








|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
One-Piece Implants For Narrow Maxillary Posterior Crest
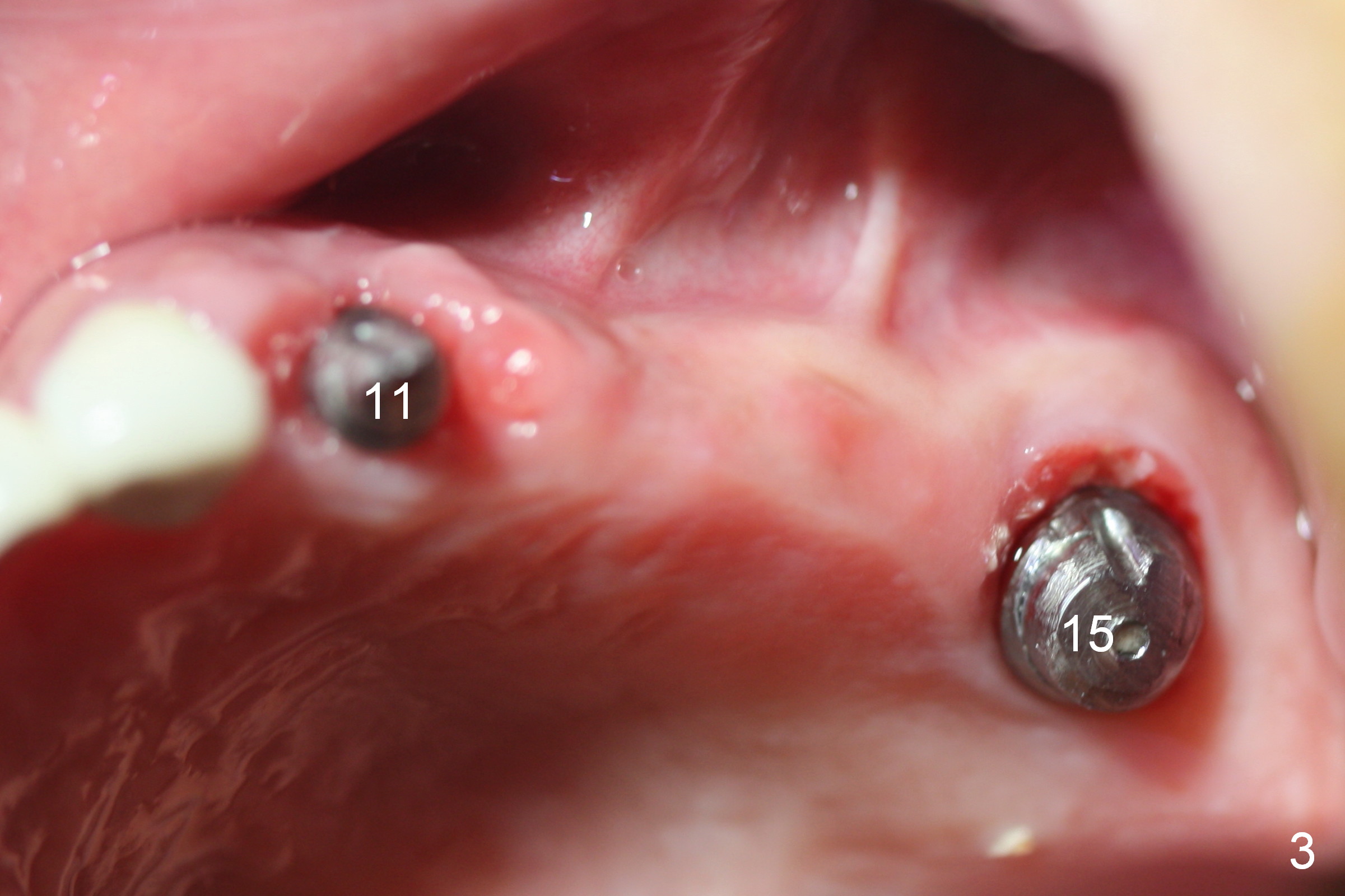
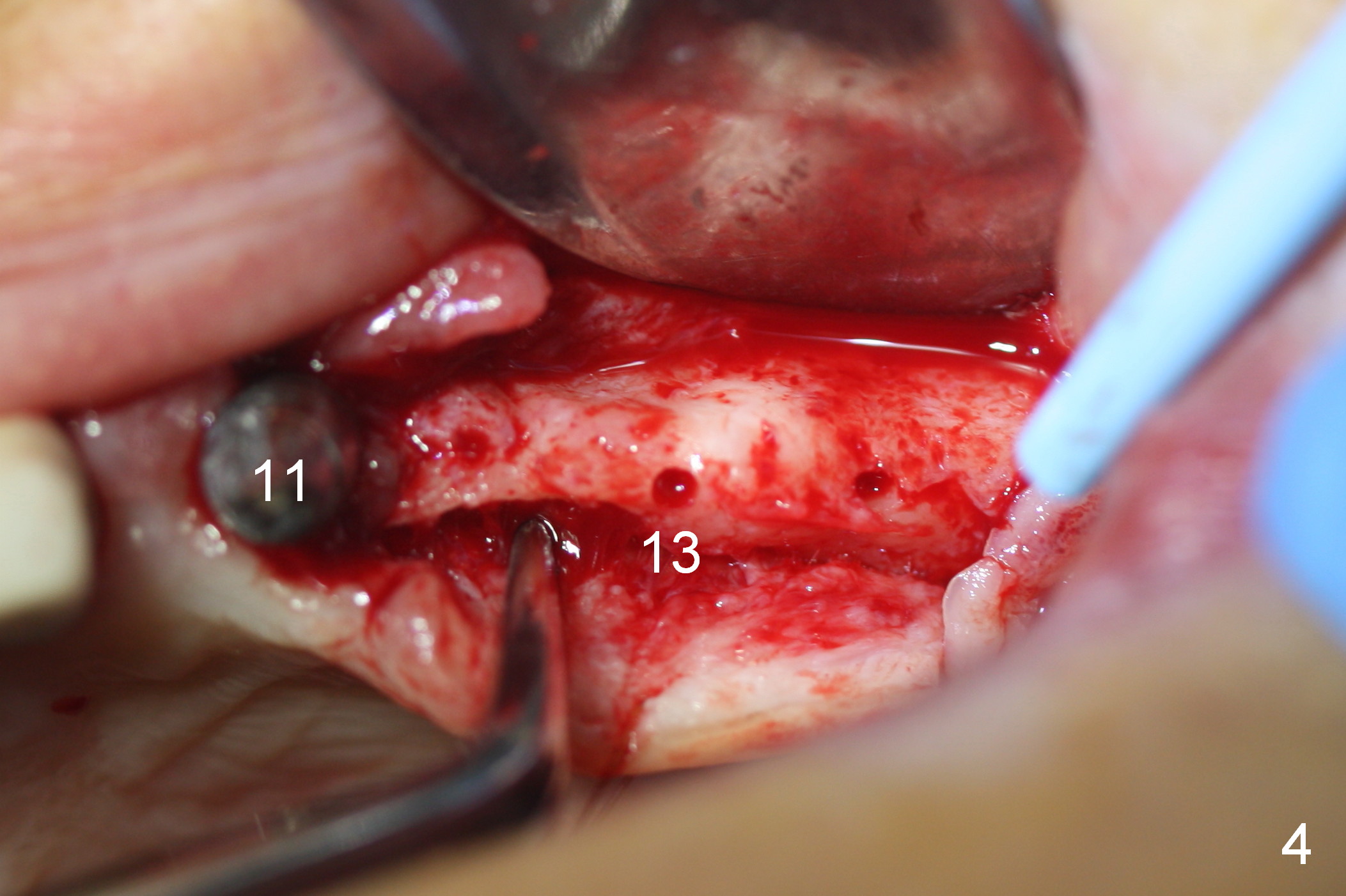
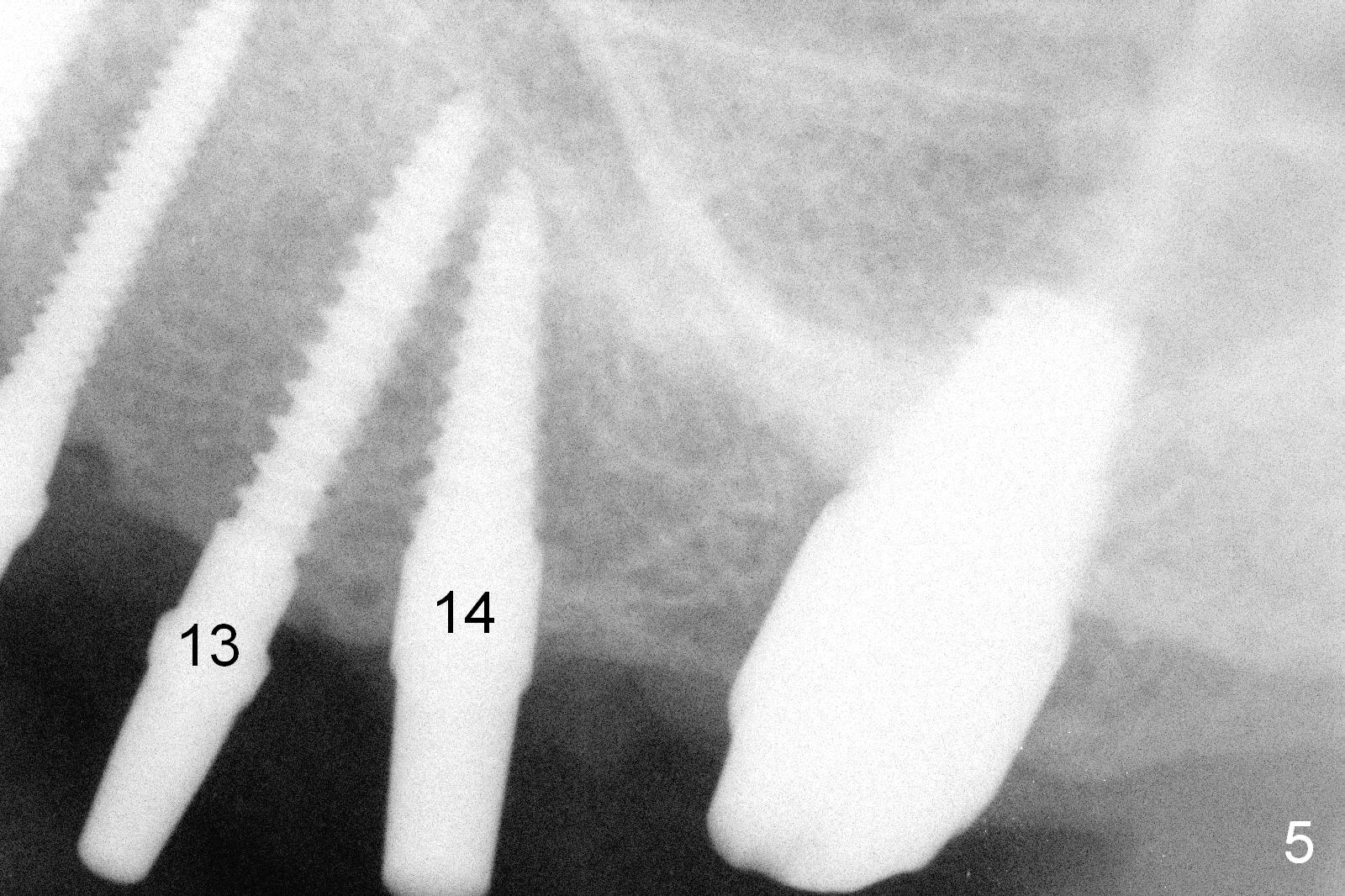
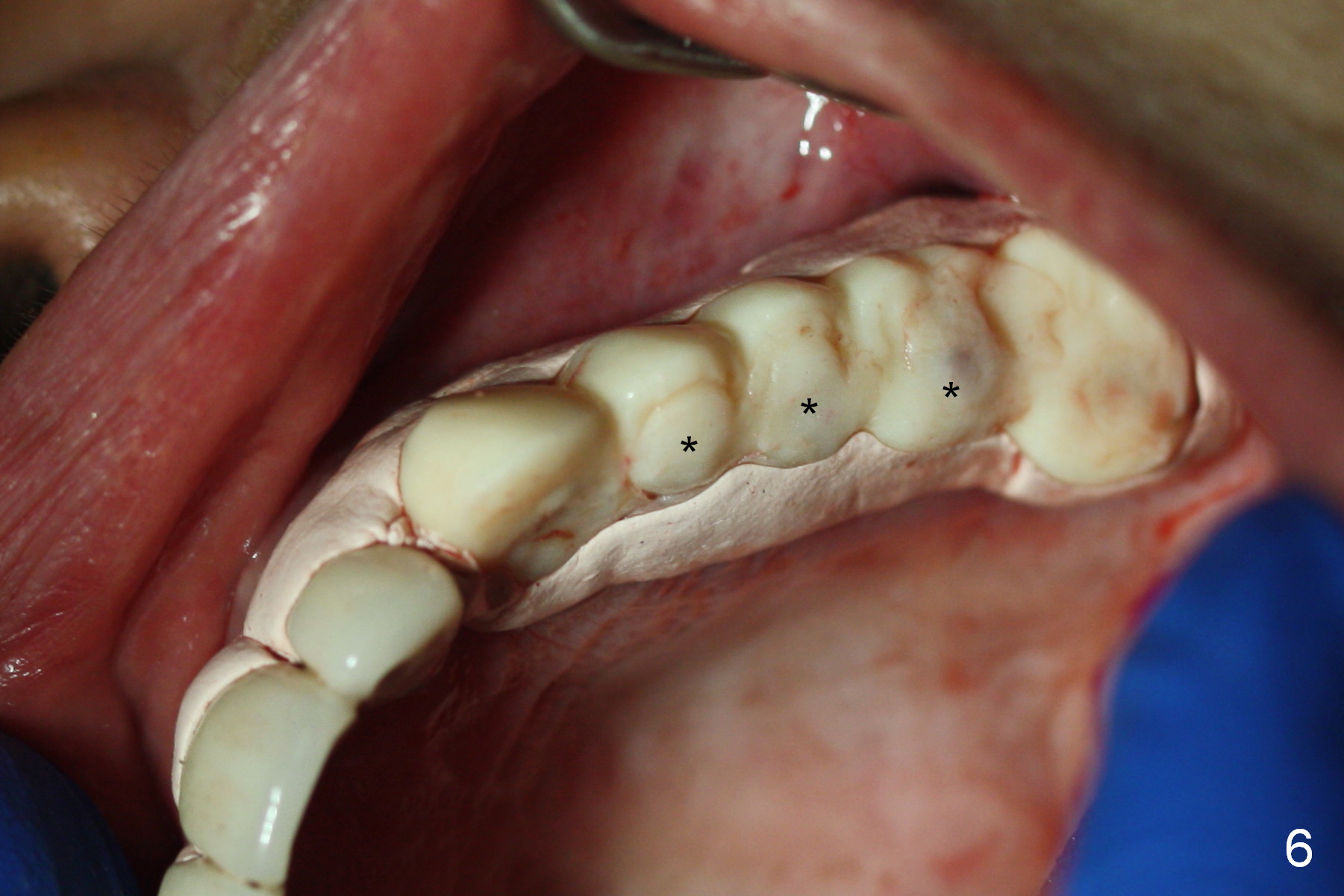
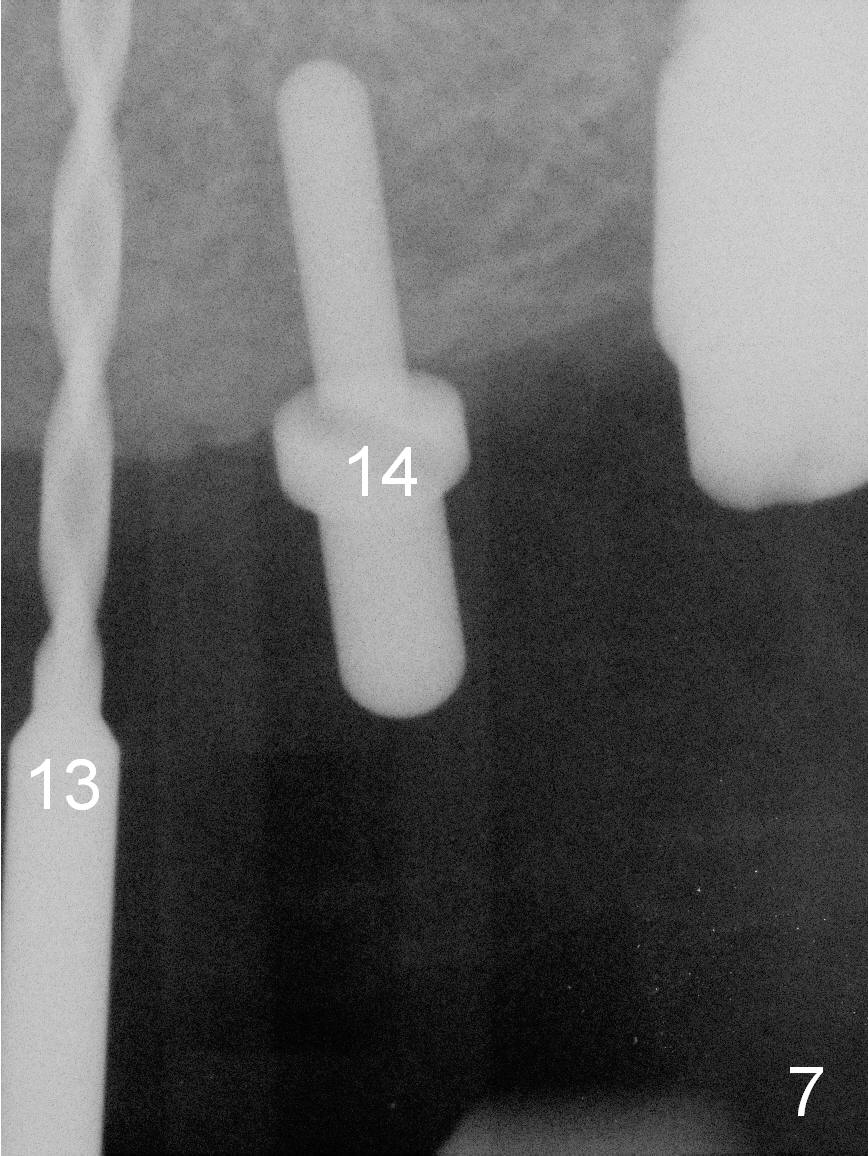
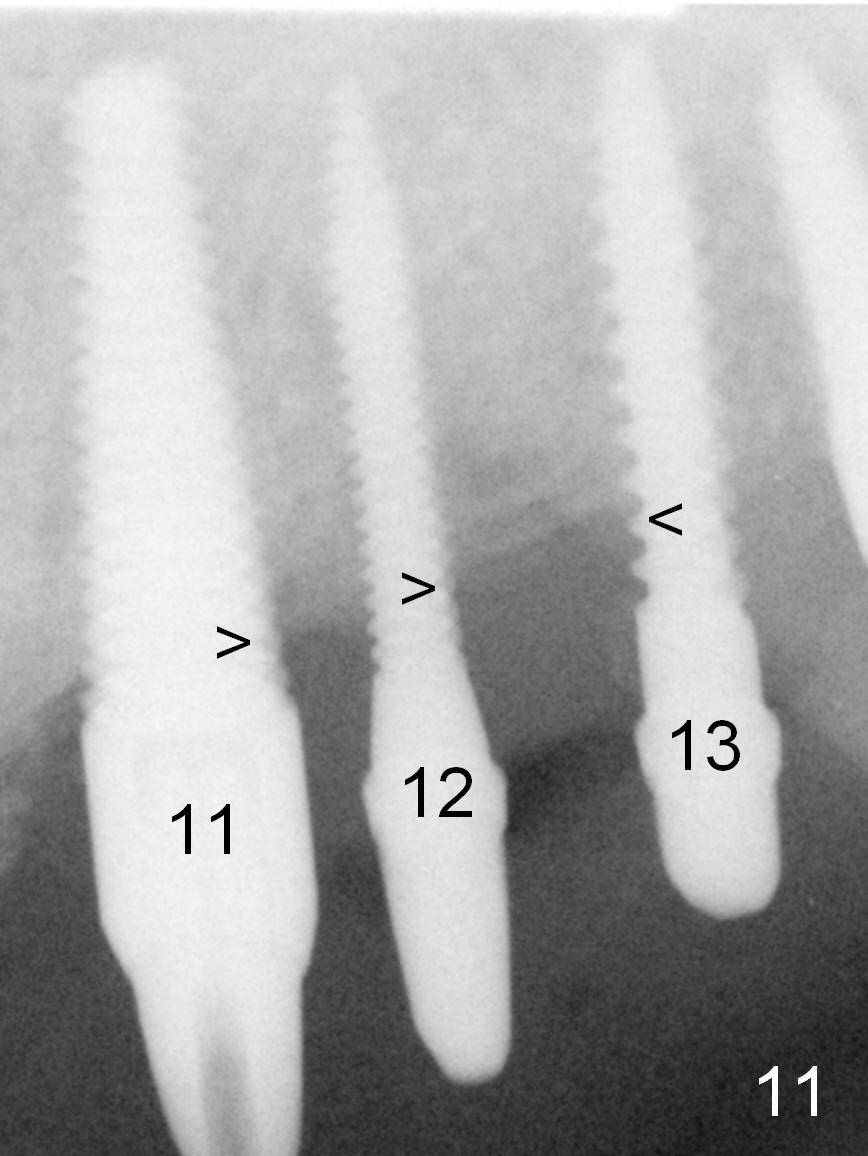
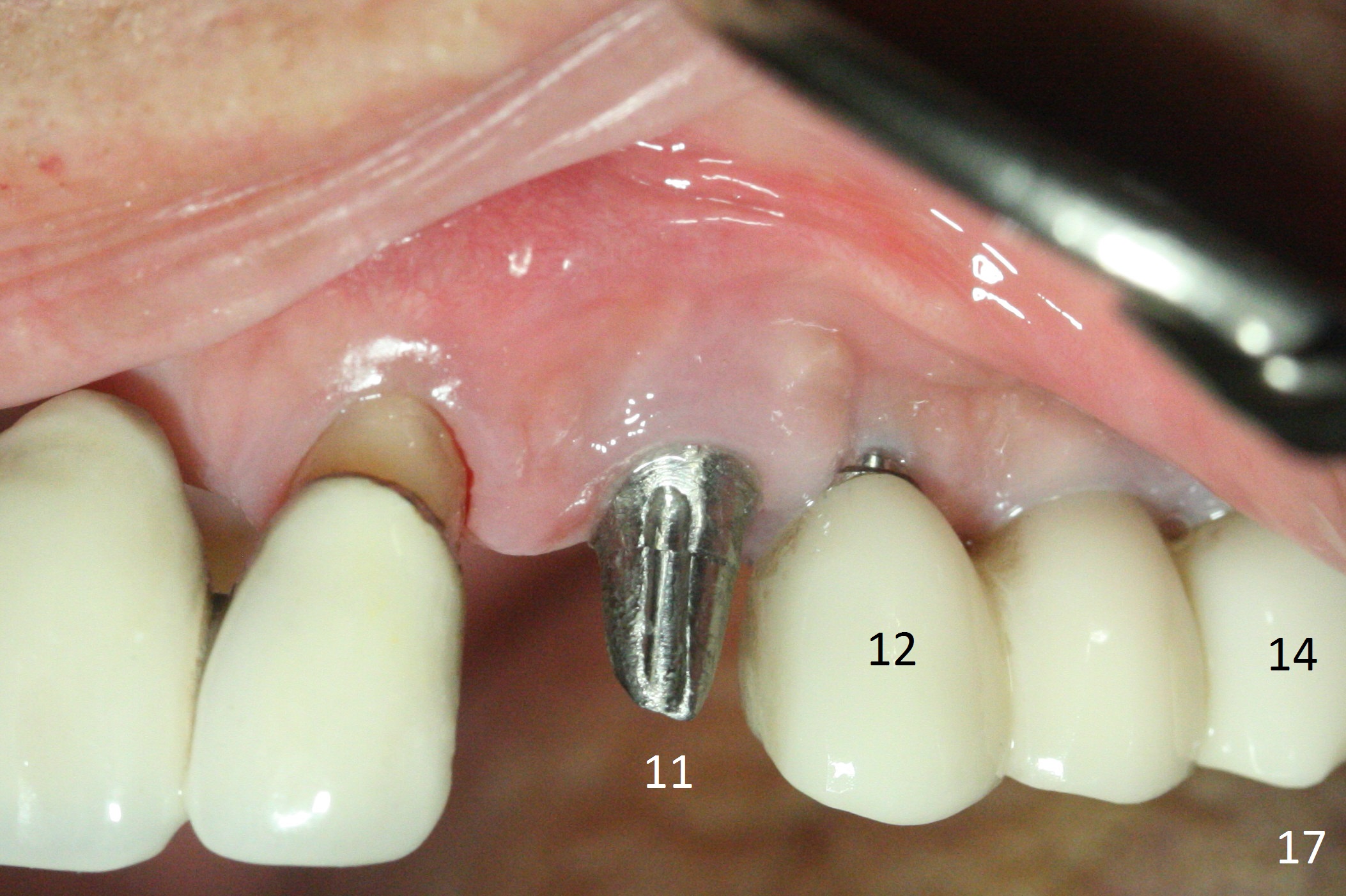
Two months and 1 week postop (#11,15 implant placement), the buccal gingival defect at the site of #11 (Fig.1,2 <) is much smaller than that 2 weeks postop. The narrow crest between #11 and 15 implants (Fig.3) is shown best when the buccal and lingual flaps are raised (Fig.4). Since the patient is extremely nervous about the surgery, a separate bone graft procedure is not practical. The goal at this moment is to place 2.5, 3 and 3.5 mm 1 piece implants at the sites of #12,13 and 14, respectively (all 14 mm long). Osteotomy are prepared accordingly. When a 2.5 mm implant is attempted to be placed at #12, it looks too big for the bone. Instead a 2x14 (2) mm implant is placed with insertion torque <15 Ncm; the 2.5 mm implant is placed at #13 ~ 15 Ncm (Fig.5). The bone density of initial osteotomy at #14 is felt to be low; the subsequent osteotomy is underprep, the insertion torque is >15 Ncm. The original provisional bridge is modified at #12-14. The middle portion of each pontic is removed so that the bridge is seated passively before reline (Fig.6 *).
The trajectory of #13 and 14 (Fig.5) could have been detected and then corrected if a longer parallel pin at #14 were used (Fig.7) and the X-ray were analyzed more carefully. It is difficult to take this early intraop PA when long drills remain in osteotomies. In this case, panaramic X-ray should be taken.
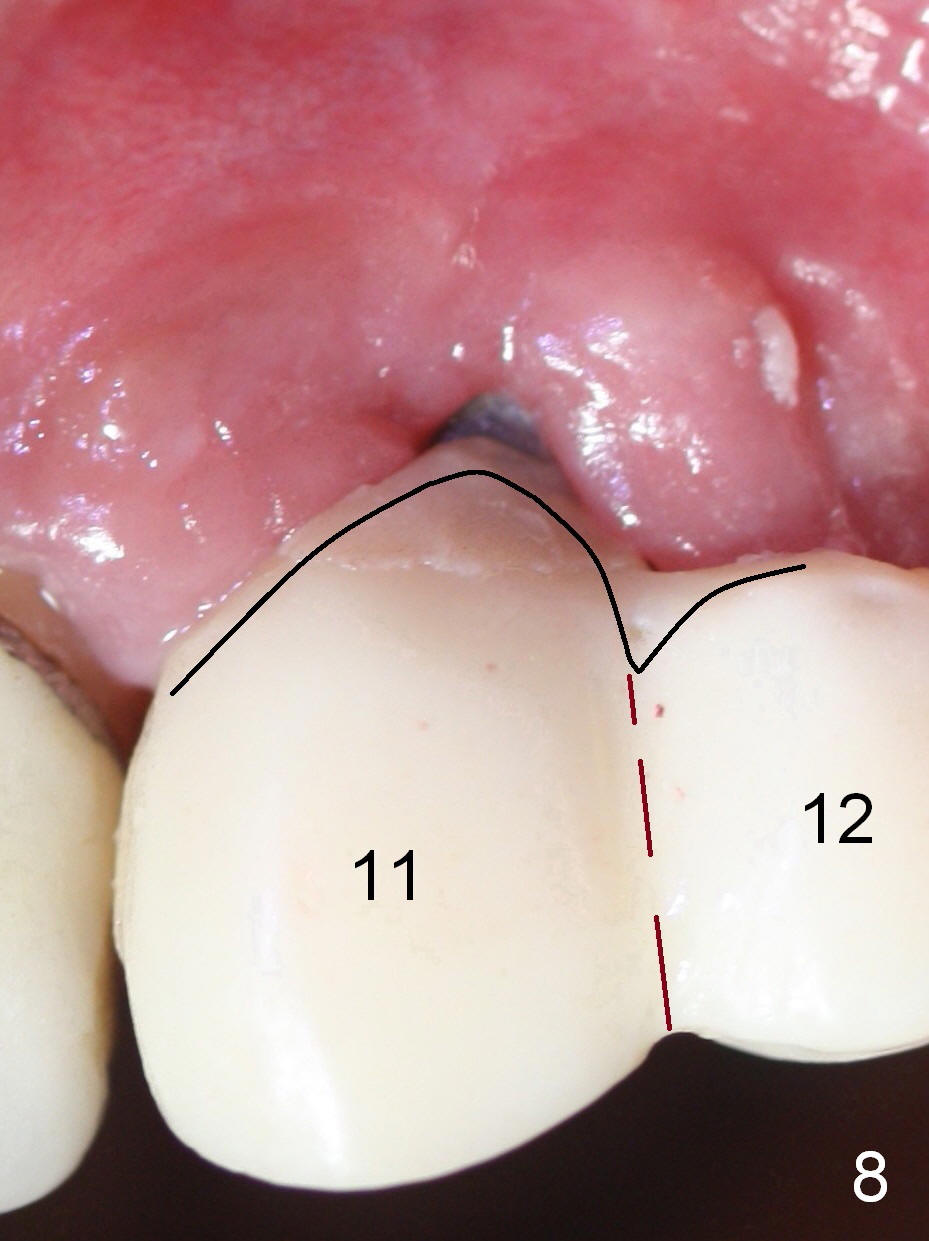
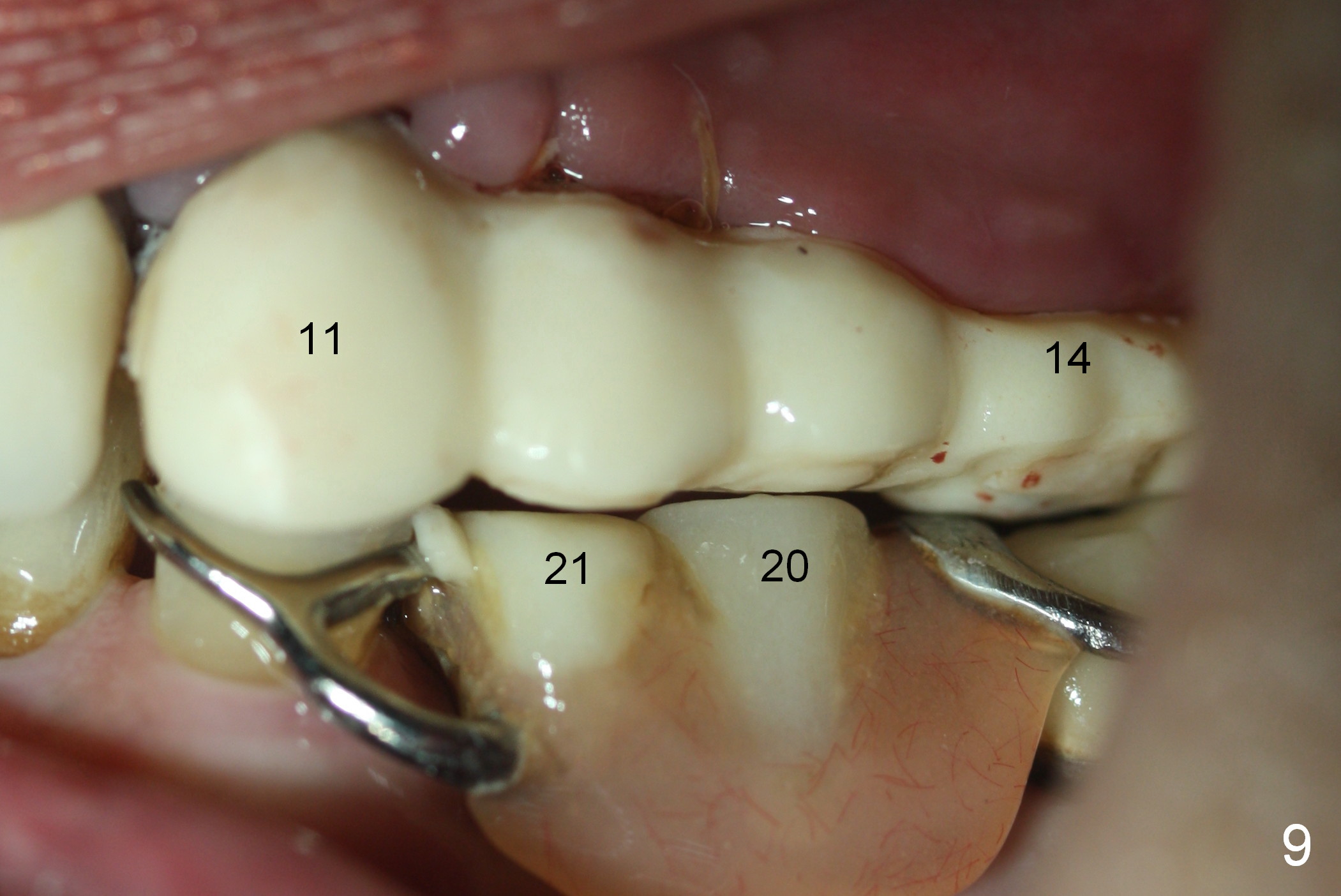
The new provisional will be kept in place as long as possible (4-6 months). In fact, the lower edentulous space is restored by a RPD (denture teeth: #18,20,21 (Fig.9),28-31). Before final impression, the provisional will be sectioned between #11 and 12 (Fig.8 brown dashed line). The retainer of #11 is removed and margin trimming (black line) so that the gingiva may grow incisally.
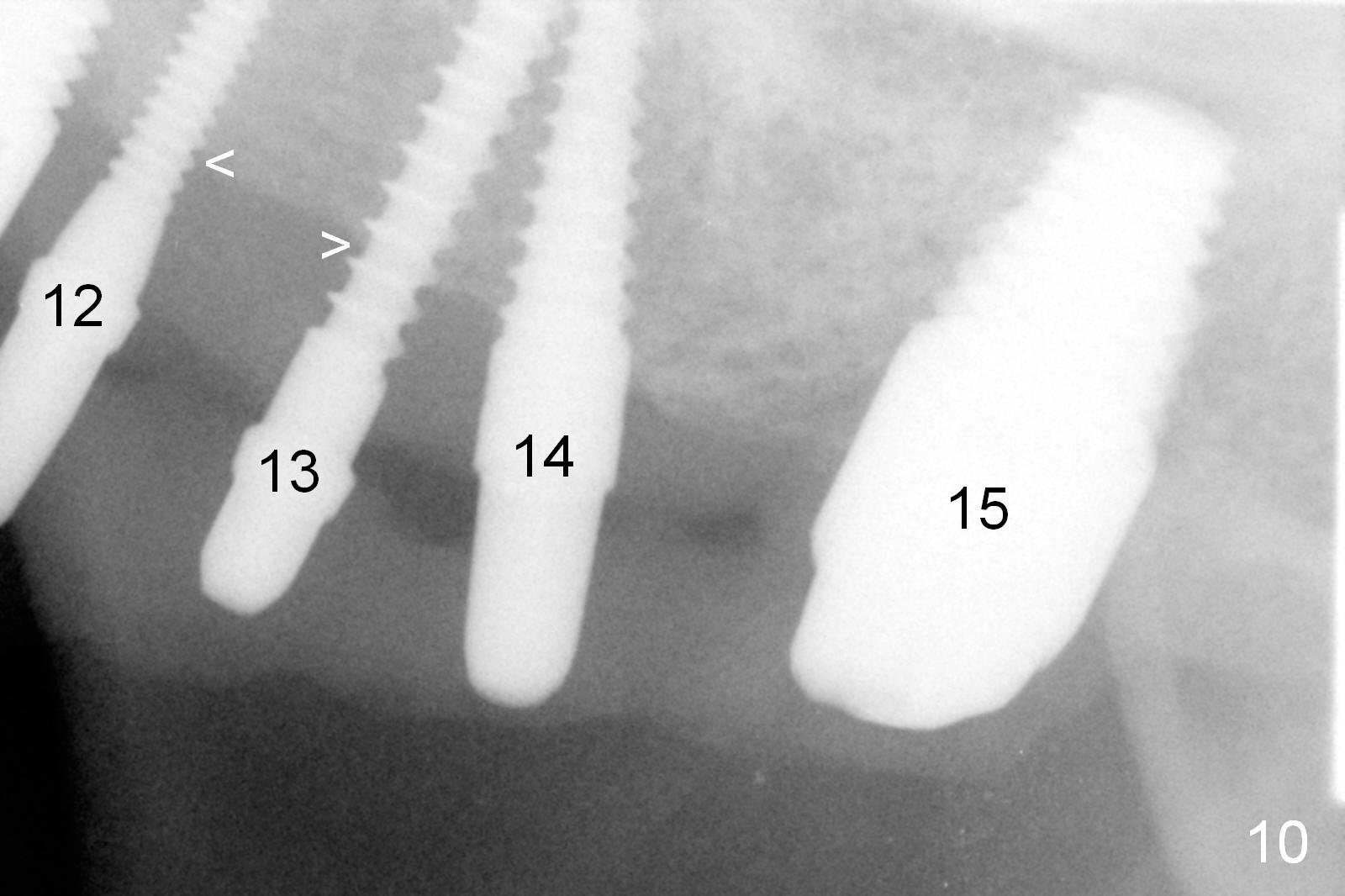
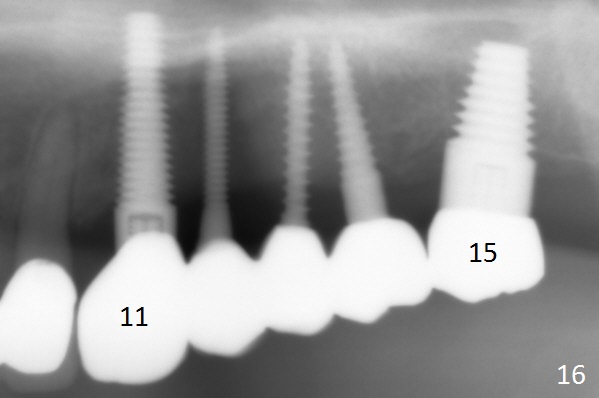
The patient returns for final restoration 4 and 5 months postop (for #12-14 and 11/15, respectively). There appears to be bone loss around the implants at #11-13 (Fig.10,11). Clinically the gingiva looks healthy. In fact it is difficult to insert gingival retraction cords. Laser gingivectomy is performed prior to impression (Fig.12).
The patient is using Water Pik for immediate provisional hygiene so that the gingiva is healthy when permanent crowns are trying in (Fig.13) or removed (Fig.14). The crowns at #12-14 are splinted. The gingiva and bone remain healthy 6 months post cementation (Fig.15,16).
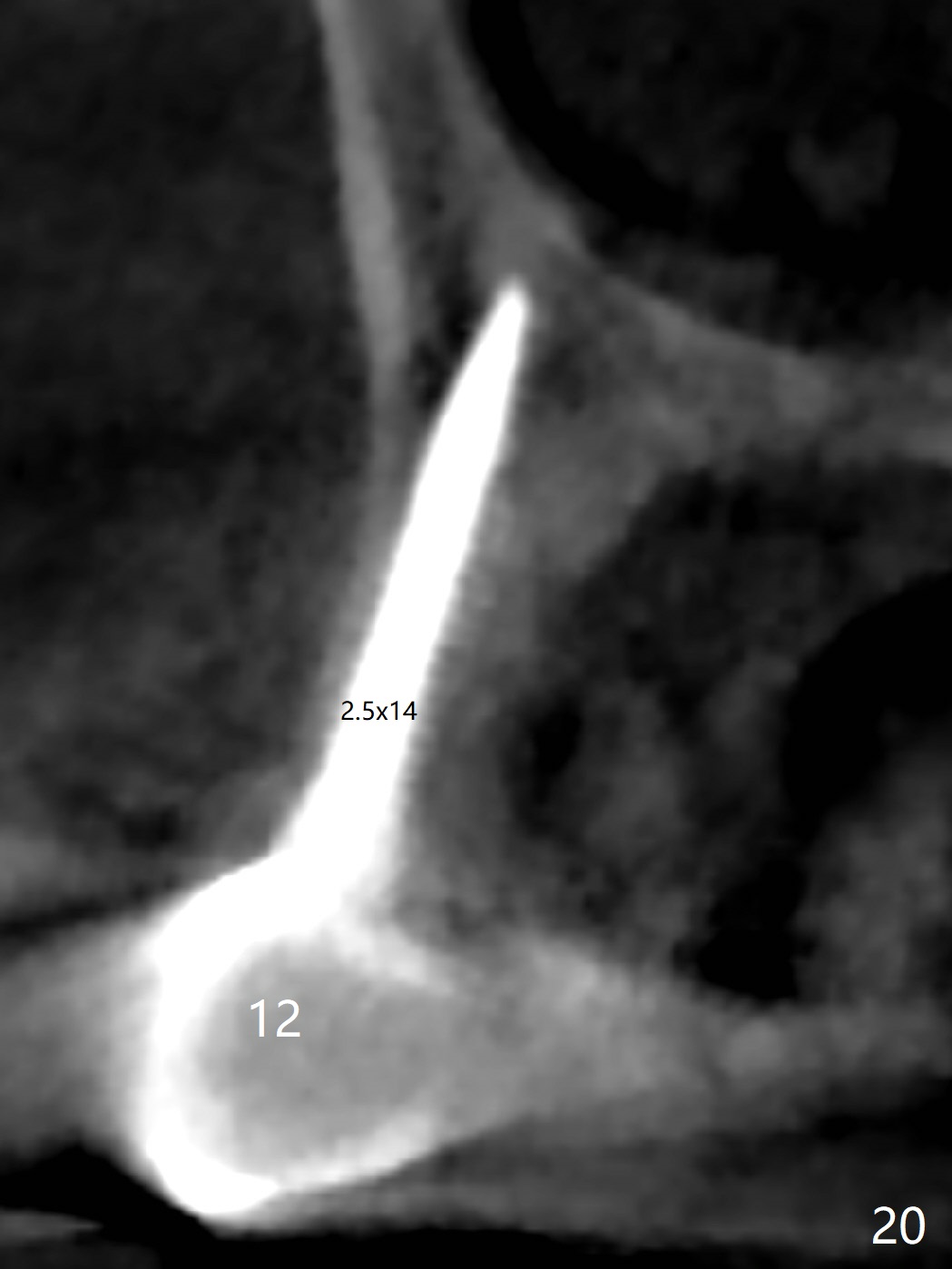
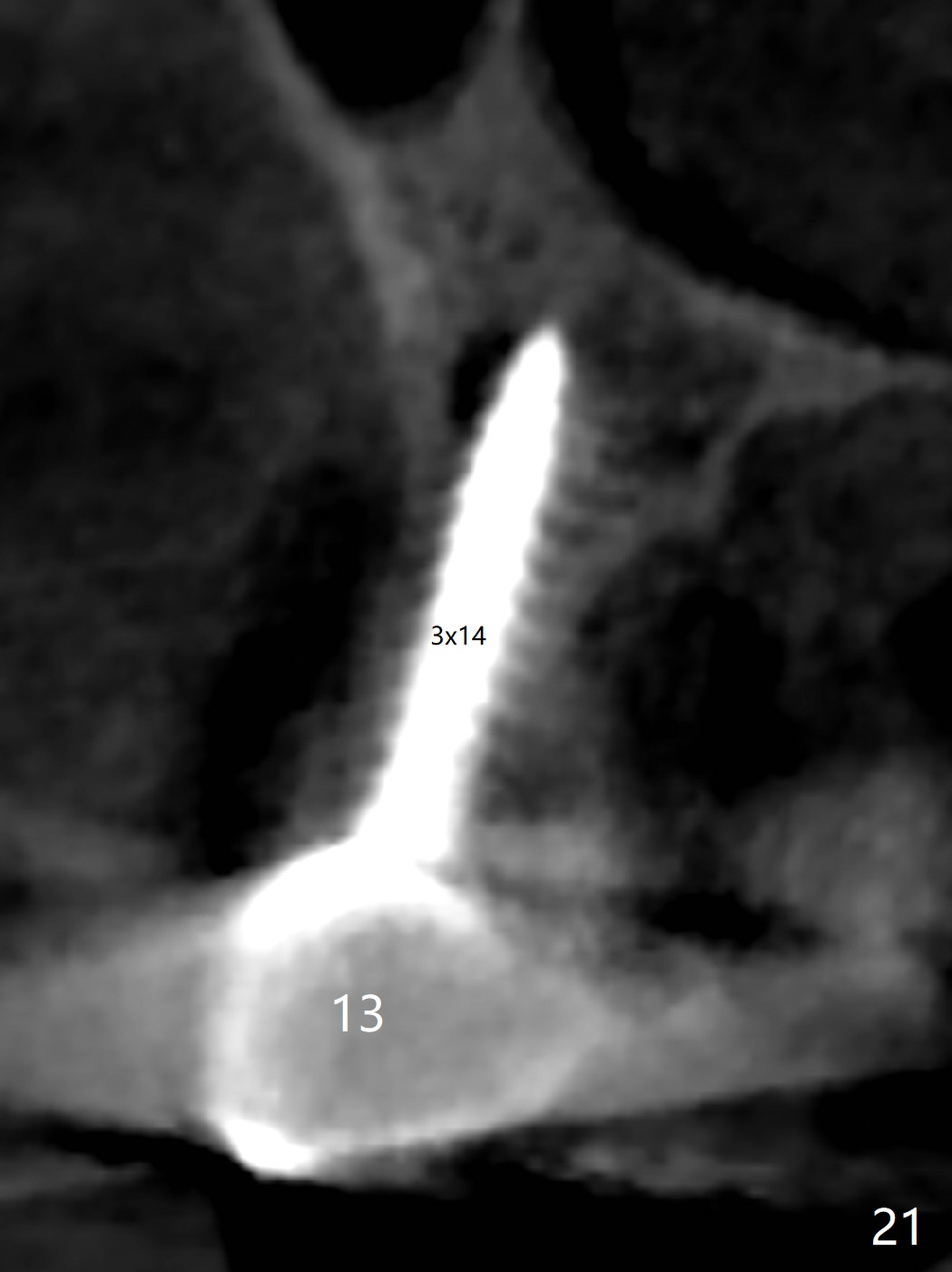
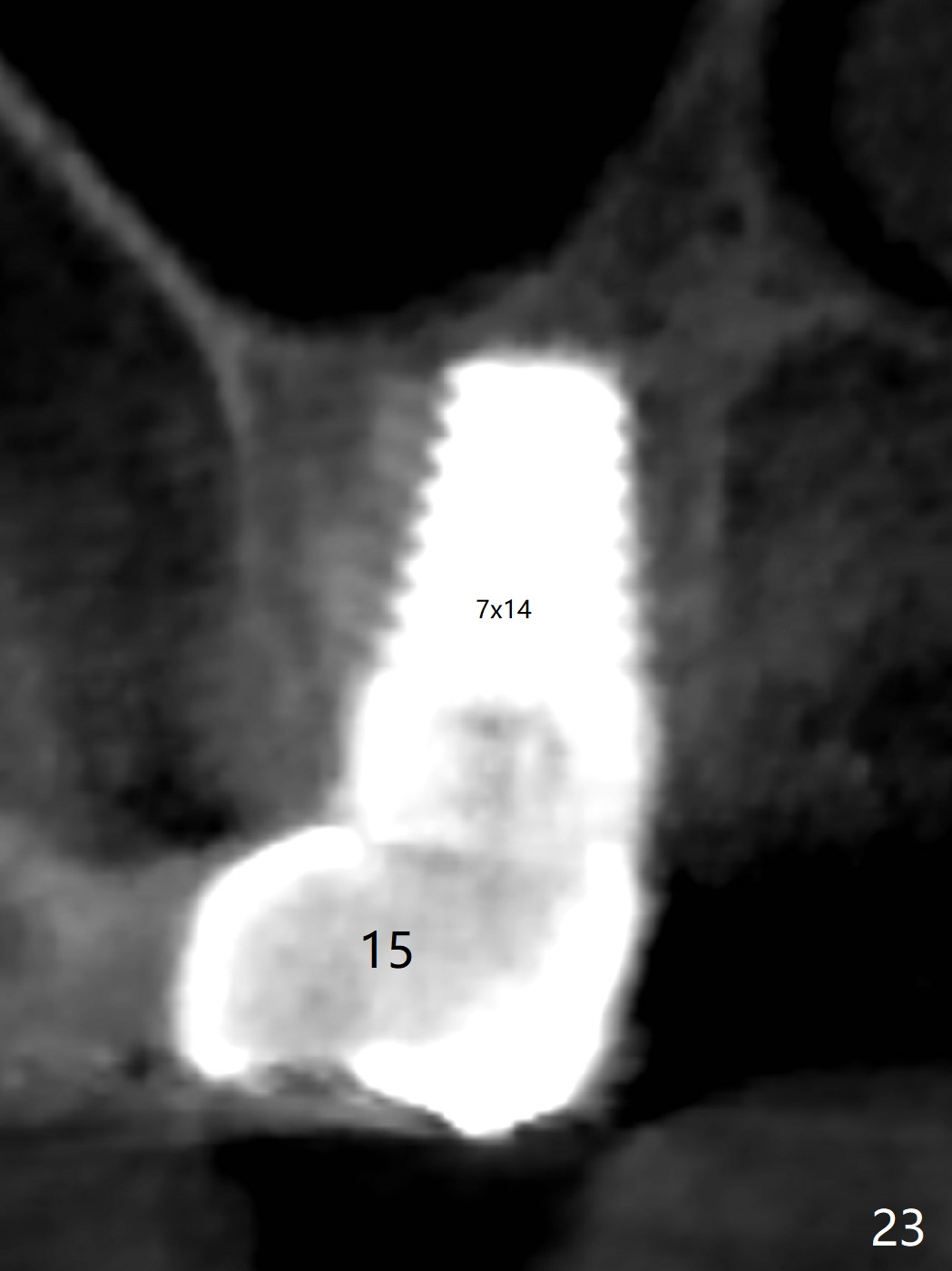
The crown at #11 dislodges 14 months post cementation probably due to distal placement of the implant and single unit, whereas the crowns at #12-14 are splinted (Fig.17). The gingiva and the buccal plate are healthy and non-atrophic (Fig.18). CBCT is taken 2 years 6.5 months post cementation (Fig.19-23).
Return to Upper Arch
Reconstruction with Implants,
Technicians,3,
26, Course 1
2
1-Piece
Xin Wei, DDS, PhD, MS 1st edition 10/11/2015, last revision 10/31/2018