
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Severe Bone Loss: Large Immediate Implant
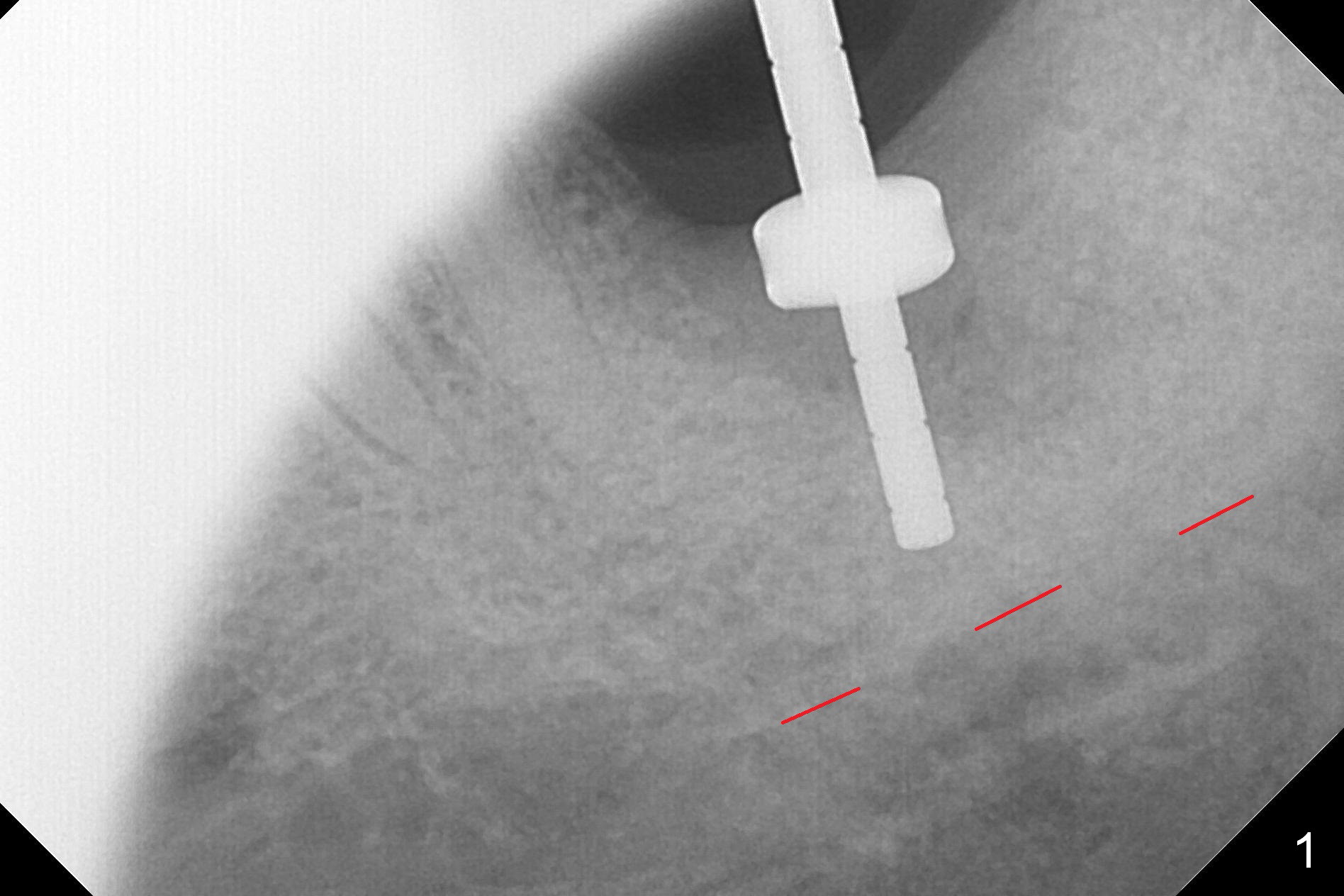
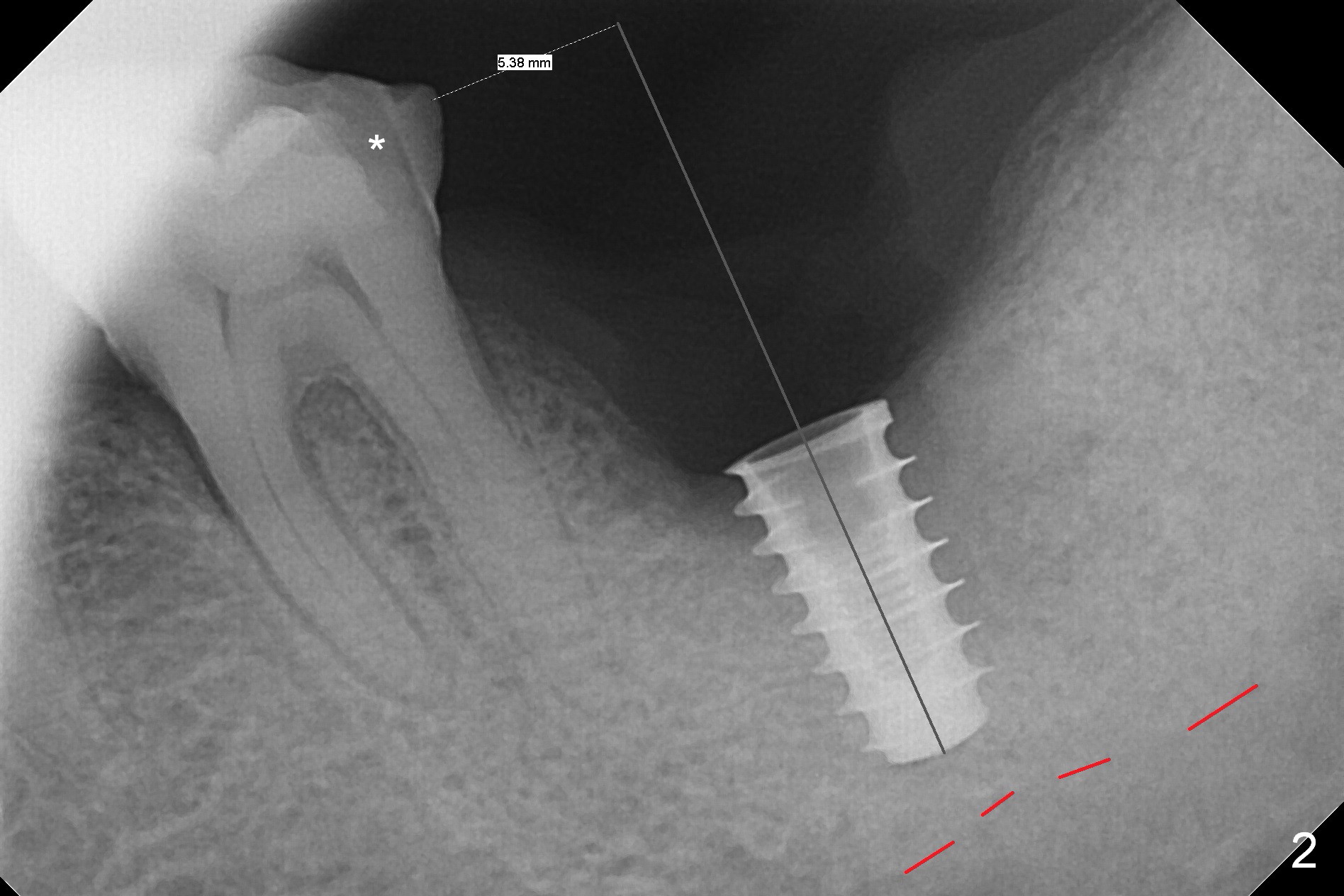
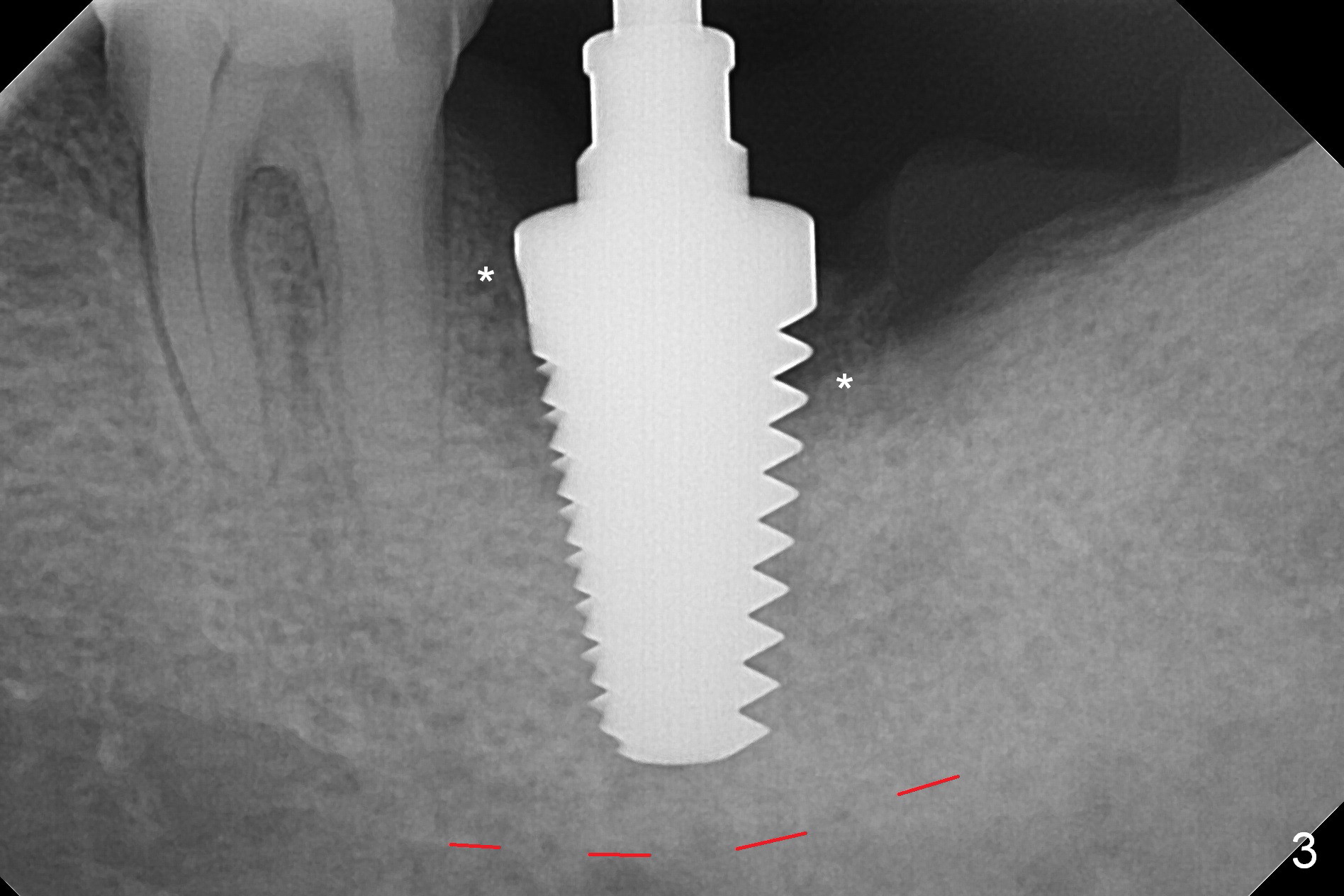
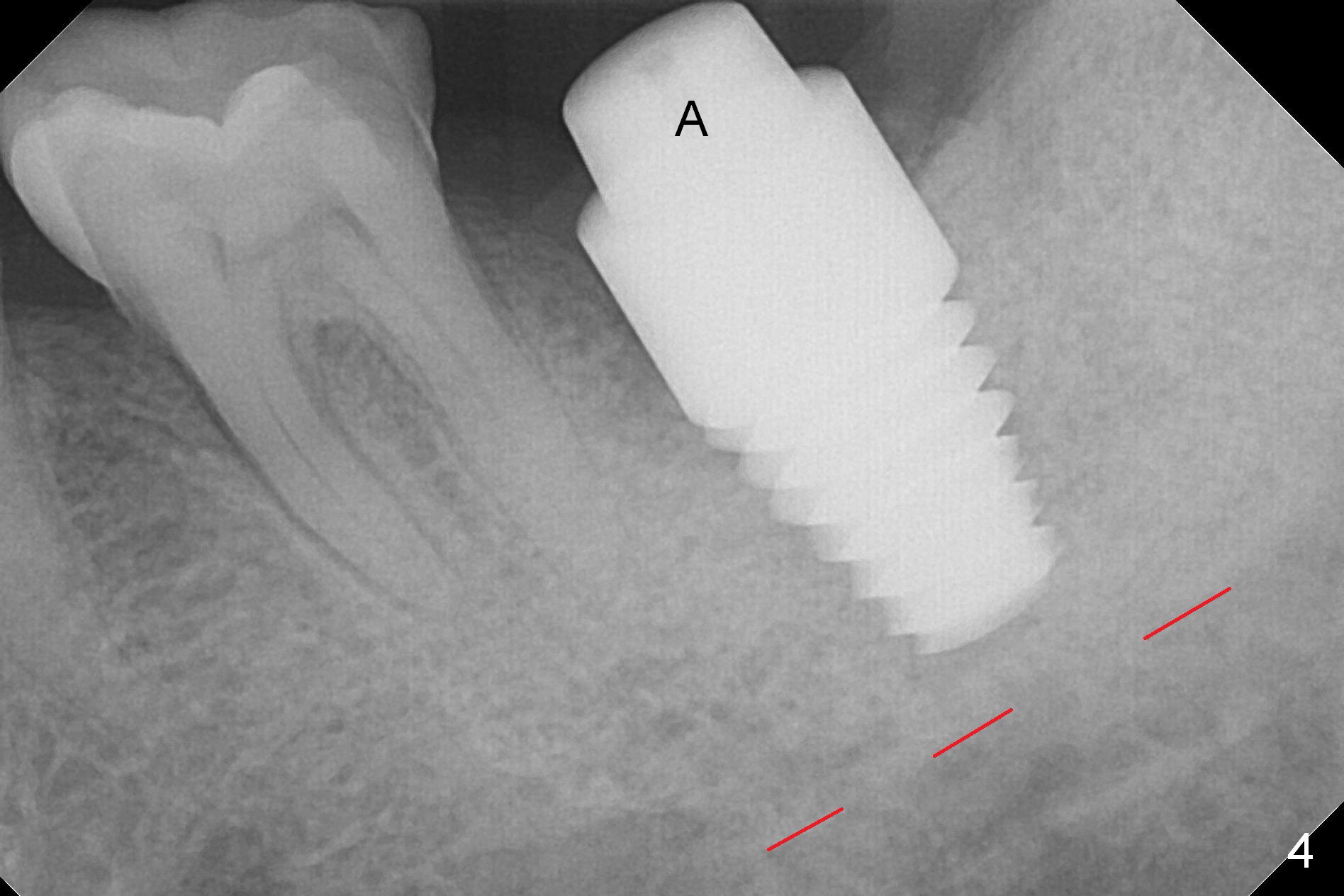
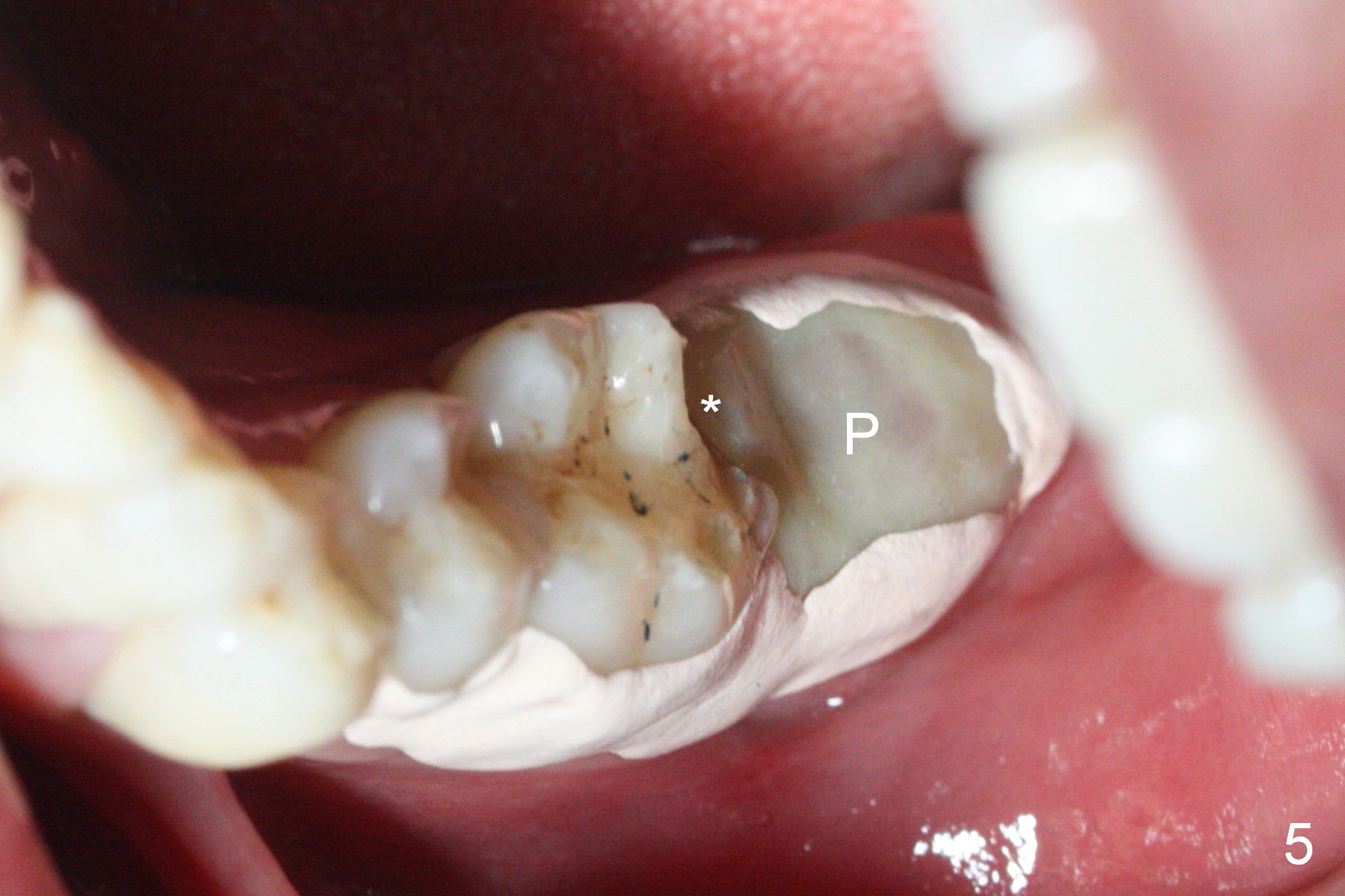
When the tooth #18 is extracted, the buccal and lingual plate are absent. Initial osteotomy is established in the middle of the socket (Fig.1). After 4.3 mm Magic Drill (15 mm from the buccal gingival margin, new bone ~ 4 mm), a 5x9 mm IBS dummy implant is placed with correct trajectory (Fig.2). Since the bone density is seemingly high, the same size of a definitive implant is placed with primary stability. The trajectory is found not ideal after bone graft and insertion of an abutment (data not shown). The stability is lost when the trajectory is changed. No primary stability is achieved with a larger (5.5x9 mm) implant. Tatum tapered taps (6x17, 7x17 and 8x17 mm) are used. The latter obtains stability with contact with the mesial and distal crests (Fig.3 *). A 8x14 mm tissue-level implant is placed with insertion torque ~ 55 Ncm (Fig.4). A 6x3 mm abutment (Fig.4 A) is placed to retain an immediate provisional (Fig.5 P). The drawback of the extra large implant is lack of bone buccolingually. Oral hygiene is emphasized so that the buccal and lingual bone have chance to regenerate. Fortunately there appears to be no paresthesia postop.
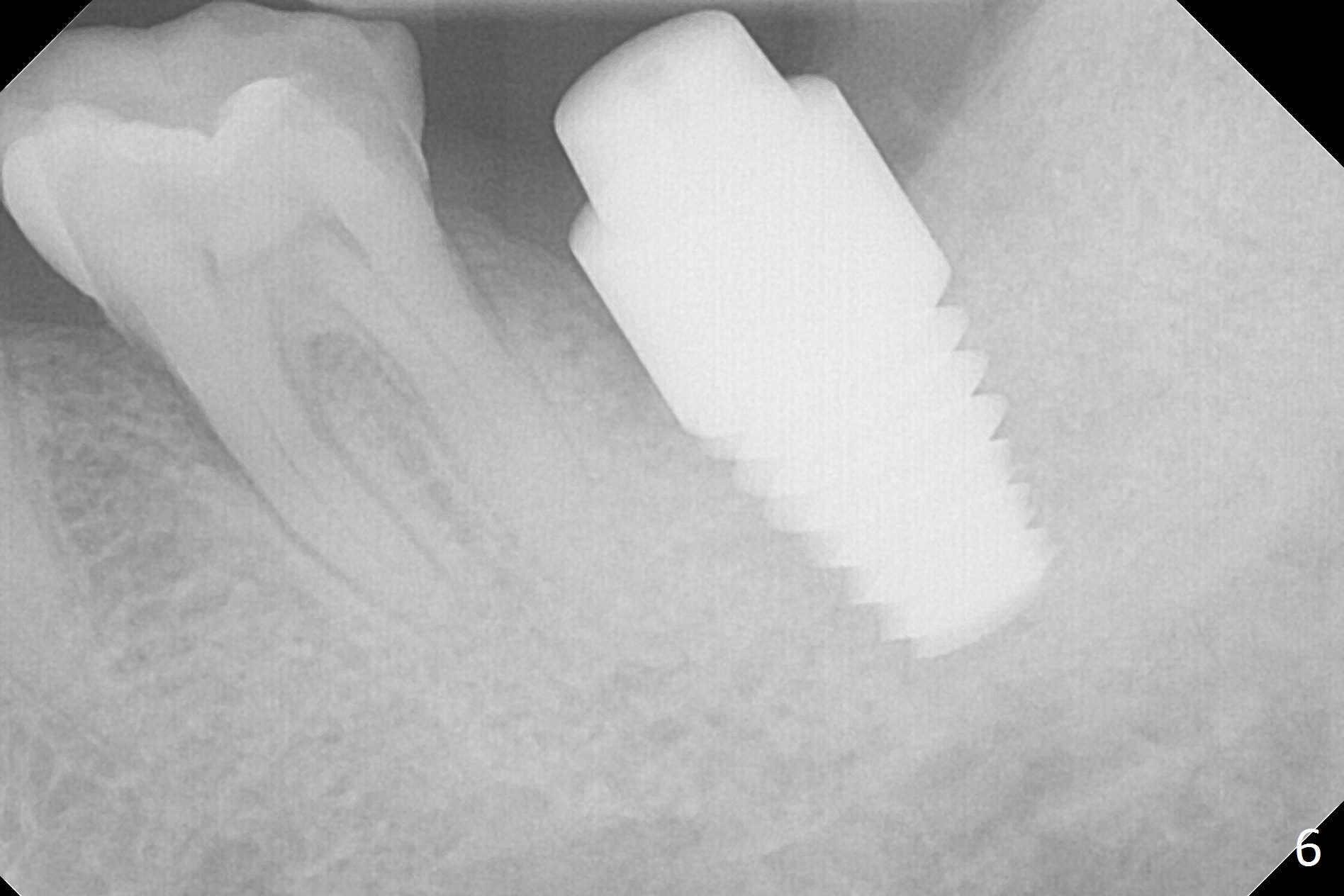
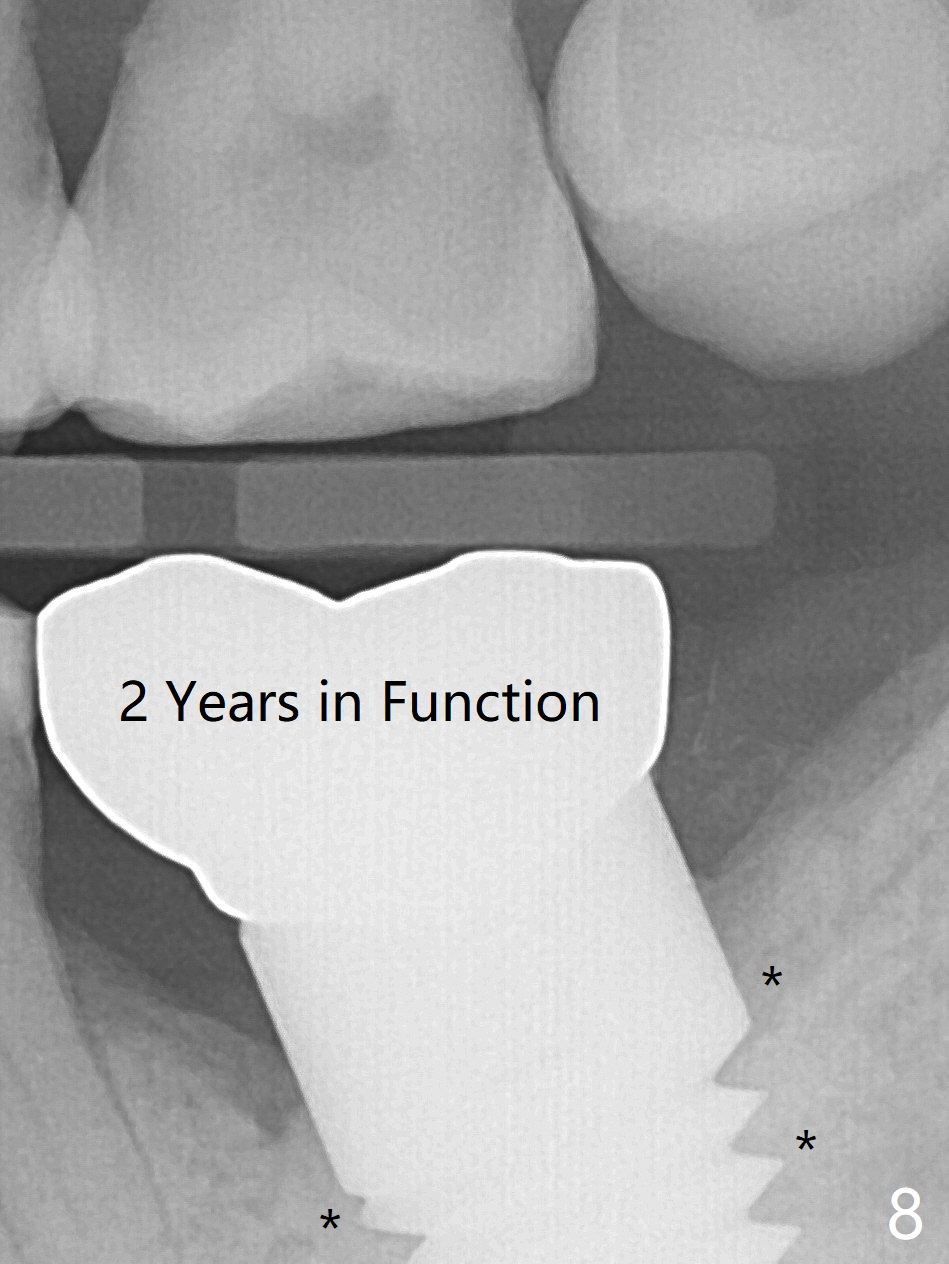
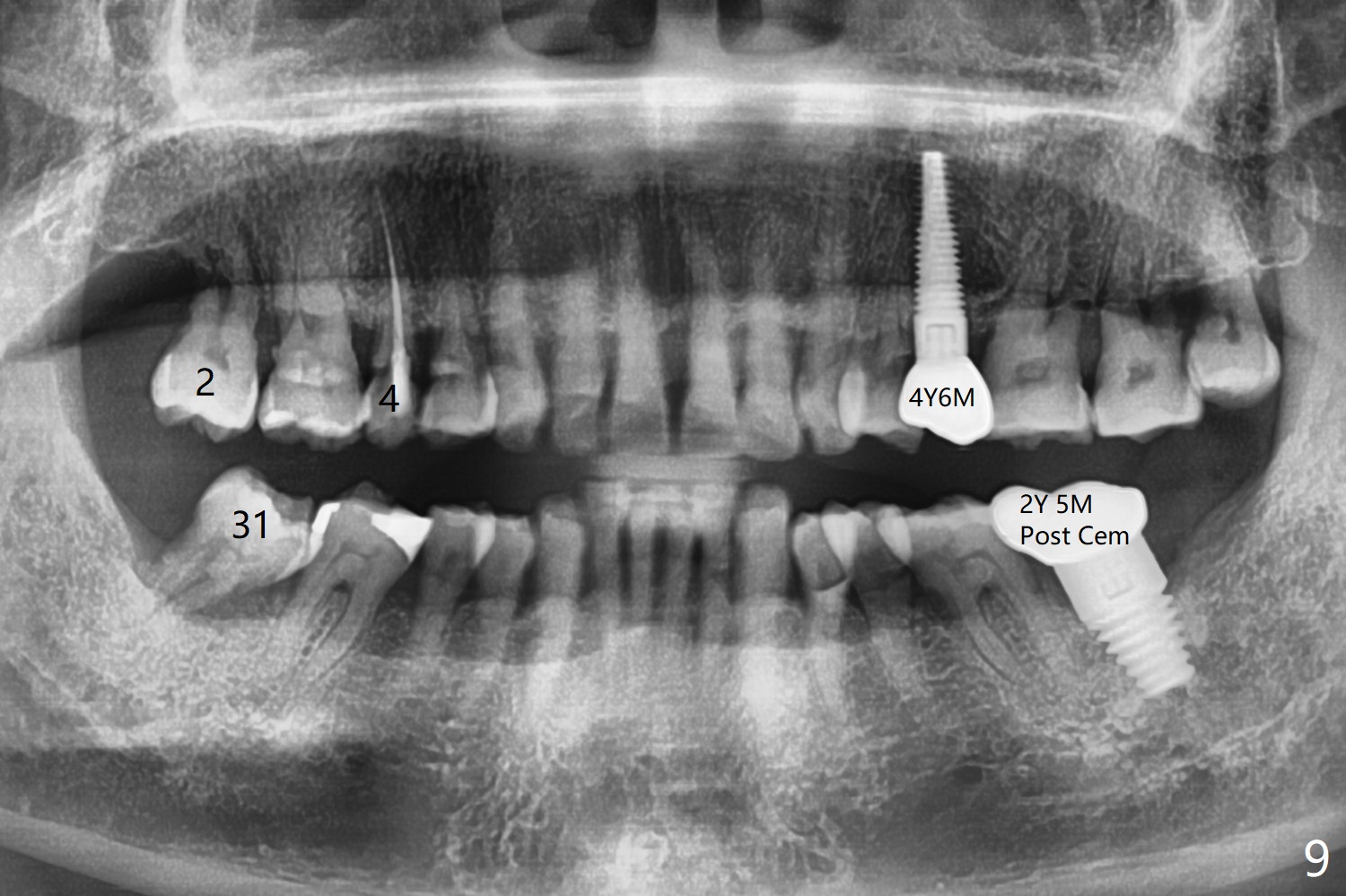
It appears that the patient chews on the left postop, since the provisional perforates with loose abutment nearly 3 months postop and the tooth #3 has occlusal sensitive chip. The implants seems to have osteointegrated (Fig.6). To improve oral hygiene, the provisional is not recemented. The patient will return for impression in 2 weeks. It appears that there is short healing time for large implant. There is no bone loss 7 months post cementation (Fig.7). The buccal gingiva is lightly erythematous without tenderness 1 year 7.5 months post cementaion. Water pik is being used, although chronic periodontitis is not under control. Retrospectively, surgery should be shifted to socket preservation when a moderate implant (5 or 5.5 mm) fails to achieve primary stability. The extra large implant (8 mm for example) leaves a little gap buccolingually. Guided surgery would allow precise placement of the moderate implant without change in trajectory. The crown becomes loose because of occlusal perforation and limited vertical space. When a new crown is cemented, the bone density around the coronal threads is high (Fig.8 *). While the bone remains stable at #4 (6 months post RCT), 13 (4 years 6 months post cementation) and 18 (2 years 5 months post cementation), there is severe bone loss at #2 and 31 (Fig.9).
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
Trajectory II
#13,
31,
4
Xin Wei, DDS, PhD, MS 1st edition 01/17/2017, last revision 04/13/2020