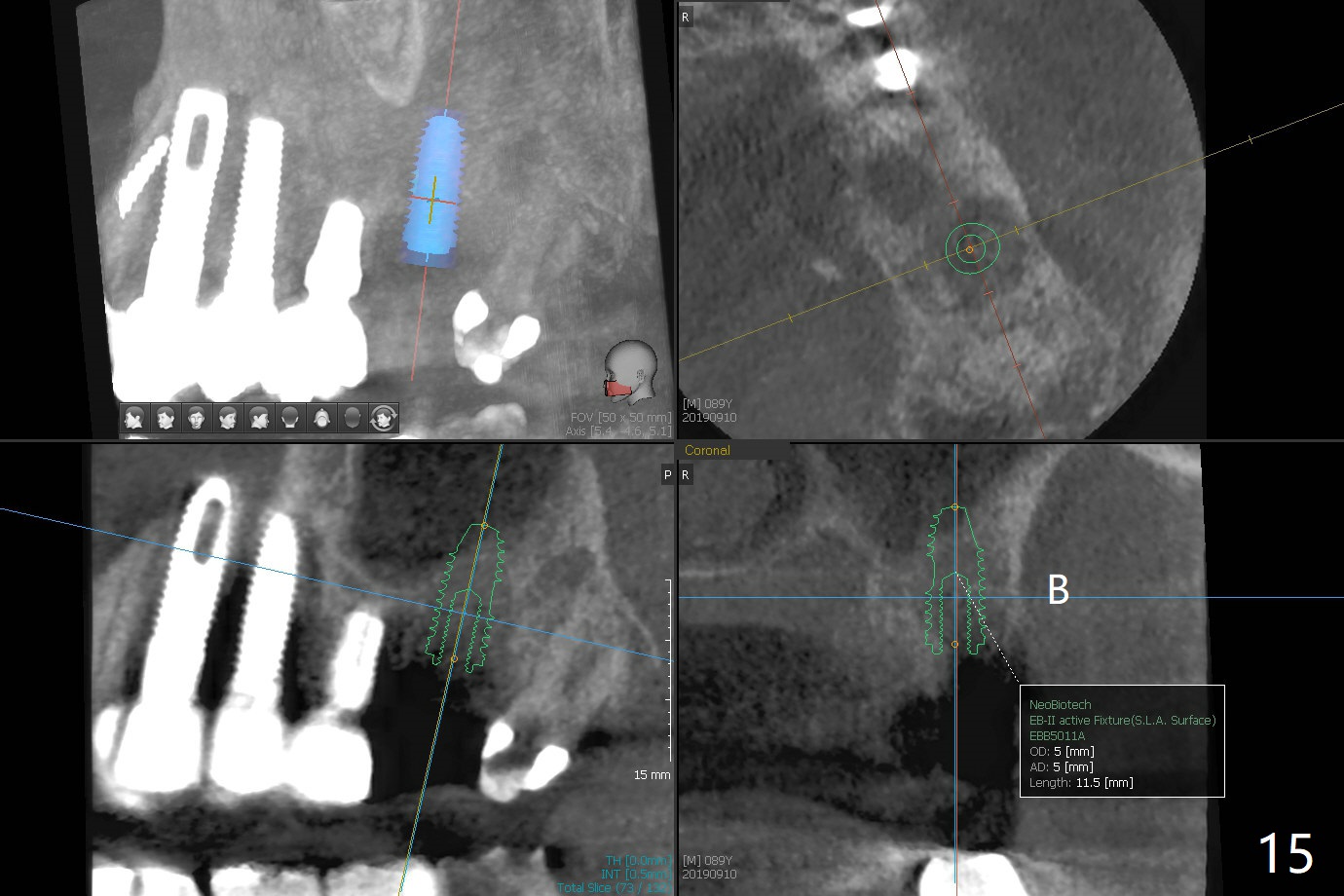
The 7x14 mm implant at #15 of a 89-year-old man is found to be loose ~ 1 year post cementation (Fig.1). After implant removal and debridement, bone graft is placed (Fig.2 G); the mesiocervical caries of the 3rd molar is removed, but not filled (*). With collagen membrane fixed with Chromic gut suture (Fig.3), setting acrylic is applied in the edentulous area, including the mesiocervical cavitation of the 3rd molar (Fig.4) for further retention. Bone graft gets lost following socket preservation at #31 with periodontal dressing. When the bone graft matures, a new implant (Fig.6 green) will get primary stability from the native bone, i.e., coronal to the sinus floor (Fig.5 F). The acrylic dressing (Fig.7 A) with a portion locking to the undercut of the neighboring crown (*) remains in place 5 weeks postop. When the dressing is cut off, the bone graft is exposed with odor (Fig.8,9 *). Periodontal dressing is applied. The distolingual portion of it gets lost due to brushing a day later. When he returns, the dressing is removed (Fig.10). It appears that the growing in gingival margin is pushing the bone graft out. A moment later after just a few rounds of swallowing, more graft is lost (Fig.11). We would love to leave the wound open, but the senior citizen complains of air leaking and requests reapplication of periodontal dressing. The bone graft is almost gone when the 2nd periodontal dressing is removed nearly 2 months postop (Fig.12). The tooth sensitivity disappears when MO caries is taken care of. The socket has a dimple 5 months postop (Fig.13), although it is filled with bone graft (Fig.14). Due to low bone density (~500 HU), sinus lift is required for implant stability with PRF (Fig.15). In fact the lab chooses not to do sinus lift.
Return to Upper Molar Immediate Implant, Trajectory II 19 21 31 Xin Wei, DDS, PhD, MS 1st edition 04/06/2019, last revision 10/15/2019