

|
|
|
|
|
|
|
|
|
|
|
Expand Dense Bone
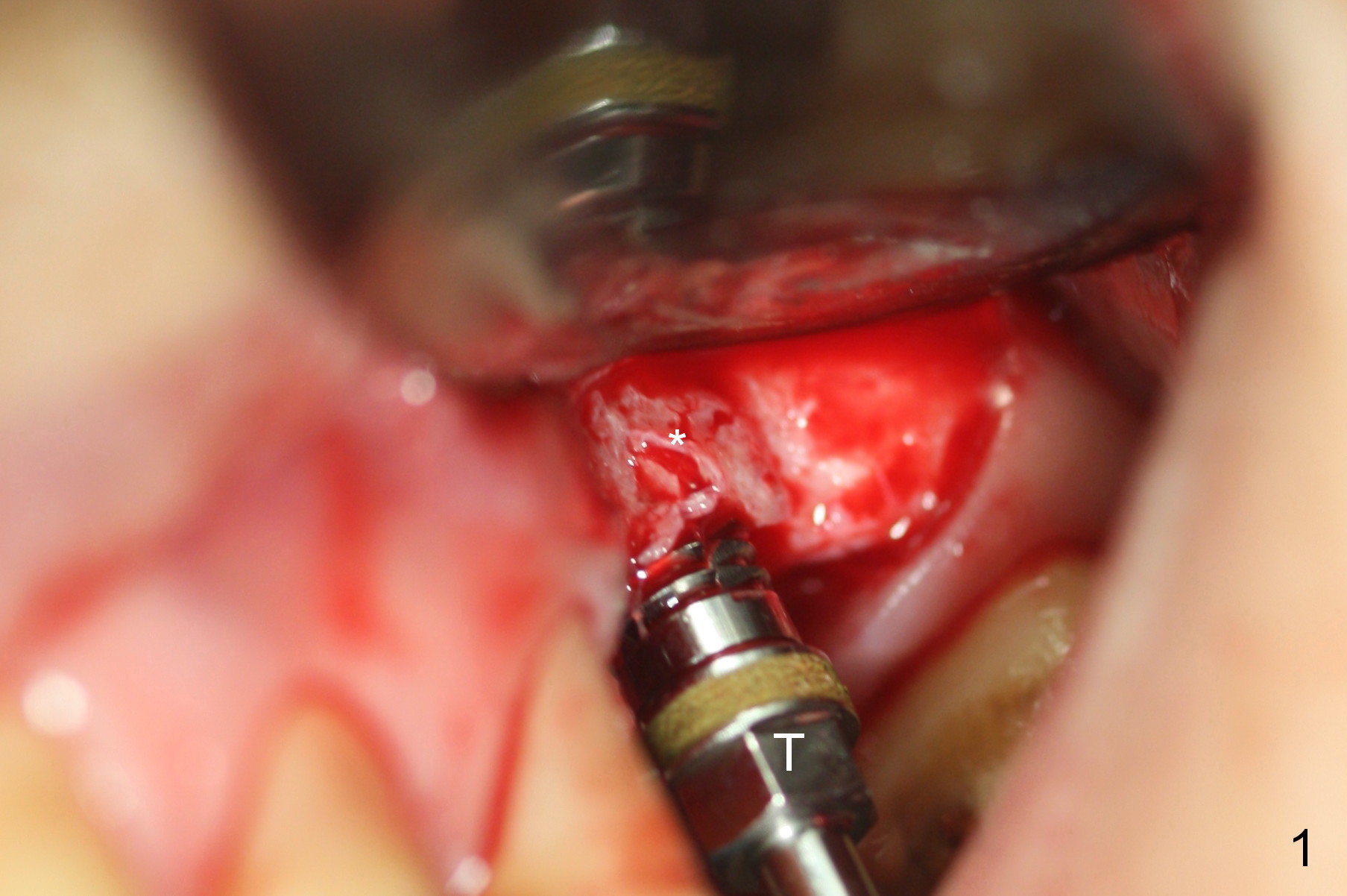
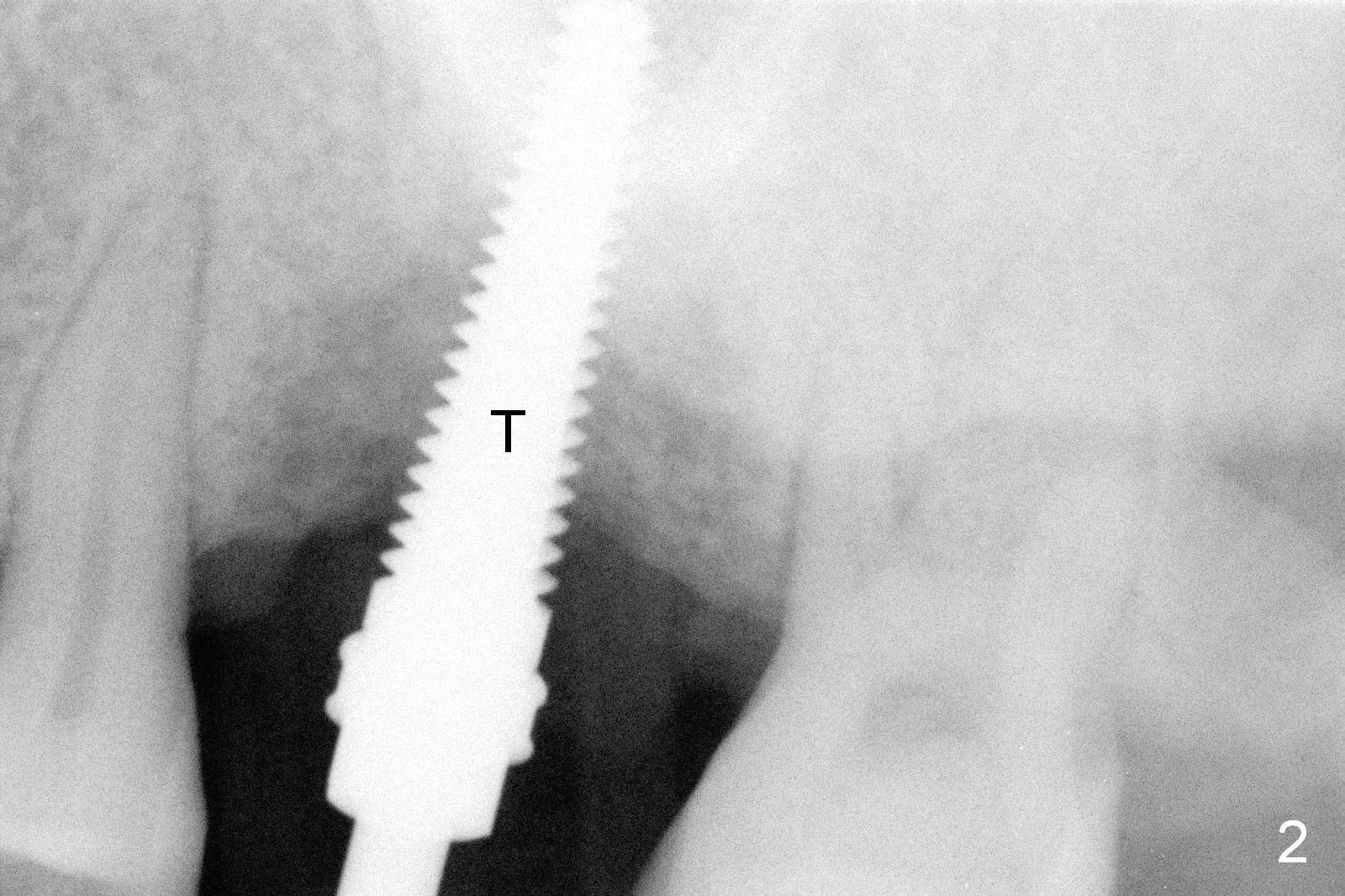
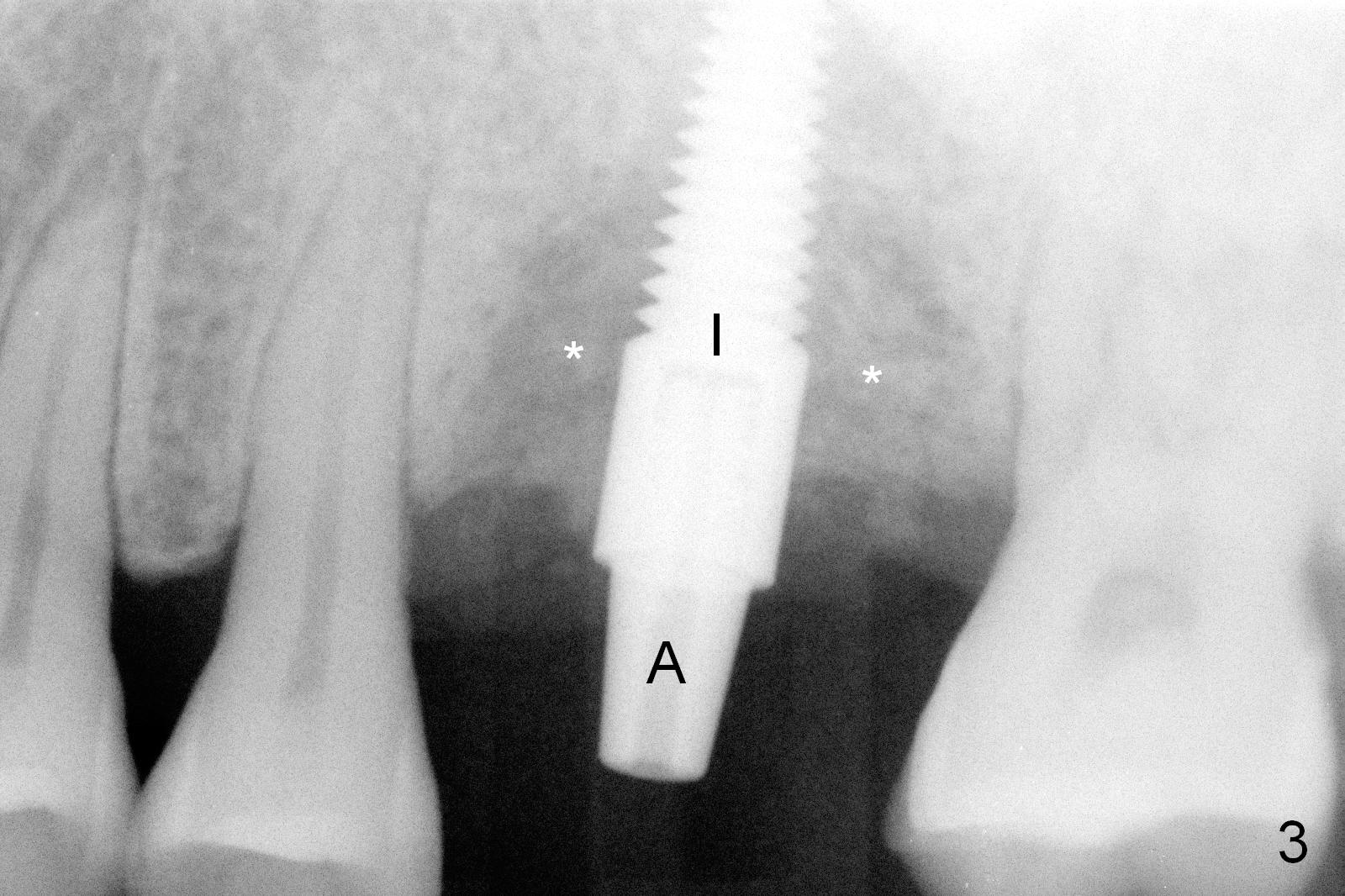
After incision and flap reflection, the crest appears to be composed of the buccal and palatal plates (fusion of two layers of the cortical bone). The crest is narrow and dense. Bone expansion starts with using a surgical fissure bur to make a slot between the buccal and lingual plates, followed by bone scalpels and bone blades. The bone is dense; bone expansion extends ~ 9 mm. A 1.6 mm pilot drill is used at the depth of 14 mm, followed by 2.6, 3.0 and 3.4 mm bone expanders. Both the buccal and lingual plates are expanded. When a 4.5 mm tap is inserted (Fig.1,2 T), the buccal plate is shown to be bulging and breaking down (Fig.1 *). Although the tap appears to enter the sinus (Fig.2), there is no air leakage. A 4.5x17 mm tissue-level implant is placed (Fig.3 I) with insertion torque >60 Ncm. Allograft and Osteogen are placed around the bulging buccal and lingual plates (Fig.3 *). Collagen membrane with a hole in the center is fixed around a 3.5x5 mm abutment (Fig.3 A). An immediate provisional is fabricated mainly for wound protection and perio dressing fixation.
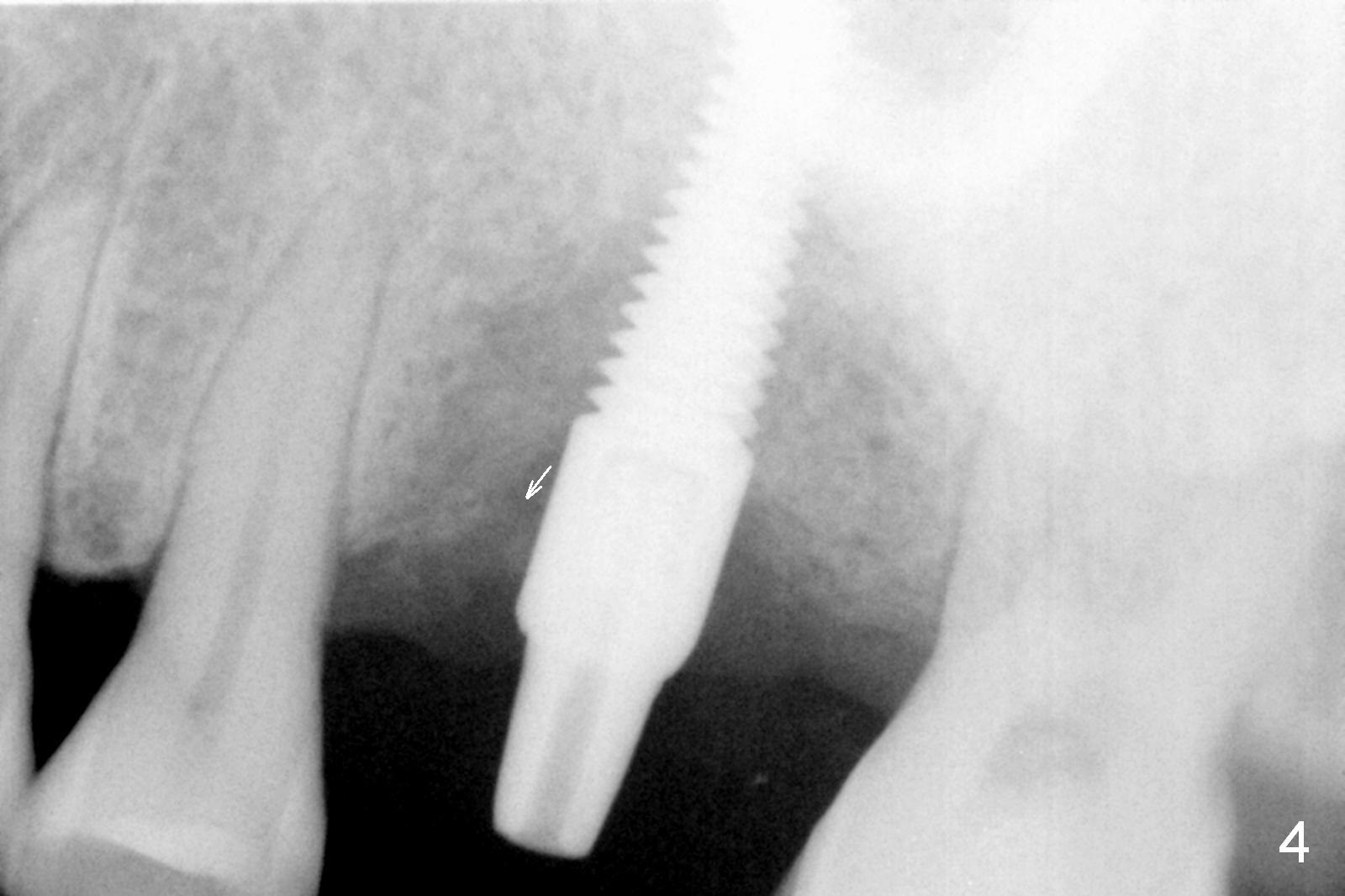
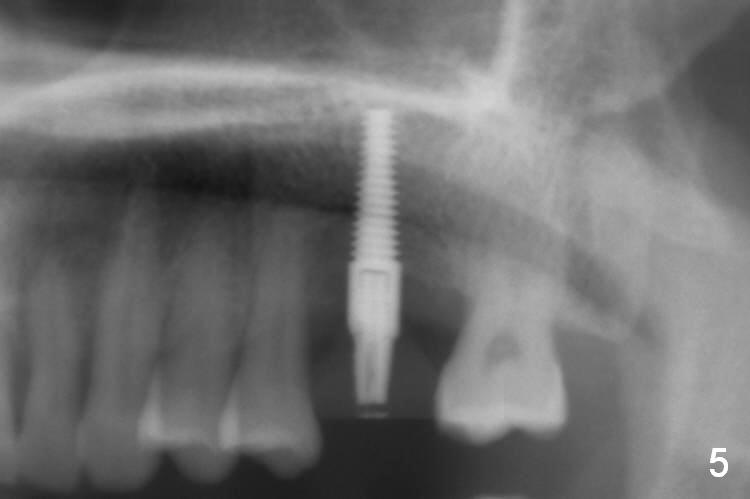
The patient returns 3 months postop; the bone graft appears to have been displaced mesioocclusally (Fig.4 arrow). The apex of the implant is not close to the sinus floor (Fig.5). The buccal plate does not look atrophic 3.5 months postop (immediately prior to cementation, Fig.6 *).
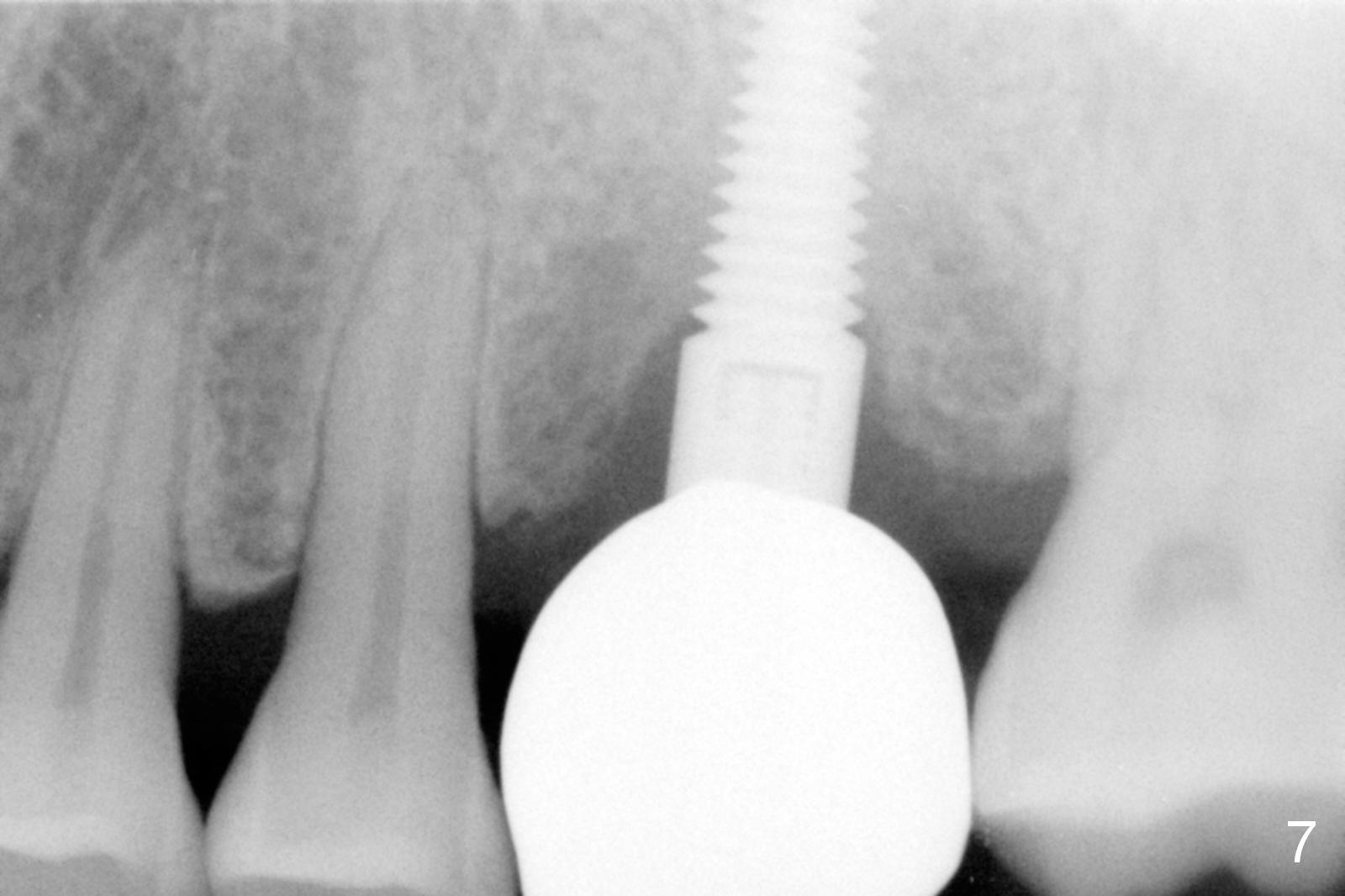
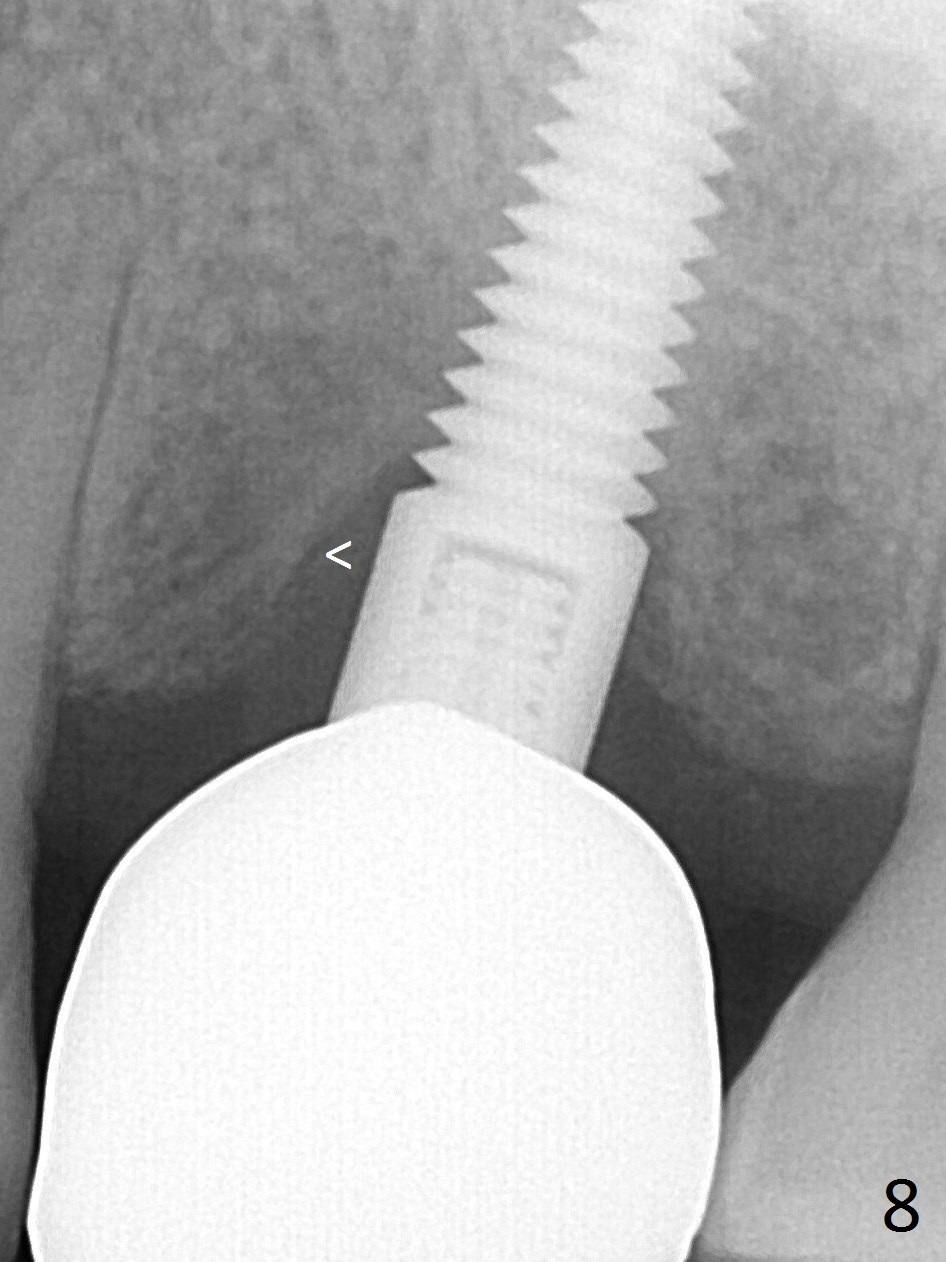
Seven months post cementation, the patient complains of occasional and mild ipsilateral submandibular lymph node tenderness. There is no significant clinical finding, including X-ray (Fig.7). The chief complaint remains the same 1 year post cementation; mesial bone appears to form lamina dura-like structure (Fig.8 <). Is this the earliest sign of periimplantitis? Oral hygiene of this patient is acceptable. The lamina-dura-like structure becomes thicker 1 year 4 months post cementation (Fig.9).
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 10/16/2015, last revision 01/19/2019